
Zackary Sholem Berger's Blog, page 32
June 20, 2012
Quotidian Hypertopos
Such is the title of an exhibit of enlightening, unexpected juxtapositions: photographs by Jeremy Kargon of urban Chinese streetscapes, together with quotes by contemporary Chinese intellectuals. By each photo, unassumingly but evocatively, hangs a Mandarin playing card from a generation ago.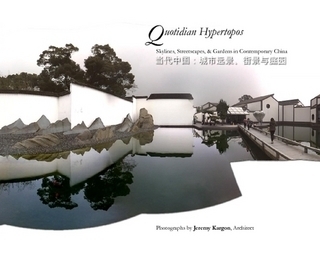
The exhibit is still catchable, and catch you must if you can, at Load of Fun. You can also buy the exhibit catalog which Kargon himself wrote and designed. I highly recommend it. Almost as much as I recommend another book he had a hand in…


June 18, 2012
Eating disorders in children: a review of clinical guidelines in Annals of Internal Medicine
Julie O’Toole, a Board certified pediatrician, has treated children, adolescents and young adults with eating disorders in a sub-specialty practice since 1998. She is the founder and medical director of Kartini Clinic, a pediatric clinic with inpatient, day treatment and outpatient care for children suffering from all conditions of disordered eating. I asked her to review the Annals of Internal Medicine In the Clinic feature on eating disorders. (She is also my aunt.)
This review article has many strong points and a few weak ones, particularly with regard to the pediatric population.
Risk. Females are at higher risk. In addition, the article highlights the importance of the family history. A first degree relative with anorexia nervosa confers a ten-fold increase in risk.
Weak points in the article’s discussion of screening are the recommendations for BMI screening. BMI can be deceptive. A child can start with a high BMI, lose a significant amount of weight, and wind up at a BMI that is still higher than average or well within the range of “normal,” falsely reassuring clinician and family.
Prevention. The authors dispel the illusion that anorexia nervosa, whose biophysiology hasn’t been elucidated and whose genetics is yet poorly defined, can be spoken of as being prevented. I agree however that early identification is critical, especially in children whose brains, bones and bodies are still being formed.
Diagnosis. This issue receives a great deal of attention. The new DSM-5 will bring substantial changes.
The older DSM-IV criteria are detrimental in pediatrics, where practitioners are tempted to either wait until age inappropriate DSM thresholds have been crossed or to use the unhelpful categorization “eating disorder not otherwise specified,” with insurance and triage repercussions. The most clinically useful suggestion the authors make, relevant to children, is to bypass psychological criteria (e.g. statements about being fat or being afraid to gain weight) in favor of “repeated failure to gain weight despite recommendation.” In childhood failure to gain weight can be as important as frank weight loss.
The physical exam, as the authors rightly emphasize, is more important than labs. Normal laboratory studies are little consolation to a clinician who has a cold, bradycardic, syncopal, cachetic patient. Not mentioned, however, is anosognosia or denial of the seriousness or even existence of the illness. The anosognosia of anorexia nervosa interferes more with successful treatment than medical compromise.
The American Academy of Pediatrics has hospitalization guidelines which have proven a boon to families who must access their insurance benefits for treatment of an eating disorder.
Where to treat. Anorexia nervosa has a mortality rate between 5-20%, with 10% a commonly given figure. This is comparable to the mortality from some types of childhood leukemia. Despite this, some practitioners are still reluctant to refer to specialists. Though the family may prefer that the generalist, whom they know and trust, manages their child’s eating disorder, this is not wise. These patients need time, which is lacking in a general practice! Even more than time, they need expertise and consistency of follow-up.
How to treat. Both cognitive behavioral therapy (CBT) and interpersonal therapy (IPT) have proven useful in the treatment of bulimia nervosa, but as the authors point out, there is little evidence for a robust effect of CBT or IPT in anorexia nervosa. In fact, a recommendation implied by the authors comes from pediatric eating disorder treatment: without weight restoration you will get nothing. Please do not follow a patient for more than a few weeks if they are not gaining weight consistently. At risk for the patient are the bones, the reproductive system, the brain, and meaningful social interaction.
Medication. Two very important points were made about medication, which should be shouted from the rafters: exogenous hormones do not help protect bones, and SSRI’s do not help in anorexia nervosa. Do not start the birth control pill to “jump start” periods, it doesn’t help their bones, and all it “jump starts” is cyclical withdrawal bleeding while imparting a false sense of normalcy.
Atypical antipsychotics have shown some use in anorexia nervosa, improving weight and cognition.
Pediatric treatment. A recommendation for family based interventions (FBT) is one I endorse. However, I am puzzled by the statement that a nutritionist should be included in any multidisciplinary team. Not only do we not use a nutritionist on our multi-disciplinary family-based treatment team, but the most widely known FBT programs in the country (Stanford University and the University of Chicago) do not use the services of a nutritionist either. The essential players in family-based interventions are the parents. Nutritional guidance can be provided in a family-based setting by specialist physicians and therapists working in collaboration with them.
Follow-up. The authors recommend frequent follow-up for any weight change. Many patients return to their home practice in good condition after a period of intense, often residential, treatment with everyone falsely reassured. Follow-up at monthly intervals is a disaster waiting to happen. Eating disorders in general and anorexia nervosa in particular are chronic illnesses; anosognosia means that external supervision and support is likely to be needed for an extended period of time.
June 15, 2012
What doctors are supposed to write
I had a patient* some time ago who, when I asked him how he was feeling, responded, “Pretty fucking awful.” He saw a copy of the note and was upset, not because he was ashamed of his language, but because he was taken aback that a doctor would use such language in a note. I explained to him that I always try to record what a patient says to me, since that conveys useful information. He was mollified.
*details changed to de-identify
June 11, 2012
Less is more in lower back pain…but what if the patient doesn’t agree?
Often, doctors and patients request unneeded tests out of either ignorance, inertia, or fear. Recently, I was part of the Good Stewardship Working Group of the National Physicians Alliance, which convened focus groups of different medical specialties to agree on “Top 5″ lists of procedures or tests which are medically contraindicated and can cause harm. This work was published in the Archives of Internal Medicine.
As a continuation to that work, we recently published a review in the Archives summarizing the reasons why requesting imaging (i.e., X-rays, CT scans, or MRIs) in routine cases of lower back pain without red flags is not a good idea, and quantifying the harm to the patient. Read it here.
Of course, the question outside the scope of the immediate article is this: what happens when the patient, against all recommendation, wants one of these imaging modalities anyway? Should the doctor do it or not?
This question attracts me because it makes things complicated. The interest of the patient comes into conflict with our interest. Do we respect the patient’s statement as it stands, do we encourage the development of a more knowledgeable approach to medical testing, or do we avoid the conversation with some appeal to insurance companies’ coverage criteria? 
In a useful review in JAMA, Brett et al. say: “Actively challenging patients’ requests for nonbeneficial interventions does not subvert properly understood respect for patient autonomy and is consistent with the professional obligation to practice high-quality, cost-effective medicine.” This is true enough. Challenging never subverts autonomy. But decision-making does. So what do we do when the rubber meets the road?
It’s not an easy question. What would you do in such a conflict, as doctor or patient?
June 5, 2012
Avoiding orthodoxy in understanding decision-making
The previous orthodoxy was paternalism. It’s my way, says the doctor, or the highway. The current orthodoxy – not stable yet but rapidly developing in that direction – is something called “patient-centered care.” Unfortunately, although we can define this term to our heart’s content, people tend not to read the textbook. What if a patient wants to be told what to do? What if a patient wishes to delegate all decision-making to their doctor, and the doctor thinks that’s not appropriate? What if a patient wishes to make all decisions themselves but clearly has no insight into their own health? Calling it “patient-centered care” solves none of these issues. 
What might help is to provide an instrument, like a survey, to a doctor before a patient’s first visit. Use this, we might say to a doctor, and you can help assess to what extent your patient wishes to be involved in decision-making. Or we might give this instrument to the patient. Then, even before the visit starts, we can know how paternalist, patient-centered, or something else either doctor or patient wish to be.
Those instruments don’t exist yet. Hey, let’s make them!
June 4, 2012
Between Paris and Williamsburg: I Am Forbidden, by Anouk Markovits
Originally posted on Unpious.net.
I Am Forbidden
By: Anouk Markovits
Hogarth, 320 pages
A man runs naked to the Aron Kodesh. A boy, after witnessing the slaughter of his family by the Romanian Iron Guard, is saved, to be raised as a Christian. In parallel: The Satmar Rebbe, in an open car, is within shouting distance of his Hasidim whom he does not or cannot save from extermination. This is national tragedy, theological failure.
It is the year 1939, in Maramures, Transylvania. 5-year-old Josef, his skullcap gone, his golden sidecurls shorn, is being raised by Fiorina, his family’s Christian maid. He has almost forgotten his Jewish origins when, several years later, he rescues a girl, Mila, whose parents are killed as they run to the Satmar Rebbe, whom they glimpse in an open train car. The rebbe will save them, they think, but instead the woman is shot; the man, still wearing his tefillin, is beaten to death in the town square. The Satmar rebbe, meanwhile, with aid from the Zionists, is on his way to safety in Switzerland.
Josef directs Mila to the home of a Satmar scholar, Zalman Stern, who later comes to retrieve Josef from his adoptive Christian mother and sends him on to yeshiva in Williamsburg, Brooklyn. The Sterns settle in Paris, and Mila remains with them, raised as a daughter — and as a sister to another girl, Atara. The two girls share everything at first but follow very different paths, both eventually intertwined with Josef’s: Mila is drawn to religious fervor, messianic redemption, and Bible study, while Atara asks herself, at first tentatively, if it is selfish to live and think as she wishes.
Despite the story’s foundation in tragedy and religion, this is not a Chaim Potok book full of disputation. We are face-to-face with people and the structures they create to deny death, bring the Messiah, or understand loss. When Josef is retrieved by Stern back to the Jewish world from Fiorina’s protection, we are given to understand the small tragedy they both live through in the shadow of a larger one, sharing a moment of “losing all, of having already lost”–a moment a lesser writer would have overlooked.
The inner lives of the punctiliously Orthodox, with their suppressed desire, menstrual obsession, and fear of death, coexist in the same book (and sometimes on the same page) as the deep joy and brilliant light of communal celebrations and Torah study. We feel the desire for Messiah in Mila, as we are moved by Atara’s yearning “to think gratuitous human constructs.” We teeter back and forth, not between Jerusalem and Athens, but between Paris and Williamsburg. Markovits brings off this balancing act with skill and daring. Everyone is given their due. Instead of disrespect or easy judgment, there is generosity of spirit and delicacy of the pen.
Chasidim make their way through these pages from Transylvania, to Paris, to Williamsburg. They are matched, marry, bear children. Some leave the fold. Stereotypes are avoided: There are Simchas Torah dances, but there is also the enchantment of a Paris library, Atara’s illicit haunt, where “lamps of milk glass inside green shells cast bright ellipses of light on rustling pages.” There is joy abounding with great-grandchildren aplenty, but there is also the pain of Mila who cannot conceive. At the center of the tale is her momentous decision that upends generations. Here, it should be said, the plot takes a baroque turn. Disbelief must be actively suspended — but this is not a misstep so much as an instance of ecstatic overreaching.
This is a different set of walls and courtyards than the familiar Brooklyn-Manhattan axis. The concreteness comes from the Maramureş wood nettle, the glowering statuary and blossoming gardens of Paris, the nighttime voyages by rail. Because Markovits is French born — having published one novel in that language already — we get the Chasidic world of the United States viewed from across the Atlantic. In Paris, the Stern children are called sale juif, dirty Jew. In Brooklyn there is “kosherness splashed all over…Jews not afraid to advertise they [are] Jews, Jews reconstructing a world that never was before.”
As creator of this microcosm, Markovits’ most impressive feat of compression is to present two great moral questions in concrete Jewish terms that can resonate with any intelligent reader. The more familiar of these is the Holocaust. “Does the Lord stay to watch,” asks Atara, a skeptic even in seminary, “when children are burning?” It is a credit to the novel and its characters that even the director of the girls’ seminary of whom this question is asked does not have the chutzpah to answer it immediately.
The more difficult question involves repercussions of individual decisions, whether a community can judge violators by its own lights. In the Jewish terms of Markovits’ plot: how do you solve the problem of the mamzeres and her descendants? How can deceit be assimilated into the stories a family tells about itself? Are there boundaries that can be crossed, and then crossed back again in the other direction — keeping what was learned on the outside while finding a place at the Shabbos table? There are answers here, but the story, its characters, and the created world are primary.
This is a book absorbing as any midrash and as enlightening as a library. I feel its contribution immediately and powerfully, and am happy to have given my time to it. I recommend you do the same.
May 30, 2012
Bridging uncertainty and action
Medicine is always uncertain because evidence is always incomplete. The bridge between this incompleteness and the decisions that must be made is the preference of the patient in discussion with their physician. No insightful care can make believe this bridge doesn’t exist, that evidence is somehow complete and easily applied without the thoughts and wishes of the patient and physician themselves. 
May 25, 2012
Final sefirah-haikus: Malchus (To the Throne!)
Thieved
It’s not the bandits’
fault, and it’s not the road.
Your unrest – you fool.
The last stage
What to take along?
The gold of the calf? Or the
fragmented tablets?
Resting
Look! The whole people
Is resting at the mountain.
Some of them hatless!
Traffic jam: Shvues
The throne of glory:
Impossible to push through
All the suckers-up.
Some advice please
Another question:
If you approach the throne, do
you wear sunglasses?
Fear
I am really scared
That all the best words are too
Simple.
The end of things
Finally it’s you
Who have to add your two words
To the Torah’s tail.
May 24, 2012
Rabbi Simchah Roth z”l
I was certainly not the only one to be shocked by the news of the death of Rabbi Simchah Roth z”l. I never knew him, but I felt like I spoke to him every week. For years I subscribed to his email Mishnah shiurim, available in Hebrew and English. Clear, careful, idiomatic, without an ounce of cant, ideology, or hubris, these were what shiurim should be – and a true tikkun for the Internet. [image error]
The last email I got from him (together with thousands of others) finished his shiur on Tractate Sukkah. It ended this way, in Hebrew:
סוף כל סוף סיימנו את לימוד מסכת זו בשטו”מ. כעת אני עושה פסק זמן לפני שנתחיל ללמוד את המסכת הבאה. כפי שהסברתי בשיעור הקודם, אני עובר כרגע תקופה של בריאות לקויה ויש לי הרבה תורים אצל רופאים למיניהם ובמרפאות למיניהן לבדיקות. אני מעדיף לחכות עד שכל הטיפולים האלה יושלמו לפני שאתחיל בלימוד מסכת חדשה. תודה על הסבלנות וההתחשבות. כשתבוא העת אשלח דוא”ל. בהזדמנות זו אני מאחל לכולם חג פסח כשר ושמח.
It’s appropriate to acknowledge Rabbi Roth’s Torah as we enter into Shavuot.
May 23, 2012
Death, Duty, Def Leppard: Three Poets and an Essayist at Normal’s in Baltimore
The poetry reading at the bookstore was called for 7:30, but when I got there people were still milling around. To occupy myself, I bought a slim paperback of Kant for 5 dollars. He talked a lot about the duty of morals and the human will, but it seemed a grim duty with very little love and a lot of law. At 8:10, someone murmured, “Maybe we should get started.”
First, Karen Rivers Hattrup read an essay, a sweet memento-mori about the transience and beauty she found as a guest at a Catholic girls’ high school dance: “the girl who had cancer and lived, the girl who had cystic fibrosis and did not.”
Jennifer Fortin, who grew up in Gaithersburg and went to Goucher, read work from her 2011 book Miner Muzzle Velocity. This is a collection of postcard-shaped poems written from a narrator, somewhere abroad, to her lover-friend-recipient, addressed only as “Dear.” Each is signed “Yrs.” and each, like a postcard, wends its way in a confined space while referring to the world outside in either oblique or explicit ways. The writer is always on the road, scribbling on the fly while connecting to her correspondent. “On the road again, Dear. Decide on stakes.”
Then came Nate Pritts, who dedicated some of his work to Def Leppard. So is Nate’s work stadium rock poetry, wearing its heart on its sleeve and demanding to be sung? Sure:
Sure:
Give thanks for what’s beautiful and the fact that it ends
I’m hot with the duty to build it again
That’s the duty we need, that’s what Kant is missing! This is the poet-philosopher: “The assumption we can define the way our surroundings continue/after our absence/is the ultimate arrogance.”
The evening’s host, Jeremy Hoevenaar, read last. A recent chapbook of his is available for free on the website of H_NGM_N, Pritts’s journal. There’s witticism – “You’re not in time. You’re too late. You missed it./ God’s not only dead, he’s completely decomposed.” There is Lucretianism: “Following a series of repeatedly failing gestures,/I hit upon the idea of addressing atoms individually.” In many of these poems, there is also love, disintegration, and anatomy.
To take some of Hoevenaar’s words out of context – the reading was both “a historical moment and an object of entertained fascination.” Let’s build it all again.


