
Zackary Sholem Berger's Blog, page 34
April 25, 2012
How doctors decide
I hope to write regularly on doctors’ decision-making. This first installment concerns types of evidence-based studies. Later, I will talk about how and whether doctors actually use such evidence to make decisions.
There are a number of kinds of evidence-based advice which doctors can use to make decisions. The differences among them are instructive.
1. Individual journal articles. These can present findings from a single trial. The potential biases are multiple. Not all findings get published (publication bias – i.e. we never find out about the results which do not support the hypothesis). Many results are never reproduced. To quote one widely read study, “studies that report positive or significant results are more likely to be published and outcomes that are statistically significant have higher odds of being fully reported.” Some studies have to be retracted later by the journal which publishes them.
2. Reviews. These can be of many kinds. A narrative review recounts in a summary form the findings of a number of articles. The summary is susceptible to bias from many factors: which articles are chosen, what emphases are given, which author is doing the review. For that reason, some people prefer a –
3. Systematic review. This combines research articles on a given topic according to strict definitions made a priori. Then the results from these individual articles are combined only if they are comparable, i.e. applying to the same population or disease. Some of the time individual results can be merged in a statistical way, called a meta-analysis. I work on a number of these; they have their own problems (the link is from an orthodontics journal but the issues are generally applicable).
4. Guidelines. Using the above reviews, a group of experts, often physicians, draft official recommendations for a given disease, group of diseases, or use of a given medication or procedure. But guidelines are only as good as the evidence they are based on, the applicability of the guidelines to the particular question that is being considered — is the patient from the population that was studied? is the clinical condition the same? — and any bias that might have affected the results.
To take one example of a well-done review, the American Academy of Neurology and the American Headache Society recently published Evidence-based guideline update: Pharmacologic treatment for episodic migraine prevention in adults. Even such a guideline, however, comes with weaknesses. For some of these we can quote the authors: while good-quality evidence does support the effectiveness of certain medications for treating migraines, “evidence is unavailable to help the practitioner choose one therapy over another.”
Another sort of weakness was also reported by these authors, but in a different way, in an often-ignored paragraph at the end of the article. For those that can’t read the small type, these are disclosures of possible conflicts of interest. Nearly all the authors have received honorariums from a number of pharmaceutical companies. I don’t think this completely obviates the recommendations, but it might if we look closely enough. This is why, to my way of thinking, any such guidelines need to be either free of conflict of interest or ensure balanced COIs within the writers.
Dr. Silberstein is on the advisory panel of and receives honoraria from AGA, Allergan, Amgen, Capnia, Coherex, Colucid, Cydex, GlaxoSmithKline, Lilly, MAP, Medtronic, Merck, Minster, Neuralieve, NINDS, NuPathe, Pfizer, St. Jude Medical, and Valeant. He is on the speakers’ bureau of and receives honoraria from Endo Pharmaceuticals, GlaxoSmithKline, and Merck. He serves as a consultant for and receives honoraria from Amgen and Novartis. His employer receives research support from AGA, Allergan, Boston Scientific, Capnia, Coherex, Endo Pharmaceuticals, GlaxoSmithKline, Lilly, MAP, Medtronic, Merck, NINDS, NuPathe, St. Jude Medical, and Valeant Pharmaceuticals. Dr. Holland (formerly Dr. Pearlman) receives consulting income from Map Pharmaceuticals and the American Headache Society and research support from Albert Einstein College of Medicine. Dr. Freitag has served on the scientific advisory boards of Zogenix Pharmaceuticals, Allergan Pharmaceuticals, Nautilus, MAP Pharmaceuticals, and Nupathe; has received travel expenses and or honoraria from GlaxoSmithKline, Zogenix, Merck, Nautilus, Allergan, Diamond Headache Clinic Research and Educational Foundation (not for profit), and the American Headache Society (travel). Dr. Freitag is a member of the Board of Directors of the National Headache Foundation. Dr. Dodick, within the past 3 years, serves on advisory boards and has consulted for Allergan, Alder, Pfizer, Merck, Coherex, Ferring, Neurocore, Neuralieve, Neuraxon, NuPathe Inc., MAP, SmithKlineBeecham, Boston Scientific, Medtronic, Inc., Nautilus, Eli Lilly & Company, Novartis, Colucid, GlaxoSmithKline, Autonomic Technologies, MAP Pharmaceuticals, Inc., Zogenix, Inc., Impax Laboratories, Inc., Bristol Myers Squibb, Nevro Corporation, Atlas, Arteaus, and Alder Pharmaceuticals. Within the past 3 years, Dr. Dodick has received funding for travel, speaking, or editorial activities from CogniMed, Scientiae, Intramed, SAGE Publishing, Lippincott Williams & Wilkins, Oxford University Press, Cambridge University Press, Miller Medical, Annenberg for Health Sciences; he serves as Editor-in-Chief and on the editorial boards of The Neurologist, Lancet Neurology, and Postgraduate Medicine; and has served as Editor-in-Chief of Headache Currents and as an Associate Editor of Headache; he receives publishing royalties for Wolff’s Headache, 8th edition (Oxford University Press, 2009) and Handbook of Headache (Cambridge University Press, 2010). Within the past 3 years, Dr. Dodick has received research grant support from Advanced Neurostimulation Systems, Boston Scientific, St Jude Medical, Inc., Medtronic, NINDS/NIH, Mayo Clinic. Dr. Argoff has served on a scientific advisory board for the Department of Defense and DSMB for the NIH; has received funding for travel and/or speaking and/or has served on a speakers’ bureau for Pfizer (King), Janssen (Pricara), Millennium Laboratories, Neurogesx, Forest Laboratories, Eli Lilly, Covidien, and Endo Pharmaceuticals; has received research support from Endo Pharmaceuticals, Forest Laboratories, Eli Lilly, Neurogesx, Pfizer, and SBRT funded by the NIH; and has received stock/stock options from Pfizer. Dr. Ashman is the Level of Evidence editor for Neurology and serves on the AAN Guideline Development Subcommittee. He reports no other disclosures. Full disclosures were provided at the time of Board approval. Go to Neurology.org for full disclosures.


April 24, 2012
Room of care
Wall talks to wall. One has a clock, the other a window, the third a cupboard with bandages etcetera. The fourth a door that opens and closes a thousand times a day.
Chair is across from chair. Occasionally the one looking for care picks the wrong one to sit in, and there is a dance for two chairs and two people till the problem is sorted out.
Tile borders ceiling tile. There is nothing to look at, lying there, but ceiling, and after a while I begin to see faces, continents, games, riddles.
April 23, 2012
Sefirah haikus: tifereth
Beat head on wall. Stop.
How are you supposed to take
pity on yourself?
Take Your Only…
Mine is a daughter.
The very same mountain, but
she’ll know what’s doing.
Pursuer of Peace
slips on his compromises
falls and breaks his neck.
Sunset’s loveliness
Exchanged now for the sunrise -
Just one loveliness.
Blindness comes from light.
From darkness – the eyes become
again light-ready.
Yom Haatzmaut
As long as heart beats-
there should be the effort, too
to make dreams better.
We’ve almost arrived
- finally – at the longed for
planned towards
middle.
April 19, 2012
Some ways to remember
In 2004, I laid out some ways in which I have tried to remember the Holocaust: narrative, history, and prayer.
April 17, 2012
Becoming someone else
I saw a patient of mine this week: someone he loved died. He said, “I felt like I went to bed one day and got up the next day a different person.”
I wonder whether he’ll be happy someday as that new person. Or if that new person, to be authentic, must always have that pain. If the latter is true, to make it better would be a lie.

Creative Commons image by theilr
April 16, 2012
Sefirah haikus: Gevurah
To Volcano, with esteem
From a scorching cra-
-ter, a curl of smoke points up,
up-up-up-upward!
The tree of the field
A bang. A bang.
Bang. A chop. A saw. The tree
doesn’t care to fall.
Waiting
Brilliant now, the
buried bones. But just wait for
what’s from the dry bones.
Or just zitsfleisch…
Wait forever, if
necessary, for the illed-
out moment. Amen.
Yom HaShoah
The bed/coffin swings
empty. Those that are made ash –
can they be buried?
Creation
 So hot! Orange soda
So hot! Orange soda
– the Shechinah — bubbles
on ice cream. Shehakol.
Sefirah Style
The hair left to grow.
Animals: winter. In us
this estivation.
April 9, 2012
Sefirah Haikus: Chesed
A few years ago, on my old blog, I posted a series of sefirah haikus. Here there are again, somewhat modified, for your counting pleasure. I will post seven of these weekly until Shavuot. The Yiddish version is available on this blog, too, over on the other side of the mechtizah.
This first week's sefirah is chesed.

Yellow, white to spite
the begrudging day. Do not
hold yourself back, now.
When I give, the I's
not lessened but strengthened – when
I hold back, it falls.
I'm braggy about
my serious piety.
Prayer works with me.
But my love for him
did not demean him. He can
resist everything.
Under the throne of
glory, there's a neon sign:
Danger! Do not touch!
Multiplicative
power floods every limit.
Death also begets.
With your two yetzers.
You say you have a thousand?
He has an Ain-Sof.
April 5, 2012
In which I channel Mark Strand
In a field
I'm not one of
the cows.
This is
always the case.
For all x not equal to me
I am not x.
More at qarrtsiluni.
April 4, 2012
Choosing Wisely: looking forward to hearing your thoughts!

Nine United States specialty societies representing 374,000 physicians developed lists of "Five Things Physicians and Patients Should Question" in recognition of the importance of physician and patient conversations to improve care and eliminate unnecessary tests and procedures. These lists represent specific, evidence-based recommendations physicians and patients should discuss to help make wise decisions about the most appropriate care based on their individual situation
April 2, 2012
So very special
This wouldn't be so confusing if I had thought about what specialists and general practitioners are each supposed to do. But I have no such a priori understanding. I send a patient to a specialist, and my thought is something like this:
"Gee, I hope they pursue a self-limited course of diagnosis and treatment based on the clinical question I have in mind!"
And the patient, on the other hand, thinks something like:
"Dr. Berger wants Dr. Gutskener to figure out why my belly hurts."
Dr. Gutskener, on the other hand, possesses a treasure of expertise around the gastrointestinal tract, and doesn't generally feel his role to be limited in the sense Dr. Berger (me) is thinking of. He takes "limited" to mean "within a given subspecialty" – he does GI, not neurology or cardiology. But within GI, he is taking care of the patient referred to him as best he knows how, and that does not mean a minimal approach.
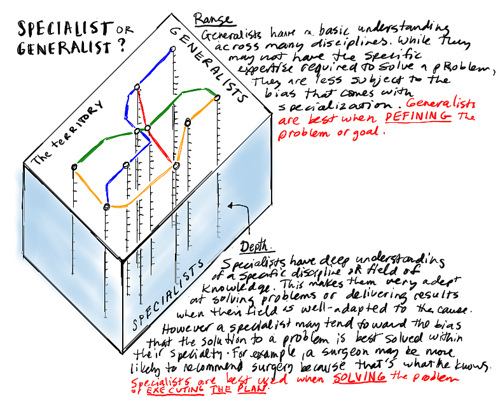
Graphic by Dave Gray
At some point, telling a specialist not to further test and treat a patient is like Ronald Reagan trying to recall a missile that has already been launched by submarine. But I have had patients where I would like to email the specialist and say, politely, Stop!


