
Jeffrey Dach's Blog, page 5
July 18, 2024
The Failure of Cholesterol Lowering Drugs
The Failure of Cholesterol Lowering Drugs by Jeffrey Dach MD
Click here for Cholesterol lowering Drugs in the Elderly, Bad idea
This new article will be ready in a few days, don’t forget to check back.
warmest regards,
Jeffrey Dach MD
References:
1) Krumholz, Harlan M., et al. “Lack of association between cholesterol and coronary heart disease mortality and morbidity and all-cause mortality in persons older than 70 years.” Jama 272.17 (1994): 1335-1340.
2) Criqui, Michael H., and Beatrice A. Golomb. “Low and lowered cholesterol and total mortality.” Journal of the American College of Cardiology 44.5 (2004): 1009-1010.
3) Petersen, Line Kirkeby, Kaare Christensen, and Jakob Kragstrup. “Lipid-lowering treatment to the end? A review of observational studies and RCTs on cholesterol and mortality in 80+-year olds.” Age and ageing 39.6 (2010): 674-680.
4) He, Guo-dong, et al. “A nonlinear association of total cholesterol with all-cause and cause-specific mortality.” Nutrition & metabolism 18 (2021): 1-11.
5) Wu, Wanqing, et al. “Low and High-Density Lipoprotein Cholesterol and 10-Year Mortality in Community-Dwelling Older Adults: The Shanghai Aging Study.” Frontiers in medicine 9 (2022): 783618.
https://esmed.org/MRA/mra/article/dow...
6) Ravnskov, Uffe, and Kilmer S. McCully. “The importance of LDL-cholesterol and infection in the etiology of cardiovascular disease: a meta-analysis of COVID-19 survivors and non-survivors.” Medical Research Archives 12.5 (2024).
!!!!!!!!!!!!!!!!!!! BEST !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
7) Sloop, Gregory D., et al. “Flawed reasoning allows the persistence of mainstream atherothrombosis theory.” Cureus 10.3 (2018).
Despite 60 years of study and an investment of billions of dollars, the rate of deaths due to coronary artery disease is increasing in the United States and in all other countries except the lowest socio-demographic populations worldwide (Figure (Figure1,1, Figure Figure2)2) [4].
Deaths due to heart disease increased by 3% in the US between 2014 and 2015, the latest years for which data are available [5]. Clearly, lipid theory is not powerful enough to provide the insight necessary to control atherothrombosis.
Popper also wrote “It is easy to obtain confirmations, or verifications, for nearly every theory—if we look for confirmations” [23]. Thus, in the scientific method as conceptualized by Popper, a theory can only be disproved, not proved. No number of confirmations can ever prove a theory.
Popper’s work sheds light on studies of statin therapy. While statins have been shown to reduce morbidity and mortality from atherothrombosis in some studies, DuBroff’s work shows that they have failed in a substantial number of studies despite significantly decreasing LDL levels. This failure falsifies the theory that elevated LDL or cholesterol is the cause of atherothrombosis.
Clinical trials of antioxidant vitamins and immunohistopathology refute oxidation theory. Immunohistopathology shows that oxidized LDL does not cause monocyte chemotaxis, cytotoxicity, or apoptosis as suggested by in vitro studies [27]. The persistent belief in the role of chronic oxidative stress in atherothrombosis can be attributed to the dominance of lipid theory and non-falsifiable defense of the oxidation hypothesis. After refutation in clinical trials, two prominent proponents of the oxidation hypothesis wrote:
“The hypothesis that oxidative modification of LDL plays a significant role in atherogenesis in humans is not necessarily disproved by the failure of these particular clinical trials any more than a negative trial of an ineffectual antibiotic in Pneumococcal pneumonia would prove that pneumonia is not a bacterial disease. The oxidative modification hypothesis is not that vitamin E will ameliorate the human disease but that oxidative modification of LDL and/or other oxidative events play a significant role in human atherogenesis as it does in animal models of atherogenesis. A corollary of the hypothesis is that some appropriate antioxidant intervention, at some appropriate dosage, in appropriately selected patients over an appropriate time interval has the potential to improve prognosis [28].
This paragraph contains numerous non-falsifiable statements meant to prevent refutation of oxidation theory, which is an ad hoc modification of lipid theory.
Oxidation theory is an ad hoc modification made necessary when it was shown that uptake of cholesterol by the LDL receptor was insufficient to form a macrophage foam cell because of negative feedback. However, chemically-modified LDL can be taken up by the scavenger receptor in sufficient quantities to create a foam cell. Oxidation theory has been refuted as discussed above.
The “weight-of-evidence fallacy” refers to the belief that the majority of evidence determines truth. This fallacy is widely used to support lipid theory, even appearing in the title of lipidologist Daniel Steinberg’s defense of lipid theory, The Cholesterol Wars: Cholesterol Skeptics vs. the Bulk of Evidence. This fallacy is also seen in the following quotation:
“The suggestion that the ‘limited success of cholesterol-lowering therapy in numerous prospective randomized controlled studies, some of which show significant decreases in serum LDL cholesterol but no improvement in outcome’ refutes the causal effect of LDL on the risk of ASCVD [atherosclerotic cardiovascular disease] is not a quantitatively literate argument. Instead, a synthesis of the totality of the evidence … provides overwhelming quantitative evidence that LDL causes ASCVD… [32].”
Regarding the weight of evidence fallacy, Skrabanek and McCormick wrote:
“Such an approach to establishing truth is nonscience: not only is it nonscience; it is also dangerous, because reasoning of this sort may lead to action that (particularly in the field of preventive medicine) can touch many people’s lives [31].” The danger of accepting lipid theory is that it makes the search for a better theory unnecessary.
Conclusions
In spite of extensive investigation into the role of lipids in atherothrombosis, the disease is not controlled and death rates are increasing around the globe. This failure is due to shortcomings of lipid theory. Lipid theory is incomplete because it does not explain the majority of cases of atherothrombosis. The theory that hypercholesterolemia is the cause of atherothrombosis and the theory that atherothrombosis is an inflammatory disease are examples of inappropriate extrapolation. These theories are special cases of the general theory that increased viscosity accelerates atherothrombosis by fostering mural thrombosis. Control of atherothrombosis will require that lipid theory is superseded by a superior theory.
————
8) Sloop, Gregory D., et al. “Apolipoprotein (a) is the Product of a Pseudogene: Implications for the Pathophysiology of Lipoprotein (a).” Cureus 10.5 (2018).
Lipoprotein(a) [Lp(a)] is a particle composed of a core which is indistinguishable from that of low density lipoprotein (LDL) and a single molecule of apolipoprotein(a) [apo(a)]. Lp(a) is clinically significant because it is a risk factor for accelerated atherothrombosis as well as arterial and venous thrombosis.
Rather, Lp(a) (and LDL) accelerate atherothrombosis by increasing blood viscosity. The most effective intervention for elevated levels of Lp(a), therapeutic apheresis, works by decreasing blood viscosity. In areas where this intervention is not available, therapeutic phlebotomy or blood donation are alternatives.
—————————-
*********************************************************
!!!!!!!!!!!!!!!!!!!!!!!!!!!!! BEST !!!!!!!!!!!!!!!!!!!
**********************************************************
New Non-statin cholesterol drugs
Click to access f3d1aae01e08d46caf5f91f7b2ab83019a46.pdf
Rabaeus, Mikael, and Michel de Lorgeril. “A Systematic Review of Clinical Trials Testing CETP and PCSK9 Inhibitors: The Cholesterol-Heart Theory—Time for a Requiem?.” Journal of Controversies in Biomedical Research 5.1 (2019): 4-11.
despite a very significant effect on cholesterol levels, the CETP and PCSK9 inhibitors have not been shown to diminish the frequency of clinical events in high-risk patients, especially not the important ones represented by total and cardiovascular deaths.
Another consequence of these findings is that they speak strongly against the cholesterol-heart theory, confirming the doubts that have already been raised by a large group of scientists all over the world. As this theory leads to millions of people taking statin drugs, it appears highly necessary that access to raw data of all statin trials be allowed so as to reappreciate them. This is an important aspect considering the very strong conflicts of interest that the majority of scientists present, all the more concerning as many of these scientists exercise official activities in Association boards and guidelines committees and in medical journals. Therefore, we continue to maintain that the cholesterol-heart theory should be seriously challenged.
==========================
44 randomised controlled trials (RCTs) of drug or dietary interventions to lower LDL-C in the primary and secondary prevention literature, which show no benefit on mortality [8]
Demasi, Maryanne, Robert H. Lustig, and Aseem Malhotra. “The cholesterol and calorie hypotheses are both dead—it is time to focus on the real culprit: insulin resistance.” Pharmaceutical Journal (2017).
For instance, there are 44 randomised controlled trials (RCTs) of drug or dietary interventions to lower LDL-C in the primary and secondary prevention literature, which show no benefit on mortality [8] . Most of these trials did not reduce CVD events and several reported substantial harm. Yet, these studies have not received much publicity. Furthermore, the ACCELERATE trial, a recent well-conducted double-blind randomised controlled trial, demonstrated no discernible reduction in CVD events or mortality, despite a 130% increase in high-density lipoprotein cholesterol (HDL-C) and a 37% drop in LDL-C. The result dumbfounded many experts, sparking renewed scepticism about the veracity of the cholesterol hypothesis[8] .
[8] DuBroff R. Cholesterol paradox: a correlate does not a surrogate make. Evid Based Med 2017;22(1):15–9.
The global campaign to lower cholesterol by diet and drugs has failed to thwart the developing pandemic of coronary heart disease around the world. Some experts believe this failure is due to the explosive rise in obesity and diabetes, but it is equally plausible that the cholesterol hypothesis, which posits that lowering cholesterol prevents cardiovascular disease, is incorrect. The recently presented ACCELERATE trial dumbfounded many experts by failing to demonstrate any cardiovascular benefit of evacetrapib despite dramatically lowering low-density lipoprotein cholesterol and raising high-density lipoprotein cholesterol in high-risk patients with coronary disease. This clinical trial adds to a growing volume of knowledge that challenges the validity of the cholesterol hypothesis and the utility of cholesterol as a surrogate end point. Inadvertently, the cholesterol hypothesis may have even contributed to this pandemic. This perspective critically reviews this evidence and our reluctance to acknowledge contradictory information.
Rudolf Virchow first described the microscopy of the atherosclerotic plaque, but Nikolay Anichkov is credited with elucidating the central role of cholesterol in atherosclerosis.
Ironically, cholesterol is also essential for life as a key component of cell membranes, steroid hormones and bile acids.
Table 1 lists 44 cholesterol-lowering RCTs that reported no mortality benefit. Most reported no reduction in CV events, and several reported substantial harm (CDP, HERS, Minnesota Coronary Experiment, Sydney Diet Heart Study, WHI, WHO). This lack of benefit was seen even with profound reductions in LDL cholesterol (50% in the Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) trial). Although several studies were not pecifically designed to assess mortality, the reported lack of mortality benefit should not be disregarded…While some experts have dismissed or criticised these negative trials, the totality of evidence simply cannot be ignored. Even when researchers demonstrate a statin mortality benefit, the findings are underwhelming. A recent analysis concluded that statins would only postpone death by a median of 3.1 and 4.2 days for primary and secondary prevention, respectively.6
DuBroff, Robert. “A reappraisal of the lipid hypothesis.” The American Journal of Medicine 131.9 (2018): 993-997.
Regrettably, some clinical trials prior to 2004 have been tainted by scandals that led to new clinical trial regulations intended to safeguard patients and lend credibility to subsequent trials.3, 4
The table summarizes 29 major RCTs of cholesterol reduction reported after the publication of these regulations (Table). Notably, only 2 of these 29 studies reported a mortality benefit, while nearly two-thirds reported no cardiovascular benefit at all. These unfavorable outcomes and inconsistent results suggest that the lipid hypothesis has failed the test of time.
———————- –
DuBroff, Robert, Aseem Malhotra, and Michel de Lorgeril. “Hit or miss: the new cholesterol targets.” BMJ Evidence-Based Medicine 26.6 (2021): 271-278.
The new guidelines recommend three classes of drugs for cholesterol reduction:
β-Hydroxy β-methylglutaryl-CoA (HMG-CoA) reductase inhibitors (statins), cholesterol absorption inhibitors (ezetimibe) and proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9…It is noteworthy that a beneficial reduction in cardiovascular events was seen with LDL-C reductions as little as 11%–15% in Aggressive Lipid-Lowering Initiation Abates New Cardiac Events (ALLIANCE) and Management of Elevated Cholesterol in the primary prevention Group of Adult Japanese (MEGA), while a lack of cardiovascular benefit was seen with LDL-C reductions as great as 50% or more in Evaluation of Cardiovascular Outcomes After an Acute Coronary Syndrome During Treatment With Alirocumab (ODYSSEY FH 1 and 2), Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) and Studies of PCSK9 Inhibition and the Reduction of Vascular Events (SPIRE 1 and 2).5–9
Limitations of LDL-C as a treatment target
Because of the putative role of LDL-C in the pathogenesis of ASCVD, it seems intuitive and logical to target LDL-C to prevent cardiovascular disease. Indeed, there is much evidence to support this approach. However, decades of RCTs of LDL-C reduction have failed to demonstrate a consistent benefit.19 Conspicuous by its absence in the AHA/ACC guidelines is any endorsement of niacin or cholesteryl ester transfer protein (CETP) inhibitors, agents with a proven track record of reducing LDL-C but failing to consistently save lives or prevent cardiovascular disease.20 21 To validate the theory that reducing LDL-C reduces the risk of cardiovascular disease (the lipid hypothesis), LDL-C lowering interventions must be efficacious. Considering that dozens of RCTs of LDL-C reduction have failed to demonstrate a consistent benefit, we should question the validity of this theory.22
In this analysis over three-quarters of the cholesterol lowering trials reported
no mortality benefit and nearly half reported no cardiovascular benefit at all.
In most fields of science the existence of contradictory evidence usually
leads to a paradigm shift or modification of the theory in question,
but in this case the contradictory evidence has been largely
ignored simply because it doesn’t fit the prevailing paradigm.25 26
there was no mortality benefit in roughly three-fourths of the trials, and nearly half reported no significant reduction in cardiovascular events. According to his analysis, some of the trials that reported the greatest drop in LDL-C among participants demonstrated no accompanying cardiovascular benefit. But in other trials where LDL-C levels dropped only modestly, there was a robust reduction in cardiovascular risk. “The cause of atherosclerosis is far more complex than we originally thought,” DuBroff says. “But our LDL-centric approach to preventing cardiovascular disease may have distracted us from investigating other mechanisms and treatments.”
————————————————————-
Proto Magazine Cholesterol Deniers by Anita Slomski Mass General Hospital
“I believe there is an association between LDL cholesterol and heart disease, but it’s very weak and it’s certainly not causal,” says Redberg, professor of medicine at University of California, San Francisco. She declines to treat patients with statins to prevent a first heart attack or stroke regardless of LDL-C levels. Although current clinical guidelines call for giving statins to anyone who has LDL-C of at least 190 milligrams per deciliter, Redberg advised her mother, who had high total cholesterol, not to take any statins. Redberg attributes the longevity of her mother, who lived to age 94, to a good diet and exercise. “Mine is a minority opinion among physicians, but it should be mainstream,” says Redberg, who launched a “Less is More” series of articles in JAMA Internal Medicine that focuses on what she considers the overmedicalization of Americans.
Retired cardiologist Robert DuBroff, who taught at the University of New Mexico, says some patients with high LDL-C may benefit from statins. But he thinks it’s time for physicians to acknowledge that randomized controlled trials have at times produced inconsistent and contradictory evidence about the benefits of cholesterol reduction. His analysis of 35 cholesterol-lowering drug trials, published in BMJ Evidence-Based Medicine in 2020, found that there was no mortality benefit in roughly three-fourths of the trials, and nearly half reported no
A 2016 meta-analysis examining 25 statin trials showed that the more you reduce cholesterol, the greater the cardiovascular benefit. And Labos’s own study that analyzed data from recent randomized trials of statins found conclusively that statins’ cardiovascular benefit is directly related to their LDL-C-lowering properties rather than to any other effects.
Redberg has long disputed the majority view of cholesterol and statins. “I believe there is an association between LDL cholesterol and heart disease, but it’s very weak and it’s certainly not causal,” says Redberg, professor of medicine at University of California, San Francisco. She declines to treat patients with statins to prevent a first heart attack or stroke regardless of LDL-C levels. Although current clinical guidelines call for giving statins to anyone who has LDL-C of at least 190 milligrams per deciliter, Redberg advised her mother, who had high total cholesterol, not to take any statins. Redberg attributes the longevity of her mother, who lived to age 94, to a good diet and exercise. “Mine is a minority opinion among physicians, but it should be mainstream,” says Redberg, who launched a “Less is More” series of articles in JAMA Internal Medicine that focuses on what she considers the overmedicalization of Americans.
Redberg says she believes there are minimal benefits in taking a statin to prevent a heart attack or stroke for someone who hasn’t already had one. “If 100 people take statins for primary prevention, only two will avoid a heart attack, which means that 98 won’t get any benefit from the statins, but up to 20% will have adverse effects and none will live longer,” she says.
But Redberg’s advice about statins is different for those who have already had a heart attack or stroke. For so-called secondary prevention, taking a statin may be worthwhile because the cardiovascular risk is so much higher, she says. “Everyone who has had a heart attack gets a statin, regardless of their cholesterol level, because you are much more likely to have a second heart attack after your first one,” Redberg says. “If your risk of having a second heart attack is 20%, a statin may cut that risk by 2%.” In contrast, a healthy person with high cholesterol may have a 1% chance of having a heart attack, and taking a statin reduces that risk by a mere 0.1%, she says. This is accurate, according to Labos. “The higher your risk, the more you benefit from treatment, which is pretty standard in all fields of medicine,” he says.
Data Kept Secret
For instance, the Cholesterol Treatment Trialists’ (CTT) Collaboration, a division at the University of Oxford in the United Kingdom that has received significant financial support from the pharmaceutical industry, keeps patient-level trial data secret. “Virtually everything we and the experts who write clinical guidelines know about statins comes from the CTT Collaboration,” says John Abramson, a lecturer on health care policy at Harvard Medical School and author of Overdosed America. “Individual patient-level data from the trials remains sealed, which means we have no confidence that the published data are a fair and complete representation of the trials’ results.”
Editorials in JAMA and The BMJ have criticized the CTT Collaboration for refusing to make all trial data available to other researchers. The editors of The BMJ say they have made multiple requests over several years to the CTT to release the data, but only a handful of collaboration members who conduct statin trials have complied. Secrecy about statin trial results underscores the “deep flaws in our current system for evaluating medicines and guiding clinical decisions,” The BMJ editors wrote.
————————–
Statins in Elderly AAA3
A prototype of the Jarvik-7 artificial heart at the National Museum of Amercian History
Date 6 November 2023, 17:13:46
Source Own work
Author Votpuske
Lipitor and The Dracula of Modern Technology
Jarvik is best known from the media circus surrounding the 1982 implantation of his Jarvik-7 into the Seattle dentist, Barney Clark. Although the artificial heart continued to beat, Barney died of multi-organ failure 112 days after the operation, tethered to a dishwasher sized air compressor. The heart device acted as a blender which chewed up the blood cells. Recipients of the Jarvik-7 suffered horribly for months, finally succumbing to infections, strokes, convulsions, and immune system failure with decline in T cells, thus making the Jarvik-7 another cause of HIV negative AIDS.
During the ensuing media coverage, the New York Times dubbed the Jarvik Heart the “Dracula of Medical Technology” .(3,4) Jarvik-7 patients had the Kevorkian option of assisted suicide, a small “kill” switch to turn off the mechanical heart when it becomes unbearable. About 90 people received the Jarvik heart before it was banned by the FDA.
=============================
Pro-Statins
https://www.scirp.org/journal/paperin...
Schade, David S., Lynda Shey, and R. Philip Eaton. “In Defense of the LDL Hypothesis.” World Journal of Cardiovascular Diseases 9.3 (2019): 245-252.
https://openheart.bmj.com/content/9/1...
Bots, Sophie H., et al. “Statins are associated with a large reduction in all-cause mortality in women from a cardiac outpatient population.” Open Heart 9.1 (2022): e001900.
Electronic health record data from 47 801 patients (17 008 statin users and 30 793 non-users) without prior cardiovascular disease were extracted from thirteen Dutch outpatient cardiology clinics. Patients prescribed statins at baseline were propensity-score matched to those eligible for statin therapy (low-density lipoprotein >2.5 mmol/L) without a statin prescription. Statins were divided into low-intensity and high-intensity according to Dutch guidelines.
Results
Propensity score matching created a cohort of 8631 statin users and 8631 non-users. 35% of women and 28% of men received a low-intensity statin. The beneficial effect of statins on both all-cause and cardiovascular mortality was stronger in women (HR 0.66, 95% CI 0.58 to 0.74 and HR 0.55, 95% CI 0.39 to 0.71, respectively) than in men (HR 0.89, 95% CI 0.81 to 0.95 and HR 0.93, 95% CI 0.77 to 1.08, respectively). High-intensity statins conferred modest protection against all-cause mortality (HR 0.94, 95% CI 0.88 to 1.00) and cardiovascular mortality (HR 0.86, 95% CI 0.74 to 0.98) in both sexes
========================
ANti Statins
Rabaeus, Mikael, and Michel de Lorgeril. “A Systematic Review of Clinical Trials Testing CETP and PCSK9 Inhibitors: The Cholesterol-Heart Theory—Time for a Requiem?.” Journal of Controversies in Biomedical Research 5.1 (2019): 4-11.
https://newswithviews.com/Ellison/sha...
THE HIDDEN ORIGIN OF STATIN DRUGS. Shane Ellison M. Sc.
April 10, 2005 NewsWithViews.com
Statins are poisons derived from fungus… statins are nothing more than an isolated poison derived from the fungus known as red yeast rice (Monascus purpurus).[1]
As a toxic agent, the consumption of lovastatin via red yeast rice by its predators leads to sickness and in some cases, death… Nowhere in the history of man has an acknowledged poison been touted as a daily vitamin for every man, woman and child.
https://pubmed.ncbi.nlm.nih.gov/15673...
Schupf, Nicole, et al. “Relationship between plasma lipids and all‐cause mortality in nondemented elderly.” Journal of the American Geriatrics Society 53.2 (2005): 219-226.
Nondemented elderly with levels of total cholesterol, non-HDL-C, and LDL-C in the lowest quartile were approximately twice as likely to die as those in the highest quartile (rate ratio (RR)=1.8, 95% confidence interval (CI)=1.3-2.4).
Low cholesterol level is a robust predictor of mortality in the nondemented elderly and may be a surrogate of frailty or subclinical disease.
-========================
https://www.ncbi.nlm.nih.gov/pmc/arti...
Golomb, Beatrice A., et al. “Statin Effects on Aggression: Results from the UCSD Statin Study, a Randomized Control Trial.” PLoS ONE 10.7 (2015).
Statin effects on aggression differed by sex and age: Statins generally decreased aggression in men; and generally increased aggression in women. Both findings were selectively prominent in participants with low baseline aggression – bearing lower change-variance, rendering an effect more readily evident.
Newson, Rachel S., et al. “Association between serum cholesterol and noncardiovascular mortality in older age.” Journal of the American Geriatrics Society 59.10 (2011): 1779-1785.
Akerblom, Jennifer L., et al. “Relation of plasma lipids to all-cause mortality in Caucasian, African-American and Hispanic elders.” Age and ageing 37.2 (2008): 207-213.
https://www.ncbi.nlm.nih.gov/pmc/arti...
Cabrera, Marcos Aparecido Sarria, Selma Maffei de Andrade, and Renata Maciulis Dip. “Lipids and all‐cause mortality among older adults: a 12‐year follow‐up study.” The Scientific World Journal 2012.1 (2012): 930139.
This is a 12-year follow-up cohort study with 800 people (60–85 years old)
The mortality showed a positive association with low TC and a negative association with high TC and high LDL-c. After the exclusion of underweight and premature mortality, there was a positive association only with TC <170 mg/dl (HR = 1.36, CI95%: 1.02–1.82). The data did not show a higher risk with high levels of TC, LDL-c, and TG. However, they showed higher mortality among older adults with low TC.
Discussion
The results indicate higher mortality among older people with lower levels of total cholesterol. Furthermore, they show no association between all-cause mortality and hypercholesterolemia, high LDL-c, low HDL-c, hypertriglyceridemia, and high non-HDL-c in this group of older adults.
Our results did not show a positive association between hyperlipidemias and all-cause mortality.
Nguyen, Xuan‐Mai T., et al. “Serum Cholesterol and Impact of Age on Coronary Heart Disease Death in More Than 4 Million Veterans.” Journal of the American Heart Association 12.21 (2023): e030496.
Lv, Yue-Bin, et al. “Low-density lipoprotein cholesterol was inversely associated with 3-year all-cause mortality among Chinese oldest old: data from the Chinese Longitudinal Healthy Longevity Survey.” Atherosclerosis 239.1 (2015): 137-142.
The goal of this study was to assess the relationship between LDL-C and all-cause mortality among Chinese oldest old (aged 80 and older) in a prospective cohort study.
Among the Chinese oldest old, higher LDL-C level was associated with lower risk of all-cause mortality. Our findings suggested the necessity of re-evaluating the optimal level of LDL-C among the oldest old.
https://www.ncbi.nlm.nih.gov/pmc/arti...
Wang, Mu-Cyun, et al. “Plasma lipid concentrations and survival in geriatric population: A retrospective cohort study.” Medicine 98.49 (2019).
We concluded that TC, mostly attributed to LDL cholesterol, was inversely related to all-cause mortality. HDL remained to be protective against both cardiovascular and stroke mortality in older females. The target levels of plasma lipids in people older than 65 years should be different from that in younger adults.
It is well known that higher total cholesterol (TC) in mid-life is associated with higher overall and cardiovascular mortality.[1,2]
However, this positive relation attenuates with increasing age.[3,4]
Studies have shown hypercholesterolemia is no longer a risk factor for cardiovascular mortality in people older than 70 years.[5,6]
On the other hand, low TC may increase all-cause mortality in the oldest old.[7–12]
https://jamanetwork.com/journals/jama...
Krumholz, Harlan M., et al. “Lack of association between cholesterol and coronary heart disease mortality and morbidity and all-cause mortality in persons older than 70 years.” Jama 272.17 (1994): 1335-1340.
Turusheva, Anna, et al. “Low cholesterol levels are associated with a high mortality risk in older adults without statins therapy: An externally validated cohort study.” Archives of gerontology and geriatrics 90 (2020): 104180.
!!!!!!!!!!!! BEST !!!!!!!!!!!!!!
https://www.researchgate.net/profile/... ved/links/5f3d25a0458515b7292c9c75/Statins-and-death-due-to-any-cause-all-doubts-removed.pdf
Barukčić, Ilija. “Statins and death due to any cause–all doubts removed.” Int J Curr Sci Res 5.12 (2019): 1884-1911.
Results: The data of the studies reanalyzed provide convincing evidence that statins unfortunately do not exclude death due to any cause. Overwhelming evidence suggests that the risk of harmful effects of statin therapy far outweigh any real or perceived benefit.
Conclusions: An immediate statin therapy discontinuation should be considered.
==========================
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
=========================
https://www.ncbi.nlm.nih.gov/pmc/arti...
Fracassi, Anna, et al. “Statins and the brain: more than lipid lowering agents?.” Current neuropharmacology 17.1 (2019): 59-83.
Zipp, Frauke, et al. “Impact of HMG-CoA reductase inhibition on brain pathology.” Trends in pharmacological sciences 28.7 (2007): 342-349.
Smolders, Inge, et al. “Simvastatin interferes with process outgrowth and branching of oligodendrocytes.” Journal of neuroscience research 88.15 (2010): 3361-3375.
=========================
Ucar, Memduh, Tom Mjörndal, and Rune Dahlqvist. “HMG-CoA reductase inhibitors and myotoxicity.” Drug safety 22 (2000): 441-457.
Omar, Mohamed A., James P. Wilson, and Tamara S. Cox. “Rhabdomyolysis and HMG-CoA reductase inhibitors.” Annals of Pharmacotherapy 35.9 (2001): 1096-1107.
Kajinami, Kouji, Noboru Takekoshi, and Yasushi Saito. “Pitavastatin: efficacy and safety profiles of a novel synthetic HMG‐CoA reductase inhibitor.” Cardiovascular drug reviews 21.3 (2003): 199-215.
Ghirlanda, Giovanni, et al. “Evidence of plasma CoQ10‐lowering effect by HMG‐CoA reductase inhibitors: a double‐blind, placebo‐controlled study.” The Journal of Clinical Pharmacology 33.3 (1993): 226-229.
Golomb, Beatrice A., et al. “Statin effects on aggression: results from the UCSD statin study, a randomized control trial.” PloS one 10.7 (2015): e0124451.
Leppien, Emily, et al. “Effects of statins and cholesterol on patient aggression: is there a connection?.” Innovations in clinical neuroscience 15.3-4 (2018): 24.
Pop, Gabriela, et al. “Post-Marketing surveillance of statins—A descriptive analysis of psychiatric adverse reactions in EudraVigilance.” Pharmaceuticals 15.12 (2022): 1536.
Diamond, David M., Benjamin T. Bikman, and Paul Mason. “Statin therapy is not warranted for a person with high LDL-cholesterol on a low-carbohydrate diet.” Current Opinion in Endocrinology, Diabetes and Obesity 29.5 (2022): 497-511.
Cham, Stephanie, Hayley J. Koslik, and Beatrice A. Golomb. “Mood, personality, and behavior changes during treatment with statins: a case series.” Drug safety-case reports 3 (2016): 1-13.
https://bmjopen.bmj.com/content/14/3/...
Kip, Kevin E., et al. “Is LDL cholesterol associated with long-term mortality among primary prevention adults? A retrospective cohort study from a large healthcare system.” BMJ open 14.3 (2024): e077949.
—————————————-
http://drdavidbrownstein.blogspot.com/
From Dr Browntsein
What prompted this post? An article in Clinical Nutrition revealed that compared to elderly patients with cholesterol levels of 200mg/dl, those with cholesterol levels of 183mg/dl had a significantly higher death rate. (1) The authors found that for every 1mg/dl increase in serum cholesterol, the death rate was reduced by 0.4%. You read that correctly—elevated cholesterol levels protect the elderly from death.
The Honolulu Heart Program found that men aged 71-93 years in the lowest total cholesterol group had a 64% increase risk in death as compared to men with the highest cholesterol levels.(2)
The Honolulu study was reported in 2001. It is too bad the media does not trumpet these results.
elderly patients with cholesterol levels of 200mg/dl, those with cholesterol levels of 183mg/dl had a significantly higher death rate
(1) Clinical Nutrition. Nov. 7, 2012. Doi.org/10.1016/j.cinu.2012.11.012
(2) Schatz, I. J. “Cholesterol and all-cause mortality in elderly people from the Honolulu Heart Program.” LANCET-LONDON- (2001): 351-355.
Published on July 18th, 2024 by Jeffrey Dach MD
The post The Failure of Cholesterol Lowering Drugs appeared first on Jeffrey Dach MD.


July 2, 2024
Copper T IUD No Longer Recommended
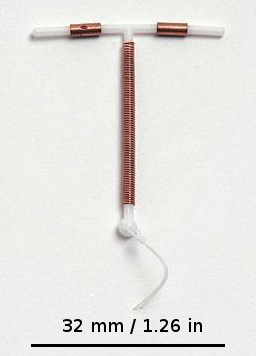 The Paraguard Copper T – IUD is No Longer Recommended by Jeffrey Dach MD
The Paraguard Copper T – IUD is No Longer Recommended by Jeffrey Dach MD
The Copper T IUD is currently in litigation for breakage of the arm during removal with retention of fragments in the uterine cavity. Other issues include heavy bleeding, disruption of vaginal microbiome with recurrent vaginal infection, copper toxicity or sensitivity, etc. Instead of the Copper T IUD, use a barrier method such as the diaphram or cervical cap (2-3)
Credit and thanks for this information goes to Lindsey Berkson and David Brownstein who discussed the adverse effects of the copper T IUD in their “Everything Hormones” course.(1)
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
Article with Related Interest
Adverse Effects of Birth Control Pills
All Articles related to Hormone Therapy
 Images and Credits
Images and Credits
Header Image above: A common copper IUD (Paragard) with scale markings. 24 July 2012, Source File:Multiload-Gynefix-Paragard.jpg, Author User:LeiaWonder, CC 4.0
Left Image, Second Image: A cervical cap and Patentex (spermicidal) gel in the Deutsches Museum, Munich. Sony ILCE-5000 camera. 12 August 2017, Author Tiia Monto. Courtesy of wikimedia commons.
Third image below: Ortho Tri-Cyclen oral contraceptives with Ortho Dialpak dispensers Date 12 April 2006 Source Transferred from en.wikipedia to Commons.; transfer was stated to be made by Tanvir. Author BetteDavisEyes at English Wikipedia.
 References:
References:
1) “Everything Hormones” by David Brownstein and Lindsey Berkson
Copper T IUD No Longer Recommended. USE cervical CAP and Diaphragm. (Barrier Methods) Very effective if people use them.
(Barrier Methods)
2) Kaunitz, Andrew M. “Patient education: Birth control, which method is right for me?(Beyond the Basics).” (2024).
3) https://www.acog.org/womens-health/fa...
Barrier Methods of Birth Control: Spermicide, Condom, Sponge, Diaphragm, and Cervical Cap
Frequently Asked Questions
========================================
EP 69: Why the Copper IUD is Not a Safe Form of Birth Control
Samantha Gilbert FNC, CHNP, CNC Nutritional Therapy Counselor and Hope Communicator
From what I’ve seen over the last 14 years, the opposite is true, yet when a woman notices chronic symptoms such as yeast infections, anxiety and panic attacks, and even psychosis after insertion of this device, she is often gaslit and told to see a psychiatrist.
The FDA first approved the copper IUD under the name Paragard in 1984. In the 30 years since Paragard was approved, there have been more than 40,000 reports to the FDA according to publicly available data in the FDA Adverse Events Reporting System database (otherwise known as FAERS),
https://www.drugwatch.com/paragard/la...
Litigation is ongoing against Paragard for injuries caused to women by the company’s intrauterine device. As of July 2024, there were 2,736 pending lawsuits and a total of 2,822 cases filed against the company in the federal court in Georgia under MDL number 2974. The first of the bellwether trial cases will be heard in 2024.
arm breakage upon removal
The Paragard IUD lawsuits claim a design flaw led to the IUD device breaking during removal. This meant that part of the device could remain lodged in the uterus or other internal organs, causing injuries.
Implanting a copper IUD into a female who is already (and usually unknowingly) overloaded with copper is a recipe for disaster. To make matters worse, few doctors are aware of copper overload, thus, they may unintentionally prescribe hormones and/or devices that could negatively impact health and well-being.
An overabundance of copper can also have a devastating effect on mental health because copper lowers dopamine (a neurotransmitter that controls the brain’s pleasure and reward centers) and increases norepinephrine (a neurotransmitter that also functions as a stress hormone) in the brain.
This explains why common, yet undisclosed side effects of copper IUDs include severe anxiety and panic attacks, depression, hair loss, anemia, increased anger and rage, brain fog, spaciness, paranoia, fatigue, and yeast and bacterial infections.
all of my female clients have complained about symptoms of insomnia, racing thoughts, heart palpitations, and dizziness after a copper IUD is inserted for birth control.
Postpartum depression (PPD) and psychosis are directly connected to elevated levels of copper, especially with multiple births because copper levels increase with each pregnancy
copper overload is quite common in women because estrogen increases copper retention in the body. It is often inherited and brought on during hormonal events such as puberty and pregnancy. If you and the women in your family share similar traits and conditions such as ADHD, painful periods, or depression, I encourage getting your copper levels checked because copper overload may run in your family as it does in mine
Zinc deficiency in parents before conception can cause miscarriage, fetal growth restrictions, learning disabilities, and mental health challenges.
In fact, thanks to great work of Dr. William Walsh, zinc deficiency is the most frequently observed chemical imbalance in mental health and cognitive functioning with more than 90% of individuals diagnosed with depression, anxiety, behavioral disorders, ADHD, autism, and schizophrenia to exhibit depleted plasma zinc levels. Additionally, most mental health disorders involve oxidative stress that depletes zinc stores in the body.
Zinc is necessary to produce important neurotransmitters and hormones such as serotonin, GABA, and dopamine.
When copper becomes elevated it turns into an pro-inflammatory agent.
https://www.peacefulmountainmedicine....
Dr. Ryan Monahan, DAOM, LAc, IFMCP
Functional Medicine | Eastern Medicine
Copper IUDs: The Problems With Paragard
© 2024 Peaceful Mountain Medicine and Acupuncture Inc.
The safest and most effective approach to natural, non-hormonal birth control is a combination of the Natural Cycles App in conjunction with intravaginal neem oil injected five minutes prior to sexual intercourse.
In clinical study, Natural Cycles App has been found to be 93% effective against pregnancy, while neem oil was found to be 96.2% effective against pregnancy in a 2018 study involving 238 women.
??? Diaphragm
https://pubmed.ncbi.nlm.nih.gov/17317...
Crayton, John W., and William J. Walsh. “Elevated serum copper levels in women with a history of post-partum depression PPD.” Journal of Trace Elements in Medicine and Biology 21.1 (2007): 17-21.
The mean serum Cu level of 78 women with a history of PPD was 131+/-39microg/dL compared with 111+/-25microg/dL in 148 women without such a history, and 106+/-20microg/dL in non-depressed controls (p<0.001).
https://www.ncbi.nlm.nih.gov/pmc/arti...
Brown, Bryan P., et al. “Copper intrauterine device increases vaginal concentrations of inflammatory anaerobes and depletes lactobacilli compared to hormonal options in a randomized trial.” Nature Communications 14.1 (2023): 499.
https://pubmed.ncbi.nlm.nih.gov/8899120/
D’Ambrosio, F. Purello, et al. “Systemic contact dermatitis to copper-containing IUD.” Allergy 51.9 (1996).
PIP: Although copper sulfate can cause systemic contact dermatitis, few such cases have been recorded among copper-releasing IUD users. Reported in this paper is a case of endometritis and urticaria-angioedema syndrome in a 32-year-old user of a copper IUD. Widespread urticaria, as well as angioedema of the eyelids and the labia majora and minora, persisted for about 6 months and were not responsive to corticosteroids and H1-antagonists. Copper sulfate positivity was demonstrated in 72-hour patch test, 48-hour application of the copper spiral to forearm, and in vitro lymphocyte-stimulating test. Histologic examination of the endometrial biopsy revealed vulvovaginitis with hyperplasia of the cervical canal and T-cell and eosinophilic granulocyte infiltration. Removal of the IUD caused complete symptom remission. In experimental animals with a radioactively labeled copper IUD, small amounts of copper sulfate are absorbed through the mucus membrane and carried to the cutis through the blood or lymph. In the cutis, the allergen is intercepted from antigen-presenting cells and recognized by T cells that migrate to the lymph nodes with blastic transformation, proliferation of cytotoxic lymphocytes, and cytokine production.
Gara, Soumaya, et al. “Systemic allergic dermatitis caused by a copper‐containing intra‐uterine device.” Contact Dermatitis (01051873) 84.2 (2021).
Copper/Zinc Ratio in Psoriais
https://www.ncbi.nlm.nih.gov/pmc/arti...
Aggarwal, Jyoti, et al. “Copper and zinc status in psoriasis: correlation with severity.” Indian Journal of Clinical Biochemistry 36.1 (2021): 120-123.
The serum trace elements analysis in the subjects revealed that serum Cu levels and Cu/Zn ratio was significantly higher in the psoriatic patients as compared to controls. Interestingly, severity of the psoriasis was well correlated with the serum Cu levels. Taking together, all these findings suggest that Cu may be a major culprit in the pathogenesis as well as in the severity of the disease.
No copper Toxicity
https://www.ajol.info/index.php/ejhm/...
Atef, Alaa Mohamed, et al. “The Association between Elevated Serum Copper (Cu) Levels and Its Complications in Cu T380a IntrauterineDevice (IUD) Users; a Cross-Sectional Study.” The Egyptian Journal of Hospital Medicine (January 2024) 94: 1263-1267.
A total of 159 women using copper T380A IUD as a method of contraception
Conclusion: There was no rise in blood copper levels among IUD users, regardless of duration of usage. Copper T380A IUD is recommended to be used safely without danger of Cu toxicity.
Crandell, Lena, and Natalie Mohler. “A literature review of the effects of copper intrauterine devices on blood copper levels in humans.” Nursing for Women’s Health 25.1 (2021): 71-81.
——————————-
Copper T IUD causes Aseptic inflammation
Che, Jia-Hui, and Xiao-Ying Yao. “Effects of copper-containing intrauterine devices on the endometrium.” Reproductive and Developmental Medicine 5.01 (2021): 38-43.
https://mednexus.org/doi/full/10.4103...
Studies on the morphology of endometrium indicate that the use of Cu-IUDs can affect the number and binding capacity of estrogen and progesterone receptors in the endometrium and reduce the response of the endometrium to estrogen and progesterone. The use of Cu-IUDs can also affect the proliferation of endometrial cells, suggesting that the aseptic inflammation caused by Cu-IUDs may differ from chronic infectious or noninfectious inflammation; this highlights that the use of Cu-IUDs provides protection against endometrial proliferative diseases. The use of Cu-IUDs increases local endometrial angiogenesis, bleeding tendency, and fibrinolytic activity, which can result in prolonged menstruation or abnormal uterine bleeding.
https://pubmed.ncbi.nlm.nih.gov/35873...
Wemrell, Maria, and Lena Gunnarsson. “Attitudes Toward the Copper IUD in Sweden: A Survey Study.” Frontiers in global women’s health 3 (2022): 920298.
Results: While many reported positive attitudes toward and experiences of the IUD, 34.7% of all respondents reported negative attitudes and 45.4% of users reported negative experiences. Negative attitudes were strongly correlated with negative experiences.
https://pubmed.ncbi.nlm.nih.gov/31990...
Omran, Eman A., et al. “Copper IUD increases virulence of non-albicans Candida species isolated from women with vulvovaginal candidiasis.” The European Journal of Contraception & Reproductive Health Care 25.2 (2020): 120-125.
Conclusion: IUD use enhanced the virulence (proteinase production and antifungal resistance) of NAC but not C. albicans, indicating a variation in virulence between Candida species in response to IUD use. C. albicans responded better to fluconazole, whereas NAC isolates were more sensitive to nystatin.
https://www.ncbi.nlm.nih.gov/pmc/arti...
Sarver, Jordan, Melissa Cregan, and Daniel Cain. “Fractured copper intrauterine device (IUD) retained in the uterine wall leading to hysterectomy: a case report.” Case Reports in Women’s Health 29 (2021): e00287.
During careful removal of the IUD, a piece was broken off and remained in the uterine cavity. Upon visual inspection of the removed IUD, the right wing was missing and presumed to be still in the patient.
=======================================================
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright © 2024 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on July 2nd, 2024 by Jeffrey Dach MD
The post Copper T IUD No Longer Recommended appeared first on Jeffrey Dach MD.
June 28, 2024
The Dangers of Sleeping Pills

The Dangers of Sleeping Pills by Jeffrey Dach MD
Mary is a 52 year old house wife from Wyoming who takes an Ambien sleeping pill every night for the last three years. Because of worrisome menopausal symptoms of vaginal dryness, hot flashes and night sweats, Mary was starting on hormone replacement with bioidentical estrogen and progesterone. A problem was apparent early on. Mary required three times the dosage of estrogen cream compared to all the other patients. Perhaps the Ambien sleeping pills are interfering with or blocking the progesterone and estrogen receptors in the brain?
Header Image: A lion and a lioness sleeping in the Serengeti. 31 July 2002 by Vincenzo Gianferrari Pini. Courtesy of Wikimedia Commons.
Sleeping Pills Mechanism of Action
 The most commonly prescribed sleeping pills in the U.S. are the “Z drugs” (zolpidem, zopiclone, and zalephon). How do they work? The the Z drugs have a mechanism very similar to the benzodiazepine class of drugs, they inhibit the Type A- GABA neurons in the brain. The GABA neurons are inhibitory while the Glutamate neurons are excitatory. (9)
The most commonly prescribed sleeping pills in the U.S. are the “Z drugs” (zolpidem, zopiclone, and zalephon). How do they work? The the Z drugs have a mechanism very similar to the benzodiazepine class of drugs, they inhibit the Type A- GABA neurons in the brain. The GABA neurons are inhibitory while the Glutamate neurons are excitatory. (9)
Above Left Image: Unable to sleep, person with with eye bags. February 2022, Digital art work by Itzamna3211, Creative Commons CC0 1.0 . Courtesy of Wikimedia Commons.
Z-Drugs Inhibit Estrogen and Progesterone Receptors in the GABA Neurons
The problem is these GABA neurons have estrogen and progesterone receptors attached to them, so when we inhibit these neurons with a sleeping pill “Z-drug”, this also inhibits the estrogen and progesterone receptors, thus requiring higher doses of hormones to be effective for relief of menopausal symptoms.
Z- Drugs Increase Mortality and Cancer
Two large studies show the Z drug sleeping pills are associated with increased mortality and a host of other medical problems. In addition, sleeping pills become ineffective through tolerance for chronic users, and actually reduce functionality the following day.
Progesterone Induces Sleep Via Same GABA receptors
How does progesterone help with sleep? What is the mechanism of action? This was aptly described in 2021 by Dr. B. J. Nolan who states progesterone metabolites inhibit the GABA neurons, in a mechanism very similar to the Z-drug sleeping pills. Dr. B. J. Nolan who writes:
Preclinical data has shown progesterone metabolites improve sleep parameters through positive allosteric modulation of the γ-aminobutyric acid type A receptor [GABA Type A Receptor]….(5)
CBT and Bright Light Therapy
Cognitive Behavior therapy and Bright Light Therapy are considered first line treatment for sleep. For post menopausal women, hormone replacement with estrogen and progesterone is usually effective and should be first line therapy.
Conclusion: Sleeping pills interfere with estrogen and progesterone receptors in GABA neurons in the brain, requiring much larger hormone doses to have efficacy. Z-drug sleeping pills are associated with increased mortality. It is best for the post-menopausal woman to taper off sleeping pills and use progesterone for sleep, a much safer choice not associated with the increased mortality of sleeping pills.
Articles with Related Interest
All Bioidentical Hormone Articles
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
==============================
References
HRT Menopause Sleep
!!!!!!!!!!!!!!!!!!!!! BEST !!!!!!!!!!!!!!!!!!
1) Almey, Anne, Teresa A. Milner, and Wayne G. Brake. “Estrogen receptor α and G-protein coupled estrogen receptor 1 are localized to GABAergic neurons in the dorsal striatum.” Neuroscience letters 622 (2016): 118-123.
This experiment demonstrated that ERα and GPER1 are localized to GABA neurons in the STR [striatum]. ERs were observed in GABAergic terminals and dendrites, where they are positioned to modulate transmission at GABA synapses. These ERs on GABAergic profiles are a possible mechanism for the rapid E2-induced decreases in GABA in the STR, and suggest that estrogens may indirectly affect dopamine transmission in this region by decreasing GABA availability…
Estrogen receptors have been shown to be membrane associated in the dorsal striatum…. Here we confirm that and show that they are localized to GABA neurons.
ERα and GABA most frequently colocalize in dendrites and terminals
There are moderate levels of colocalization between ERα and GABA in the STR. Colocalization of ERα- and GABA- IRs was most commonly observed in dendritic shafts (Fig. 2 A, B), with 35.3% of ERα immunoreactive dendrites containing GABA-IR (see Table 1). Colocalization of GABA- and ERα- IRs was also frequently (27.1%) observed in axon terminals (Fig 2B).
Thus, to determine whether ERα or GPER1 are localized to GABAergic neurons, we double labeled the striatum with antibodies for ERα or GPER1 and GABA and examined them using electron microscopy. Ultrastructural analysis revealed that ERα and GPER1 are localized exclusively to extranuclear sites in the striatum, and ~35% of the dendrites and axon terminals labeled for these receptors contain GABA immunoreactivity. Binding at membrane-associated ERα and GPER1 could account for rapid estrogen-induced decreases in GABA transmission in the striatum, which, in turn, could affect dopamine transmission in this region.
2) Thind, Khushdev K., and Paul C. Goldsmith. “Expression of estrogen and progesterone receptors in glutamate and GABA neurons of the pubertal female monkey hypothalamus.” Neuroendocrinology 65.5 (1997): 314-324.
In summary, certain subpopulations of Glu and GABA neurons in principal hypothalamic regions of the female monkey express ER and PR at midpuberty. Taken together with previous findings, these results suggest that Glu and GABA neurons which become sensitive to steroid hormones may help regulate GnRH neurohormone release and promote the onset of puberty.
================================================
3) Kapur, Jaideep, and Suchitra Joshi. “Progesterone modulates neuronal excitability bidirectionally.” Neuroscience letters 744 (2021): 135619.
Progesterone acts on neurons directly by activating its receptor and through metabolic conversion to neurosteroids. There is emerging evidence that progesterone exerts excitatory effects by activating its cognate receptors (progesterone receptors, PRs) through enhanced expression of α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid receptors (AMPARs). Progesterone metabolite 5α,3α-tetrahydro-progesterone (allopregnanolone, THP) mediates its anxiolytic and sedative actions through the potentiation of synaptic and extrasynaptic γ-aminobutyric acid type-A receptors (GABAARs).
Progesterone synthesized in the ovaries and adrenocortical glands can easily cross the blood-brain barrier and can also be synthesized locally in the brain from cholesterol.
The most commonly studied molecule is its metabolite allopregnanolone (THP). These effects are rapid and potentiate the inhibitory neurotransmission mediated through the GABAARs [GABA Type A Receptors] .
Estrogen stimulates PR expression;
4) Guennoun, Rachida. “Progesterone in the brain: hormone, neurosteroid and neuroprotectant.” International journal of molecular sciences 21.15 (2020): 5271.
Progesterone has a broad spectrum of actions in the brain. Among these, the neuroprotective effects are well documented. Progesterone neural effects are mediated by multiple signaling pathways involving binding to specific receptors (intracellular progesterone receptors (PR); membrane-associated progesterone receptor membrane component 1 (PGRMC1); and membrane progesterone receptors (mPRs)) and local bioconversion to 3α,5α-tetrahydroprogesterone (3α,5α-THPROG), which modulates GABAA receptors.
5) Nolan, B. J., B. Liang, and A. S. Cheung. “Efficacy of Micronized Progesterone for Sleep: A Systematic Review and Meta-analysis of Randomized Controlled Trial Data.” The Journal of Clinical Endocrinology and Metabolism 106.4 (2021): 942-951.
Conclusions: Micronized progesterone improves various sleep outcomes in randomized controlled trials, predominantly in studies enrolling postmenopausal women.
Preclinical data has shown progesterone metabolites improve sleep parameters through positive allosteric modulation of the γ-aminobutyric acid type A receptor….Our search strategy retrieved 9 randomized controlled trials comprising 388 participants.
mice study
6) Lancel, Marike, et al. “Progesterone induces changes in sleep comparable to those of agonistic GABA-A receptor modulators.” American Journal of Physiology-Endocrinology and Metabolism 271.4 (1996): E763-E772.
The effects of progesterone on sleep closely resemble those of agonistic modulators of GABAA receptors such as benzodiazepines and correlate well with the increases in the levels of its GABAA agonistic metabolites. These observations suggest that the hypnotic effects of progesterone are mediated by the facilitating action of its neuroactive metabolites on GABAA receptor functioning.
pdf
7) Jeon, Gyun-Ho. “Insomnia in Postmenopausal Women: How to Approach and Treat It?.” Journal of Clinical Medicine 13.2 (2024): 428.
menopausal hormone therapy (MHT) should be considered as the treatment of choice among pharmacological treatments, following cognitive behavioral therapy, which is suggested as the first-line treatment in the general population insomnia treatment guidelines. Additionally, melatonin and 5HT-based drugs, which have fewer side effects, along with MHT should be preferentially recommended in menopausal women…menopausal women with insomnia also need an individualized approach and
treatment (MHT, prolonged-release melatonin, 5HT-based drugs, etc.) under the premise that CBT should be used as the first-line treatment, following the treatment guidelines of
insomnia for the general population.
Previous studies have reported beneficial effects of female sexual hormones on sleep…Estrogen blocks wake-promoting neurotransmitters, such as acetylcholine, histamine, norepinephrine, serotonin, and dopamine [19], and is known to have a thermoregulatory effect of regulating the lowest body temperature during the night, which provides good conditions
for falling asleep [20]. Overall, estrogen seems to increase the rapid eye movement sleep and total sleep time and decrease sleep latency and awakenings after sleep [21].
Estrogen may also exert an antidepressant effect by regulating 5HT [22]. Progesterone stimulates benzodiazepine receptors, causing the release of gamma-aminobutyric acid (GABA),
a sedating neurotransmitter, and thus induces sleep favoring non-rapid eye movement sleep [23,24]. Progesterone is also known to exert an anxiolytic and respiratory stimulant effect [24,25], which may also help promote good sleep.
Menopausal Hormone Therapy
Based on the identified roles of reproductive hormones in sleep and the theory that vasomotor symptoms (VMS), such as HFs, in menopause cause insomnia, as discussed above, MHT can be an important treatment for insomnia in menopausal women with
hot flashes. Indeed, a meta-analysis including 15,468 women from 42 trials published in 2017 showed that MHT improved sleep quality in menopausal women with VMS, along with improvement in concomitant VMS. There was no significant difference when women without VMS were analyzed separately or combined in this study [53]. However, several previous studies exploring the effects of estrogen and progesterone on sleep efficiency have
shown mixed results. While some studies suggested that hormone therapy, such as low dose estrogen with micronized progesterone or drospirenone, 17β-estradiol-progesterone, and low-dose oral estradiol and venlafaxine, reduced insomnia symptoms compared with a placebo [54–58], some contrary results were also reported, which failed to identify any superiority of MHT over the placebo [59,60]. Even studies favoring the effectiveness of MHT mainly showed improvements in subjective sleep quality and tended to show inconsistent results in objective PSG variables [61–63]. This lack of consistency is due to the heterogeneity of the trials regarding differences in study populations, age, definitions of
menopausal stages, types of menopause, preparations of hormones, and unstandardized sleep scales; therefore, there is a limitation of overall certainty in the evidence of the MHT
effects on sleep disturbances [11,53]. Nevertheless, based on the fact that MHT is effective for HFs in peri- and post-menopausal women and helps improve quality of life, there is an emerging view that MHT can be considered as the first-line treatment when insomnia is suspected to be part of VMS, and it is better to first evaluate the response of MHT and then
consider other treatments for insomnia in menopausal women with VMS [64]. In the same context, it was reported that the degree of improvement in VMS was an important predictor
of insomnia improvement [65]. Considering the bidirectional relationship between insomnia and depression, it is difficult to determine whether insomnia in postmenopausal women is related to the high prevalence of clinical depression or depressed mood during that period or due to menopause itself. The only way to differentiate may be a trial of MHT and consideration of other therapy if insomnia or depression persists after three months of
successful MHT [64]. Before using MHT to relieve insomnia in menopausal women, it is important to monitor the side effects of MHT, such as thromboembolic events and breast cancer, and whether the benefits outweigh the risks should be evaluated. Additionally, there are recent studies showing that transdermal treatment was the safest type of hormone therapy in the assessment of risk of venous thromboembolism [66], and micronized progesterone was more effective for improving sleep, as well as reducing HFs [67], which suggests to consider transdermal estradiol and micronized progesterone for the patients at risk of thromboembolism.
8) Cheng, Yu-Shian, et al. “Pharmacologic and hormonal treatments for menopausal sleep disturbances: a network meta-analysis of 43 randomized controlled trials and 32,271 menopausal women.” Sleep Medicine Reviews 57 (2021): 101469.
Therefore, the results of the present NMA suggest that oral combined hormone replacement therapy may be useful for sleep disturbances in women suffering from vasomotor symptoms due to menopause…
=================================================================================================
9) Segal, Alan Z. “Sleeping Pills Increase Risk of Death.” Internal Medicine Alert 36.12 (2014).
Hypnotic and anxiolytic drugs have been associated with an increased risk of dementia, daytime fatigue, ataxia, falls, and traffic accidents. Medical ailments such as cancer, pneumonia, and other infections have been associated with use of these medications.
The Z-drugs (zolpidem, zopiclone, and zalephon) are the most commonly prescribed medications for insomnia in the United States.
10) Weich S, et al. Effect of anxiolytic and hypnotic drug prescriptions on mortality hazards: Retrospective cohort study. BMJ 2014;348:g1996.
In this large cohort of patients attending UK primary care, anxiolytic and hypnotic drugs were associated with significantly increased risk of mortality over a seven year period, after adjusting for a range of potential confounders. As with all observational findings, however, these results are prone to bias arising from unmeasured and residual confounding.
11) Kripke, Daniel F. “Hypnotic drug risks of mortality, infection, depression, and cancer: but lack of benefit.” F1000Research 5 (2016).
Evolving concern with hypnotic risks provides many new studies for this review, including four additional large epidemiologic analyses relating hypnotic prescriptions to excess mortality and two complementary meta-analyses demonstrating associations of hypnotic prescriptions to specific cancers. Meanwhile, the data base has grown demonstrating superior results with cognitive-behavioral therapy of insomnia and with bright light treatment.
The most important risks of hypnotics include excess mortality (especially overdose deaths, quiet deaths at night, and suicides), infections, cancer, depression, automobile crashes, falls, other accidents, and hypnotic-withdrawal insomnia. Short-term use of one-two prescriptions is associated with even greater risk per dose than long-term use. Hypnotics have usually been prescribed without approved indication, most often with specific contraindications, but even when indicated, there is little or no benefit. The recommended doses objectively increase sleep little if at all, daytime performance is often made worse (not better) and the lack of general health benefits is commonly misrepresented in advertising. Treatments such as the cognitive behavioral treatment of insomnia and bright light treatment of circadian rhythm disorders offer safer and more effective alternative approaches to insomnia.
12) Sun, Y., M. K. Tsai, and C. P. Wen. “Association of sleep duration and sleeping pill use with mortality and life expectancy: A cohort study of 484,916 adults.” Sleep Health (2023): S2352-7218.
Objectives: To compare mortality risk and life expectancy among individuals with different sleep durations and sleeping pill use.
Methods: A cohort of 484,916 community-dwelling adults in Taiwan was recruited into a health screening program from 1994 to 2011. Subjects were categorized by daily sleep duration into 4 groups: extremely short (<4 hours), short (4-6 hours), medium (6-8 hours), and long (>8 hours). Cox proportional hazards models were used to investigate the associations of mortality risk with sleep duration and sleeping pill use. Models were adjusted for sociodemographic characteristics, lifestyle, and comorbidities. Life expectancy tables were calculated among sleeping pill users and nonusers with different sleep durations.
Results: With 6- 8 hours of daily sleep, sleeping pill nonusers had the lowest mortality risk. Sleeping pill users, even with this optimal amount of sleep, had a 55% (p < .001, 95% CI, 1.38-1.73) higher mortality risk than nonusers. The life expectancy of 30-year-old male sleeping pill users with extremely short or long sleep durations was 12-13 years shorter than sleeping pill nonusers who had 6-8 hours of sleep. On average, life expectancy in individuals using sleeping pills (vs. nonusers) was shorter by 5.3 (95% CI, 4.10-6.32) years in men and 5.7 (95% CI, 5.28-7.98) years in women.
Conclusions: This study suggests that the use of sleeping pills is associated with an increased risk of mortality and shortened life expectancy, especially in extreme sleepers. Regular users should be aware of potential harms from sleeping pills.
=
==========================================
13) Kripke, Daniel F., et al. “Mortality hazard associated with prescription hypnotics.” Biological psychiatry 43.9 (1998): 687-693.
14) Kripke, Daniel F. “FDA ASKED TO SEVERELY RESTRICT USE OF MOST COMMONLY-PRESCRIBED SLEEPING PILLS.”
16) Kripke, Daniel F. “Chronic hypnotic use: deadly risks, doubtful benefit.” Sleep medicine reviews 4.1 (2000): 5-20.
In the United States, roughly 2/3 of all hypnotic prescriptions go to chronic users, who have taken hypnotics for an average of 5 years or more. Two large prospective epidemiological studies have shown that reported hypnotic use, especially use 30 times per month, is associated with an excess hazard of death. Indeed, use of hypnotics 30 times per month is associated with a similar mortality hazard to smoking 1–2 packs of cigarettes per day. Moreover, the hypnotic user’s wish to improve daytime function is usually unfulfilled. The preponderance of evidence is that hypnotics impair performance, cognition and memory, increase the risk of automobile accidents and falls and promote unfavourable changes in personality. Due to tolerance, the sleep-promoting effects of hypnotics appear to be lost with chronic use. With long-term use, there is little controlled evidence that hypnotics produce benefits of any sort. More study of long-term hypnotic effects by public agencies is needed, but available evidence weighs strongly against long-term prescribing.
17) Kripke, Daniel F., Robert D. Langer, and Lawrence E. Kline. “Hypnotics’ association with mortality or cancer: a matched cohort study.” BMJ open 2.1 (2012): e000850.
As predicted, patients prescribed any hypnotic had substantially elevated hazards of dying compared to those prescribed no hypnotics. For groups prescribed 0.4–18, 18–132 and >132 doses/year, HRs (95% CIs) were 3.60 (2.92 to 4.44), 4.43 (3.67 to 5.36) and 5.32 (4.50 to 6.30), respectively, demonstrating a dose–response association. HRs were elevated in separate analyses for several common hypnotics, including zolpidem, temazepam, eszopiclone, zaleplon, other benzodiazepines, barbiturates and sedative antihistamines. Hypnotic use in the upper third was associated with a significant elevation of incident cancer; HR=1.35 (95% CI 1.18 to 1.55). Results were robust within groups suffering each comorbidity, indicating that the death and cancer hazards associated with hypnotic drugs were not attributable to pre-existing disease.
18) Kripke, Daniel F. “Surprising view of insomnia and sleeping pills.” Sleep 36.8 (2013): 1127-1128.
19) Kripke, Daniel F. “Hypnotic drug risks of mortality, infection, depression, and cancer: but lack of benefit.” F1000Research 5 (2016).
This update adds new findings about the accelerating overdose epidemic that is suddenly reducing U.S. life expectancy. The overdose role of hypnotics and other benzodiazepine agonists in combination with opioids is further reviewed. Evidence is expanded that most hypnotic prescriptions are not indicated—indeed, the great majority have been contraindicated or result in misuse. The “weak” evidence relating minimal benefit with indicated hypnotics does not support over 90% of actual U.S. ingestion, wherein the hypnotic was not indicated or rather was contraindicated. For >90% of cases, there seems to have been no scientific evidence of benefit. On the other hand, the evidence of severe risks appears to apply to all hypnotic utilization whether or not given for an approved indication. Evolving concern with hypnotic risks provides many new studies for this review, including four additional large epidemiologic analyses relating hypnotic prescriptions to excess mortality and two complementary meta-analyses demonstrating associations of hypnotic prescriptions to specific cancers. Meanwhile, the data base has grown demonstrating superior results with cognitive-behavioral therapy of insomnia and with bright light treatment.
This is a review of hypnotic drug risks and benefits. Almost every month, new information appears about the risks of hypnotics (sleeping pills). The most important risks of hypnotics include excess mortality (especially overdose deaths, quiet deaths at night, and suicides), infections, cancer, depression, automobile crashes, falls, other accidents, and hypnotic-withdrawal insomnia. Short-term use of one-two prescriptions is associated with even greater risk per dose than long-term use. Hypnotics have usually been prescribed without approved indication, most often with specific contraindications, but even when indicated, there is little or no benefit. The recommended doses objectively increase sleep little if at all, daytime performance is often made worse (not better) and the lack of general health benefits is commonly misrepresented in advertising. Treatments such as the cognitive behavioral treatment of insomnia and bright light treatment of circadian rhythm disorders offer safer and more effective alternative approaches to insomnia.
Keywords: hypnotics and sedatives, mortality, cancer, infection, depression, insomnia, sleep
Go to:
======================================
20) The Dark Side of Sleeping Pills, Mortality and Cancer Risks, Which Drugs to Avoid & Better Alternatives By Daniel F. Kripke, M.D.
in my view, the risks of death, cancer, depression, and infection with sleeping pills, besides the behavioral impairments and accidents, are much more important than any small benefits. Besides, use of sleeping pills seems to cause insomnia, at least after withdrawal.
Even with tiny increases in sleep that they provide for a few days, hypnotics do not improve an insomnia patient’s daytime function. More often, the pills make daytime function measurably worse. Patients often seek improved function, but they usually do not receive it. Further, although we hear colleagues mention that perhaps a patient will be healthier if the patient sleeps better, our research found that patients taking sleeping pills were more likely to develop new medical disorders than matched control patients who avoided sleeping pills. I have located no reliable evidence that any sleeping pill improves general health, but there is much evidence of serious harm to physical and mental health.
The specific sleeping pills we studied were zolpidem (e.g., Ambien), temazepam (e.g., Restoril), eszopiclone (e.g., Lunesta), zaleplon (e.g., Sonata), other benzodiazepines such as triazolam (e.g., Halcion) and flurazepam (e.g., Dalmane), barbiturates, and sedative antihistamines such as diphenhydramine (e.g., Benadryl). Most of the patients in this study were taking zolpidem or temazepam.
As a young medical student in my first year of training, one of the first things I learned in our student laboratory was that the humane way to “put an animal to sleep” was to administer a fatal dose of a barbiturate such as pentobarbital. A bit later, I learned that pentobarbital was being prescribed almost automatically as a sleeping pill for patients in the hospital. Pentobarbital and related drugs are currently used to execute the death penalty on prisoners. Any medical student knows that these drugs can kill.
Doctors have a wonderfully complete understanding of how sleeping pills such as pentobarbital kill animals. These drugs bind with protein molecules called GABA receptors on the surface of nerve cells. The same protein receptor molecules bind at the same time with a neurotransmitter chemical called GABA, which gives them their name. Barbiturates and other sleeping pills accentuate the action of GABA, which is to cause the receptor molecule to allow chloride ions to enter the nerve cells. Since the chloride ions are negatively charged, they make the inside the nerve cell more negatively polarized, which in turn, makes the nerve cells less likely to fire (to generate nerve activity). When the nerve cells which stimulate the muscles of breathing are overly inhibited from firing by sleeping pills, the animal stops breathing. When breathing stops, the animal dies within a few minutes from lack of oxygen. This same mechanism explains how sleeping pills kill people who take an overdose. Mixture with other drugs, particularly opioids, alcohol and other sedatives, greatly magnifies the risks, as do various medical conditions, possibly stopping breathing with a dose not intended to be lethal.
Use of sleeping pills is very strongly associated with suicide from all causes.
Suicide, accidental overdose and cancer are probably not the most common ways in which sleeping pills kill,
All approved sleeping pills can cause “hangover,” that is, they not only reduce the action potentials of our brain cells during sleep, but they can also reduce brain cell activity during the day.[13] This can make us sleepy, less alert, confused, and weak during the day.
As explained above, sleeping pills suppress the action potentials of a wide variety of brain cells. The psychological effects are to make us sleepy, reduce alertness and vigilance, slow reaction times and judgment, and impair aspects of intelligence and memory. Literally hundreds of studies have been done concerning the psychological effects of sleeping pills, both within a few hours after ingestion and then during the day following taking a sleeping pill at bedtime.[20] To summarize an extremely complex group of studies, almost all sleeping pills produce immediate impairments of memory and performance. Further, there is extensive evidence that sleeping pills impair performance and memory on the following day.
Sleeping pills generally make function WORSE the next day.
To view sleeping pill advertising, you might imagine sleeping pills help you to work better, think better, or function better the next day. This is deceptive. With very few exceptions, controlled studies supported by the manufacturers showed that sleeping pills made test performance WORSE on the following day, or else had no definite effect on performance. Look through the FDA files for Ambien, Lunesta, Sonata, Rozerem, Belsomra, or Silenor at the FDA website.[21] See if you can find any evidence that these drugs improved next-day performance for people with insomnia. You will not find any. For the older sleeping pills, there are less definite data available in FDA files, but many studies of older hypnotics showed that sleeping pills impaired performance the next day.
Because the build-up of these drugs in blood happens slowly, patients may not realize that their intelligence, reflexes, and judgment are slowly fading, and relatives may not know the cause.
That is a lesson in the misperception of sleeping pill users. These patients were self-deceived about the value of the medication, almost deluded, thinking the medicines made them better which actually made them worse. Users of addicting sleeping pills are like heroin addicts: they may claim they need the drug, but to medical people and their own families, it looks like the addicting drugs are very harmful.
The studies showed that sleeping pills produced no long-term benefits, only harms. Also, the studies showed that the volunteers thought they were benefitting from the drugs (even placebo), even when they were being harmed.
Patients who continued to take zolpidem as-needed after two years slept worse than patients who tapered off zolpidem. [29] I would interpret these studies as indicating that continuing use of zolpidem made insomnia worse.
The manufacturers now admit that both zolpidem (Ambien) and eszopiclone (Lunesta) cause withdrawal insomnia on the night after you stop the pill. Anxiety may also occur as a withdrawal symptom. People become addicted to these drugs because they experience such anxiety and poor sleep, whenever they try to stop. If they stayed off the drug for a few days, they might sleep just as well without the medication. Even worse, newer studies indicate that with sleeping pills, drug-withdrawal damage may be surprisingly lasting. Indeed, we are not certain if the damage ever completely heals.
Disastrous side effects.
having taken Ambien, people can act like somnambulists or sleep walkers or robots gone haywire. In the more amusing examples, they may sleep-walk to the refrigerator and stuff themselves with strange foods that they would not normally eat in such quantity. Of course, this is not amusing if it leads to obesity, which can be a life-threatening condition, or if they eat something unhealthy. The behavior of the so-called Ambien Zombies is not always amusing. In a few reported cases, people intoxicated with Ambien have climbed into their cars and engaged in sleep driving. Some had serious accidents.[30] Hallucinations have been reported with zolpidem, zaleplon, and eszopiclone.[31] At other times, people receiving sleeping pills have become confused or disoriented. Another odd symptom is complete amnesia for events, even during the day. For example, a successful businessman told me that while taking Ambien at night, he might have absolutely no recollection of a conference which his own notes showed that he had attended the following day. From viewing various reports, I now realize that these terrible side effects may develop in about one percent of users of sleeping pills.
Multiple studies have found that sleeping pill use is associated with very high suicide rates, but as yet, the evidence that sleeping pills cause increased suicide is based on the strong evidence that the pills cause depression, as well as very high rates of suicide observed among those known to have taken sleeping pills.
Everyone has heard the stories of nurses awakening patients to give them sleeping pills. When I was a medical student, I learned that nurses want to keep their patients quiet for the night. Physicians routinely write sleeping pill orders in the hospital without specific medical goals, because they hate for nurses to call at night and wake the doctor up to get a sleeping pill order. As a medical student, I was instructed that if I wanted to sleep at night, I had better routinely prescribe a sleeping pill for every patient. The sleeping pill was to help the doctors and nurses sleep, not for the patients. Moreover, there is no evidence that sleeping pills really help hospital personnel at night, since sleeping pills seem to produce problems like falls and delirium that do not make the work of the night staff easier.
2.E. The problem of addiction.
All U.S.-approved prescription hypnotics are addicting (with the exception of ramelteon and the new drug Silenor). By addicting, we mean that these sleeping pills have two properties. First, when we take addicting drug such as narcotics or barbiturates, we develop tolerance so that a given dosage has less and less effect or “stops working.” People who develop tolerance are prone to increase their dosage more and more. Second, addicting drugs cause physical withdrawal symptoms when addicts try to stop. The withdrawal symptoms of hypnotics such as barbiturates and benzodiazepines are very well known.[34] Symptoms include insomnia, shakiness and tremor, nervousness and anxiety, panic, hyperactivity and increased reflexes, rapid heart rate: even epileptic seizures and death in the most severe cases.
Remarkably, even recent studies show that most people given sleeping pill prescriptions do not have complaints or diagnoses of insomnia in their medical records. This suggests that gift-giving or doctor-marketing explains much hypnotic prescribing.
2.G. Disinhibition of punished behaviors and the dark side of tranquilization.
Scientists say that benzodiazepines disinhibit punished behavior, which means that the animals become more likely to hurt themselves or to behave in a way in which they will be hurt. Another way of saying this is that benzodiazepines disinhibit aversive behaviors. There is a human analogy.
In humans, an action of benzodiazepines is to reduce fears of being harmed, which we may call being tranquilized. People very much like this feeling of reduced fear, and there is no doubt that many people like how they feel when taking benzodiazepines.
When we consider that benzodiazepines increase people’s tendency to act in a self-harmful way, it is logical that taking harmful sleeping pills may be one of the harmful behaviors which benzodiazepines tend to increase.
2.H. Infection.
Working with colleagues at Scripps Clinic, we found that people who take sleeping pills such as eszopiclone, zaleplon, and zolpidem have about a 44% higher risk of developing infections such as sinusitis, pharyngitis, upper respiratory tract infections, influenza, herpes, and so forth.[38]
A new study from Great Britain showed that use of benzodiazepines (including popular older sleeping pills) was associated with a 50% increase in hospitalizations for pneumonia and about a 30% increase in subsequent mortality. For more scientific data about infections, see this review: [39
According to those recordings, volunteers who slept 5.0 to 6.5 hours had the lowest mortality.[41] If you feel you sleep five to seven hours a night and feel rested, there is no evidence that you should try to sleep any more as far as life expectancy is concerned, and that is largely true of other health measures.
Adopting good sleep habits and attitudes is extremely effective in solving long-term sleep problems. It is more effective than sleeping pills.[42]
For help with insomnia by changing habits and attitudes, try a program of Cognitive-Behavioral Therapy for insomnia, abbreviated CBT-I.
CBTforInsomnia.com[43] and SHUTi[44],\
CBT-I helps more than sleeping pills and CBT-I is much safer.
There have now been dozens of randomized trial comparisons of CBT-I versus sleeping pills, showing that in the long run, CBT-I is more helpful and safer than sleeping pills.
In summary, there is expert consensus that the medical evidence does not support chronic use of sleeping pills.
Getting Off Sleeping Pills
Even with slow tapering, withdrawal from sleeping pills can cause at least a few nights of insomnia, anxiety (both day and night), tremulousness, and other symptoms. People will have much less difficulty withdrawing from sleeping pills if they first begin CBT-I treatment as described in Chapter 3 above, or obtain CBT-I from a therapist or web site.
Even people with no intrinsic depression or anxiety are likely to become anxious when withdrawing from a sleeping pill. It helps to understand that this anxiety and fear of insomnia is usually a drug withdrawal reaction which will go away in time, often within a day or two, so starting a replacement drug may not be advisable. People withdrawing from sleeping pills may become filled with the idea that they can never do without their pill, when a few days later, they do perfectly well without it.
The most reasonable substitute drugs might be trazodone, Silenor (doxepin 3 or 6 mg.) and melatonin, but I say this without recommending substitution. Trazodone and melatonin are not FDA-approved as hypnotics as of September, 2018.
8.A. Why haven’t you heard from the FDA?
When we reported that people who took sleeping pills died 4.6 times faster and suffered more cancer,[66]
===========================
Sun, Nov, and Aims Scopes. “Inside Insomnia: Pharmacist Management of Sleep Disorders.”
There are 5 benzodiazepines that are FDA approved for insomnia: estazolam (Prosom), flurazepam (Dalmane), quazpam (Doral), temazepam (Restoril), and triazolam (Halicon). Pharmacists can counsel patients on the use of these prescribed medications, but for many patients, insomnia can be mitigated through lifestyle modifications and appropriate sleep hygiene. “According to the CDC, some examples of good sleep hygiene include going to sleep and waking up at a consistent time every day, removing electronic devices from the bedroom, keeping the a comfortable temperature, exercising during the day—but not too late because that can keep you awake later—and avoiding large meals, caffeine, and alcohol too close to bedtime,” Khorassani explained.
Other agents such as diphenhydramine HCI (Benadryl) and doxylamine (Unisom) are also options, but they come with more adverse effects than melatonin, such as dry mouth and next-day drowsiness. Because of this, these agents are best used for short-term insomnia only.2
“I’ve had a few patients who have complained of insomnia because they were taking [the antidepressant bupropion (Wellbutrin)], which can cause insomnia,” Khorassani said. “Several of them were taking it twice daily and were taking the second dose at bedtime. If this medication is taken twice daily, the second dose is ideally given before 4 PM because of its stimulating properties.
Campbell will occasionally recommend melatonin but said she is more concerned about a patient’s sleep hygiene. Before melatonin, she will remind patients to ensure that their bedroom is optimized for sleep and that they aren’t eating too close to bedtime or drinking too much alcohol.
“If they are at the age where they are not producing as much melatonin as they need, I will put them on a very low-dose melatonin,” she said. “I incorporate a lot of nutrition science and a lot of stress science into how I approach and coach patients.”
————————————-
https://www.ncbi.nlm.nih.gov/pmc/arti...
Bruni, Oliviero, et al. “Herbal remedies and their possible effect on the GABAergic system and sleep.” Nutrients 13.2 (2021): 530.
https://scholar.google.com/scholar?ou...
Guadagna, S., et al. “Plant extracts for sleep disturbances: A systematic review.” Evidence‐Based Complementary and Alternative Medicine 2020.1 (2020): 3792390.
================================
Phototherapy: Is bright light an effective alternative for the treatment of insomnia disorders?
Phototherapy: Is bright light an effective alternative for the treatment of insomnia disorders?
14 noviembre, 2020 3:13 pm , Ciencia Cognitiva
Marc Dalmau Rodríguez
Facultad de Psicología, Universitat Oberta de Catalunya, España
In conclusion, the treatment of insomnia should follow, first and foremost, a non-pharmacological approach. Although cognitive therapy is the most effective treatment to date, its limitations in terms of involvement and abandonment must be considered. Phototherapy, on the other hand, has proven to be effective in treating insomnia, although its efficacy must be investigated in greater depth,
Click to access The_role_of_bright_light_therapy_in_mana20160326-14838-ppkd12.pdf
Lovato, Nicole, and Leon Lack. “The role of bright light therapy in managing insomnia.” Sleep Medicine Clinics 8.3 (2013): 351-359.
Chambe, Juliette, et al. “Light therapy in insomnia disorder: A systematic review and meta‐analysis.” Journal of sleep research 32.6 (2023): e13895.
Lei, Huabin, et al. “Efficacy and safety evaluation of bright light therapy in patients with post-stroke insomnia: A protocol for systematic review and meta-analysis.” Medicine 100.50 (2021): e27937.
===================================
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright (c) 2023 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on June 28th, 2024 by Jeffrey Dach MD
The post The Dangers of Sleeping Pills appeared first on Jeffrey Dach MD.
June 26, 2024
The Fear of Estrogen Part Two by Jeffrey Dach MD
 The Fear of Estrogen Part Two by Jeffrey Dach MD
The Fear of Estrogen Part Two by Jeffrey Dach MD
In part one of this series, we discussed how fear of estrogen is one of the errors of modern medicine, causing increased mortality and suffering in large numbers of menopausal women by denying them HRT (hormone replacement). To be fair, we should present the other side of the argument, and try to understand the views and positions of the other side, the estrogen denialists such as Dr. Adriane Fugh-Berman who speaks and writes extensively against the use of estrogen for menopausal women.
Above Header Image Courtesy of Wikimedia Commons, “Menopause”, Kibbutz Hagoshrim November 2011 Source Avishai Teicher via the PikiWiki – Israel free image collection project. CC 2.5
Dr. Adriane Fugh-Berman Opposition to Use of Estrogen
Firstly I must admit I greatly respect and admire Dr. Adriane Fugh-Berman who graduated from Georgetown University School of Medicine and completed a family medicine internship at Montefiore Hospital in the Bronx. She is currently Professor of Pharmacology & Physiology in the Department of Family Medicine at Georgetown University Medical Center. (1-2)
I suggest Dr. Berman is a “medical thought leader” and menopausal women look to her for advice. I must say I agree with many of her statements, such as those on the corrupting influence of the pharmaceutical industry on the practice of medicine, ghost writing, disease mongering etc. However, I would respectfully disagree with Dr. Berman’s opposition to menopausal hormone replacement expressed in her 2002 book, The Truth about Hormone Replacement Therapy : How to Break Free from the Medical Myths of Menopause. On the Amazon page for the book, Dr. Adrienne Fugh-Berman writes:
Menopause is not a disease.So why are millions of American women taking a drug [estrogen] for this natural body process? The widespread popularity of hormone replacement therapy (HRT) is a triumph of marketing and advertising over science. Although HRT and estrogen replacement therapy (ERT) can help some women with certain menopause-related problems, the benefits have been oversold to women and their health care providers. There is no scientifically valid evidence that estrogen prevents heart disease, colon cancer, or Alzheimer’s. Nor is there any evidence that it keeps you looking younger, preserves your sex drive, or enhances your memory. However, HRT does carry the risk of serious side effects, including certain cancers. Should you be taking such risky drugs to help you get through menopause? (3)
I would suggest the above views are in error as there are many scientifically valid studies showing estrogen prevents heart disease such as the 2012, the Danish Osteoporosis Prevention study (Schierbeck,DOPS, RCT) which showed a 52% reduction in death, admission to hospital for heart failure, and myocardial infarction in the hormone treated group. HRT yielded a 63 percent reduction in colon cancer (Rennert, 2009), the WHI (first arm, CEE+MPA) report 28 percent reduction in risk for colon cancer. HRT with estrogen and progesterone is neuroprotective with improvement in memory and cognition. There is considerable evidence of improved sex drive (libido) with HRT, especially the using the testosterone component. (7-14) (27)
Progesterone has remarkable anti-cancer effects and is mainstream conventional treatment for prevention of endometrial/ uterine cancer. Progesterone studies also show remarkable efficacy in prevention and treatment of other cancers, breast, endometrial/uterine, ovarian cancer,
prostate cancer, colon, non-small-cell lung cancer, malignant melanoma
and mesothelioma. (27)
Her Turn News Podcast 2023
In a December 2023 interview recorded as a podcast on Arlene Zaucha’s Her Turn News, Dr. Berman expresses many of her opposing views on menopausal hormone replacement, firstly claiming “menopause is not a disease”. I would disagree with this statement. Menopause is an estrogen deficiency disease which then leads to degeneration in all estrogen dependent organs and body tissues. Dr. Berman would than call this “normal aging”. If this is true, then other hormone deficiency diseases such as Addison’s, Type One Diabetes, and Hypothyroidism are all normal aging events that should not be treated with the missing hormones, cortisol, insulin and thyroid hormones. Of course we know this would not be acceptable to anyone. In my opinion, as discussed elsewhere in this book, estrogen deficiency leads to a number of degenerative diseases, such as cardiovascular disease, osteoarthritis, osteoporosis, retinal and neural degeneration, cognitive impairment, and genito-urinary syndrome with recurrent UTI’s as discussed in the Chapter on the Health Benefits of Estrogen Hormone Replacement. In my opinion, menopausal women should be offered treatment with natural human bioidentical HRT providing them with reduced mortality and a better quality of life. Menopausal HRT should be a basic tenet of OB/Gyne and family practice medicine. For the subspecialties of cardiology, rheumatology, orthopedics, neurology, and psychiatry, these specialist doctors should be prescribing HRT for their menopausal patients or at least referring them to a physician who can. How can we explain Dr. Berman’s negative attitude regarding menopausal hormone replacement? Perhaps the most significant factor is Dr. Berman does not practice medicine herself. She does not have first hand experience with menopausal women’s complaints on a day to day basis. If she treated menopausal patients, she would find her patients responding to menopausal hormone replacement by reporting symptomatic relief, and improved quality of life. Many will express gratitude. Let’s review a few of Dr. Berman’s statements in this podcast interview which targets hormone replacement for menopausal women. My response to Dr. Berman’s statement are indented.(4)
Dr. Berman : There is no medical test for menopause.
My reply: No medical test is needed since medical history of cessation of menses indicates menopause. However, in some patients a medical test would be useful, such as women who have had partial hysterectomies with removal of uterus with preservation of ovaries. In this case, marked elevation of LH and FSH hormones is a useful test indicating menopausal status, characterized by ovarian failure with low serum estrogen levels.
Dr. Berman: The only symptoms proven to be associated with menopause is hot flashes and night sweats and vaginal dryness. Most menopausal symptoms are the result of aging. In Japan, menopause is associated with joint pain.
My reply: Hot flashes, night sweats and vaginal dryness are indeed the three most often and glaring symptoms of menopause brought to medical attention. Menopausal estrogen deficiency causes joint pain and osteoarthritis not only in Japan, but also the in the U.S. and rest of the world. Many other menopausal symptoms are related to degeneration of organs and tissues resulting from estrogen deficiency such as osteoarthritis, osteoporosis with fracture risk, insomnia, mood disturbance, loss of libido, vaginal atrophy and vulvo-vaginal syndrome (chronic UTI’s), retinal degeneration, and cognitive dysfunction. To say estrogen deficiency of menopause is normal aging, and deny women estrogen treatment for menopausal symptoms is not a good idea. Why not treat these menopausal women with the most effective treatment, estrogen hormone replacement, and alleviate misery and suffering in this patient population?
Dr. Berman : estrogen alone resulted in endometrial cancer.
My reply: This is correct and I agree with Dr. Berman. There is no argument here. However, one must be careful and say it is the unopposed estrogen which causes endometrial hyperplasia and increases risk for endometrial cancer. Micronized progesterone is FDA approved for prevention of endometrial hyperplasia, and when progesterone is combined with estrogen, there is no increased risk of endometrial cancer. In the WHI study (first arm CEE+MPA) after 5.2 years, there was 17 percent reduction in endometrial cancer in the hormone treated group. (14-16)
Dr. Berman: Later on, hormones came back with a progestin added. This was meant to prevent heart disease, stroke, dementia.
My reply: Dr. Fugh-Berman’s makes three errors here. The first error is lumping together progestins with progesterone, and not differentiating between the two. The progestins such as medroxyprogestroeen (MPA) are the cause of poor health outcomes, while human bioidentical progesterone is the preferred choice, having better outcomes. Error number two is not explaining that oral estrogens cause increased coagulation and clotting, leading to DVT and stroke, while the transdermal route of delivery of estrogen does not cause clotting and stroke and is the preferred choice, avoiding the oral estrogen route of administration. The third error is not mentioning the Timing Hypothesis of Dr. Hodis which is that estrogen reduces heart attacks by 46 percent in the younger 50-60 age group as demonstrated in the 2011 WHI (second arm, estrogen alone) and more recently, in the 2012, the Danish Osteoporosis Prevention study, (DOPS RCT) study in which women receiving hormone therapy (HT) had a 52 percent reduced risk of composite cardiovascular safety outcomes, death, or hospitalization for MI or heart failure (hazard ratio [HR], 0.48) (Cho, Leslie, 2023) (Schierbeck, 2012). However, in older women starting HRT more than 10 years after menopause transition, the studies show no cardiovascular benefit. (17-18)
Dr. Berman: HERS Trial tested hormones in women who had had a heart attack. It was found there was no beneficial effect at al.
My reply: I agree with Dr. Berman. The Hers Trial used oral premarin and MPA (medroxyprogestreone) in older women with known coronary artery disease showing no cardiovascular benefit. We do not use this hormone combination of horse estrogen with a synthetic progestin. This combination is not actually women’s ovarian hormone replacement, and should never be used. Dr. Berman fails to mention that later studies such as the WHI second arm , the 2012 DOPS, KEEPS and ELITE studies all showed cardiovascular benefit of natural, ovarian hormone replacement. Dr. Berman also fails to mention that animal and human studies show cardiovascular benefit when HRT is started early, shortly after the menopausal transition. Estrogen can not reverse the established coronary artery plaques in older post menopausal women starting HRT 10 years after menopausal transition. However it is preventive before the plaques form. The message here that Dr. Berman should be advising menopausal women to start HRT early, and not to wait. (19-22)
Dr. Berman : The WHI clinical trial NIH funded under director Bernadine Healy. This trial found the risks far outweigh the benefit for menopausal hormone therapy.
Again, Dr Berman ignores and fails to mention the second arm of the WHI estrogen alone which showed women in the 50-59 age group enjoyed dramatic reduction in mortality, myocardial infarction and heart disease risk. Dr Fugh-Berman fails to recognize the poor outcomes were seen in the first arm, associated with older age group, and use of oral estrogen (CEE) and synthetic progestins (MPA).
Dr. Berman: In terms of disease prevention, hormones should never be used for disease prevention.
This is an error. Dr. Berman is stating that hormone deficiency is not a disease. Let me ask you this: Why is it that other forms of hormone deficiency are accepted by mainstream medicine as diseases, yet Dr. Berman claims estrogen deficiency is not a disease? Insulin deficiency is found in Type One Diabetes. This is treated with a hormone called insulin. Cortisol deficiency is Addison’s disease treated with another hormone called cortisol. Thyroid deficiency is hypothyroidism, a disease treated with thyroid hormone. As mentioned above, menopausal estrogen deficiency is a disease leading to degeneration of estrogen dependent organs and tissues. Menopausal HRT with natural, human (bioidentical) estrogen, progesterone, testosterone should be used for prevention and treatment of osteoarthritis, osteoporosis, coronary artery disease, genito-urinary syndrome, dementia, and macular degeneration.
Dr. Berman : Women should stop HRT when hot flashes stop.
This is an error. I advise women to continue HRT even after complete symptom relief to prevent onset of estrogen deficiency diseases as listed above, osteoarthriits, osteoporosis, coronary artery disease, cognitive dysfunction, vaginal dryness and genito-urinary syndrome, etc.
Dr. Berman : Estrogen increases blood clots.
I agree with this statement. However, this applies to oral estrogen, and not transdermal delivery of estrogen. Dr. Berman fails to advise women to avoid oral estrogen and instead use the transdermal delivery of estrogen which is safer and avoids the blood clotting effects of oral estrogen.
Dr. Berman: This idea that breast cancer risk is low. There is really no question that hormone therapy increases breast cancer risk.
I agree with Dr. Berman that the WHI first arm revealed increased breast cancer risk with the combination of oral estrogen (CEE) and MPA, a synthetic chemically altered version of progesterone. However, Dr Fugh-Berman fails to recognize and mention the 23 percent reduction in breast cancer in the WHI (second arm, estrogen alone). And Dr. Berman also fails to mention the 45 percent reduction in mortality from breast cancer in the 18 year follow up of this estrogen alone group. Most of her listening audience would want to know this.
Dr. Berman: If you are not having hot flashes, you don’t need medication of any sort.
Dr. Berman fails to recognize menopausal estrogen deficiency as a disease leading to degeneration of estrogen dependent organs and tissues. All post menopausal women should be offered natural human bioidentical hormone replacement.
Dr. Berman: Symptoms associated with menopause are not caused by menopause. They are caused by aging.
This is a nonsensical statement equivalent to stating symptoms of hypothyroidism are caused by aging, and therefore should not be treated. Symptoms of menopause are caused by menopausal estrogen deficiency, and untreated menopausal women are subject to increased mortality and a host of degenerative diseases. They deserve better care than calling this “aging”.
Dr. Berman: Medicalization of menopause is an industry funded campaign.
I agree with the above statement by Dr. Berman. This is called disease mongering, the medicalization of symptoms in order to create a new disease to sell a drug, merely a standard marketing practice by the drug industry. An example of this is labeling normal children as ADHD and then treating them with addictive amphetamines having the same mechanism of action as cocaine (Ritalin, Adderal, etc). In 2005, Dr. Howard Wolinsky writes:
routine human conditions—unhappiness, bone thinning, stomach aches and boredom—is increasingly being re-defined as disease: depression in its milder forms, osteoporosis, irritable bowel syndrome and attention deficit disorder. Likewise, risks factors, such as high cholesterol and high blood pressure, are declared diseases in their own right—hypercholesterolaemia and hypertension—with falling thresholds resulting in more people considered to be sick. In other cases, drugs approved for devastating illness, such as clinical depression, are indicated for milder conditions, such as shyness, which is now dubbed ‘social phobia’.(23-26)
However, in the case of menopausal symptoms treated with hormone replacement, Dr. Berman’s labeling this as drug mongering or medicalization is not justified and quite off the mark.
Dr. Berman: Low doses of antidepressant can be helpful in menopause.
It is quite surprising that Dr. Berman is usually “anti-drug industry”, yet in the above statement promotes the use of SSRI antidepressants for a hormone deficiency state. SSRI antidepressant drugs do not contain estrogen and are ineffective as a treatment for menopausal estrogen deficiency. Not only that, these drugs carry adverse side effects of emotional blunting, loss of libido and can induce psychotic or violent behavior. My advice to all women is to stay away from SSRI antidepressants, use the real thing, bioidentical hormones for the best results.
Dr. Berman: phytoestrogens in soybeans can be helpful for menopausal symptoms.
Since Dr. Berman is opposed to the use of hormone replacement, what is the symptomatic menopausal women to do? It is just sad to me that any medical thought leader would propose phytoestrogens in soy products as an effective treatment for menopausal estrogen deficiency. These products are not effective, and many of them actually block estrogen receptors making symptoms worse. (4)
Conclusion: In order to take a position opposed to the use of hormone replacement for menopausal women, one must ignore much of the medical literature on hormone replacement. Doing so usually involves believing that only RCT’s randomized controlled trials can be used as evidence, yet discarding those RCT’s that conflict with one’s position. Preclinical, animal and observational studies are all valid as scientific evidence and should be included in one’s knowledge base. When viewing the totality of the medical literature on this topic over more than 100 years, one comes to the overwhelming conclusion that natural bioidentical menopausal hormone replacement is the cornerstone for healthy menopause. When it comes to the practice of medicine, nothing is more gratifying to the doctor than prescribing menopausal hormone replacement. The dramatic improvement in quality of life we see in the patient is simply miraculous. What else in medicine can compare to this? Perhaps modern cataract surgery with lens implant with its dramatic recovery of vision comes close. My advice to Dr. Berman is this: Try prescribing HRT for your menopausal patients. You will be pleasantly surprised with the results.
Articles with Related Interest:
Errors in Modern Medicine: The Fear of Estrogen Part One
Health Benefits of Menopausal Hormone Replacement
All Bioidentical Hormone Articles
References:
1) Adriane Fugh-Berman Professor of Pharmacology & Physiology M.D.
Georgetown University, 1988 The primary areas of research for Dr. Fugh-Berman are pharmaceutical marketing practices and the culture of medicine. She directs PharmedOut, a Georgetown-based project that advances evidence-based prescribing and educates healthcare professionals about pharmaceutical marketing practices. Dr Fugh Berman also studies the benefits and risks of complementary and alternative medicine (CAM), especially herbs and dietary supplements. She has a particular interest in herb-drug interactions. Dr. Fugh-Berman maintains medicinal herb gardens on the Georgetown campus, and directs the Urban Herbs project.
2) Adriane J Fugh-Berman SOM Medical Educator Track — Professor
Bio and Featured Works
Adriane Fugh-Berman, MD is a Professor of Pharmacology and Physiology with a joint appointment in the Department of Family Medicine at Georgetown University Medical Center. Dr. Fugh-Berman co-directs the M.S. program in Health and the Public Interest and directs PharmedOut, a GUMC research and education project that promotes rational prescribing, exposes the effect of pharmaceutical marketing on prescribing practices and has had a profound impact on prescribers’ perceptions of the adverse consequences of industry marketing.
Previously, Dr. Fugh-Berman was a medical officer in the Contraception and Reproductive Health Branch of the National Institute for Child Health and Human Development, NIH. She has also worked with the nonprofit Reproductive Toxicology Center and edited an award-winning CME newsletter on women’s health.
Dr. Fugh-Berman graduated from Georgetown University School of Medicine and completed a family medicine internship in the Residency Program in Social Medicine at Montefiore Hospital in the Bronx.
3) The Truth about Hormone Replacement Therapy : How to Break Free from the Medical Myths of Menopause by Adrienne Fugh-Berman and National Women’s Network Staff (2002, Trade Paperback) Dr. Berman writes:
Menopause is not a disease.So why are millions of American women taking a drug [estrogen] for this natural body process? The widespread popularity of hormone replacement therapy (HRT) is a triumph of marketing and advertising over science. Although HRT and estrogen replacement therapy (ERT) can help some women with certain menopause-related problems, the benefits have been oversold to women and their health care providers. There is no scientifically valid evidence that estrogen prevents heart disease, colon cancer, or Alzheimer’s. Nor is there any evidence that it keeps you looking younger, preserves your sex drive, or enhances your memory. However, HRT does carry the risk of serious side effects, including certain cancers. Should you be taking such risky drugs to help you get through menopause?
Menopause is not a disease.So why are millions of American women taking a drug for this natural body process? The widespread popularity of hormone replacement therapy (HRT) is a triumph of marketing and advertising over science. Although HRT and estrogen replacement therapy (ERT) can help some women with certain menopause-related problems, the benefits have been oversold to women and their health care providers. There is no scientifically
The authors disagree with the widely promoted message that nearly all perimenopausal women should use HRT for cardiovascular and bone health or to modulate health problems associated with that stage of life; they argue that, except for a very small percentage of women, using alternative therapies is preferred. They also report on studies of HRT and provide a wealth of information. While their analytical and cautious approach is commendable, their words are often provocative e.g., they claim that the drug companies “play on women’s fears,” utilize “scare tactics,” and “artfully persuade.” Within the profusion of books on HRT on the market today, this one stands out not because of its advocacy of alternative treatments but because it is so vehement in its criticism of the medical and pharmaceutical establishments.
4) Menopause is not a disease. December 10, 2023 by Her Turn News podcast audio recording of interview. Link using Wayback Machine
Here’s a news ‘hot flash’ for you: menopause is not a disease. Menopause is not a disability — but you might think so if you’ve been paying attention to the new marketing push targeting mid-life women. We have a feminist take on the natural process for mid-life women. Her Turn reporter Arlene Zaucha talks to a longtime feminist health activist Dr, Adriane Fugh Berman about the issue. Dr. Fugh Berman runs Pharmed Out, which has more information at pharmedout.org.
Errors
1) Dr. Berman : There is no medical test for menopause.
Marked elevation of LH and FSH hormones indicates menopausal state characterized by ovarian failure and low estrogen levels.
Dr. Berman : The only symptoms proven to be associated with menopause is hot flashes and night sweats and vaginal dryness. Most menopausal symptoms are the result of aging. In Japan, menopause is associated with joint pain.
estrogen deficiency also causes joint pain, osteoarthritis, bone loss, osteoporosis, increased fracture risk, insomnia, loss of libido, vaginal atrophy and vulvo-vaginal syndrome.
(chronic UTI’s)
Dr. Berman : estrogen alone resulted in endometrial cancer.
This is correct
Dr. Berman : Later on , hormones came back with a progestin added. This was meant to prevent heart disease, stroke, dementia. All things we now know hormones dont health and in fact increase.
Dr Fugh-Berman’s error is lumping together Progestins with progesterone, and not differentiating between the two. The progestins are the cause of poor health outcomes, while human bioidentical hormones estrogen are associated with good health outcomes.
Dr. Berman : HERS Trial tested hormones in women who had had a heart attack. It was found there was no beneficial effect at al.
Dr. Berman : WHI clinical trial NIH funded under Bernadine Healy. This trial found the risks far outweigh the benefit for menopausal hormone therapy.
Again, Dr Fugh-Berman fails to recognize the poor outcomes were from use of synthetic progestins in the WHI. Dr Berman ingnores the second arm of the WHI estrogen alone which showed women in the 50-59 age group enjoyed dramatic reduction in myocardial infarction and heart disease risk.
Dr. Berman’s Error: “In terms of disease prevention, Hormones should never be used for disease prevention.”
This is wrong. Bioidentical Hormones, estrogen, progesterone, testosterone are used, and should be used to prevent estrogen deficiency diseases of osteoarthritis, osteoporosis, heart disease, and dementia, macular degeneration and cancer prevention.
Dr. Berman : “Women should stop HRT when hot flashes stop.” This is an error.
Dr. Berman : Error:”Estrogen increases blood clots”
Oral estrogen does,. Transdermal does not. Failure to say transdermal estrogen does not increase blood clots and is preferred over oral estrogen.
New York times criticized the WHI study.
“all these ctiticisms are from the industry?
Error: Dr Fugh-Berman fails to recognize and mention the positive health outcomes of the 2nd arm (premarin alone) WHI study.
Dr. Berman : Error: “This idea that breast cancer risk is low. There is really no question that hormone therapy increases breast cancer risk.
Dr Fugh-Berman fails to recognize and mention the reduction in breast cancer in the premarin alone group. And the increased breast cancer in the progestin users.
Dr. Berman : Error: if you are not having hot flashes, you dont need medication of any sort.
Dr. Berman : Error: Symptoms associated with menopause are not caused by menopause. They are caused by aging.
Dr. Berman : Medicalization of menopause is an industry funded campaign.
This is true, as this is a standard marketing practice by the pharmaceutical industry for all drugs.
Dr. Berman : Error: Low doses of antidepressant can be helpful in menopause.
Dr. Berman : Error: phytoestrogens in soybeans can be helpful for menopausal symptoms.
Dr. Berman : Error: Hormones dont work for everyone either.
Dr. Berman : Error: Vaginal dryness can be dealt with moisturizers or topical estrogen.
———————————————————–
free pdf
5) Fugh-Berman, Adriane. “The science of marketing: How pharmaceutical companies manipulated medical discourse on menopause.” Women’s Reproductive Health 2.1 (2015): 18-23.
The case is closed. Women without symptoms should not use HT [hormones therapy]. Women with symptoms should carefully weigh benefits against risks, and, if they choose to take hormones, they should take as little as possible for as short a time as possible.
!!!!!!!!!!!!!!!!!!!!! GOOD !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
6) Fugh-Berman, Adriane, and Anthony R. Scialli. “Gynecologists and estrogen: an affair of the heart.” Perspectives in biology and medicine 49.1 (2006): 115-130.
=============================================================
7) Hodis, Howard N., and Wendy J. Mack. “Menopausal hormone replacement therapy and reduction of all-cause mortality and cardiovascular disease: it is about time and timing.” The Cancer Journal 28.3 (2022): 208-223.
Taken together, randomized controlled atherosclerosis imaging trials and animal studies strongly support the healthy endothelium hypothesis showing that HRT is more effective in maintaining vascular health rather than treating established vascular disease manifested as atherosclerosis lesions.
In two meta-analyses, Salpeter, et al. showed that relative to placebo, HRT significantly reduced all-cause mortality by 39% (95% confidence interval (CI), 5%–61%) across 30 RCTs and reduced CHD by 32% (95% CI, 4%–52%) across 23 RCTs when initiated in women <60 years of age and/or <10 years-since-menopause (Fig. 6) (24,25). On the other hand, the effect of HRT on all-cause mortality and CHD was null when initiated in women >60 years old and/or >10 years-since-menopause.
DOPS is the only randomized clinical event trial to closely replicate the populations of women in observational studies.
Schierbeck, Louise Lind, et al. “Effect of hormone replacement therapy on cardiovascular events in recently postmenopausal women: randomised trial.” Bmj 345 (2012).
Women in DOPS were on average 50 years of age and 7 months past menopause with an average BMI of 25.2 kg/m2 when randomized to HRT or no HRT.
In addition, DOPS provides the longest duration of randomized HRT than any other RCT to date. CVD was reduced by 52% (hazard ratio (HR), 0.48; 95% CI, 0.27–0.89) after 10 years of randomized HRT compared with no HRT and reduced by 39% (HR, 0.61; 95% CI, 0.39–0.94) after 16 years of total follow-up (10 years of randomized treatment and 6 years of postintervention follow-up) (Fig. 8). All-cause mortality was reduced by 43% (HR, 0.57; 95% CI, 0.30–1.08) after 10 years of randomized HRT and by 34% (HR, 0.66; 95% CI, 0.41–1.08) after 16 years of total follow-up (22).
The Salpeter, et al. meta-analyses were validated and confirmed by the Cochrane group, who also showed similar reductions in all-cause mortality (30%; 95% CI, 5% – 48%) and CHD (48%; 95% CI, 4% – 71%) in women initiating HRT <60 years old and/or <10 years-since-menopause (Fig. 7) (26).
The null effect of statin therapy on primary CVD prevention in women contrasts with that of men. With careful separation of women from men and primary from secondary prevention trials, the first sex-specific meta-analysis to analyze primary CVD prevention trials showed that statin therapy reduced CHD in men but not in women (Fig. 15, top panel) (34). All-cause mortality was neither reduced in men nor women in primary CVD prevention RCTs. This latter meta-analysis included the Management of Elevated Cholesterol in the Primary Prevention Group of Adult Japanese (MEGA) trial in which 5,356 women were treated for more than 5 years (35).
The most recent primary CVD prevention RCT with statin therapy conducted in a large cohort of 5,874 women, the Heart Outcomes Prevention Evaluation-3 (HOPE-3 trial), is consistent with the sex-specific meta-analyses showing that statin therapy significantly reduces CHD in men but does not statistically significantly reduce CHD in women in primary CVD prevention and has no effect on all-cause mortality in either sex
The consistency across individual primary CVD prevention RCTs and sex-specific meta-analyses shows that statin therapy does not statistically significantly reduce all-cause mortality or CHD in women when administered for primary CVD prevention.
On the other hand, HRT is well-known to reduce new onset diabetes mellitus by 20%–30% (Fig. 18). The anti-diabetogenic effect of HRT has been shown across many independent RCTs and meta-analyses including an analysis of 107 RCTs (68–71).
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
menopausal HRT is unique in that it reduces all-cause mortality and CVD when initiated in women <60 years of age and/or <10 years-since-menopause. These cumulated findings from RCTs are consistent with the large body of observational studies that consistently show a reduction of all-cause mortality and CVD in young women who initiate HRT at the time of menopause. When initiated in women in their 50s and continued for 5–30 years, HRT reduces all-cause mortality and cost-effectively increases quality adjusted life-years (QALYs)
8) Schierbeck, L. “Primary prevention of cardiovascular disease with hormone replacement therapy.” Climacteric 18.4 (2015): 492-497.
9) Rennert, Gad, et al. “Use of hormone replacement therapy and the risk of colorectal cancer.” Journal of clinical oncology 27.27 (2009): 4542.
10) Ali, Noor, et al. “The role of estrogen therapy as a protective factor for Alzheimer’s disease and dementia in postmenopausal women: A comprehensive review of the literature.” Cureus 15.8 (2023).
11) Salinero, Abigail E., et al. “Brain Specific Estrogen Ameliorates Cognitive Effects of Surgical Menopause in Mice.” bioRxiv (2023).
12) Russell, Jason K., Carrie K. Jones, and Paul A. Newhouse. “The role of estrogen in brain and cognitive aging.” Neurotherapeutics 16 (2019): 649-665.
13) Uloko, Maria, et al. “The clinical management of testosterone replacement therapy in postmenopausal women with hypoactive sexual desire disorder: a review.” International journal of impotence research 34.7 (2022): 635-641.
========================================
14) Writing Group for the Women’s Health Initiative Investigators. “Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial.” Jama 288.3 (2002): 321-333.
15) Cagnacci, Angelo, and Martina Venier. “The controversial history of hormone replacement therapy.” Medicina 55.9 (2019): 602.
16) Woodruff, J. Donald, James H. Pickar, and Menopause Study Group. “Incidence of endometrial hyperplasia in postmenopausal women taking conjugated estrogens (Premarin) with medroxyprogesterone acetate or conjugated estrogens alone.” American Journal of Obstetrics and Gynecology 170.5 (1994): 1213-1223.
============================
17) Cho, Leslie, et al. “Rethinking menopausal hormone therapy: for whom, what, when, and how long?.” Circulation 147.7 (2023): 597-610.
18) Schierbeck, Louise Lind, et al. “Effect of hormone replacement therapy on cardiovascular events in recently postmenopausal women: randomised trial.” Bmj 345 (2012).
======================
19) Grady, D., Herrington, D., Bittner, V., et al. (2002). Cardiovascular disease outcomes during 6.8 years of hormone therapy heart and estrogen/progestin replacement study follow-up (HERS II). Journal of the American Medical Association, 288, 49–57.
20) Hulley, S., Furberg, C., Barrent-Connor, E., et al. (2002). Noncardiovascular disease outcomes during 6.8 years of hormone therapy heart and estrogen/progestin replacement study follow-up (HERS II). Journal of the American Medical Association, 288, 58–66.
21) Grady, D., Applegate, W., Bush, T. L., et al. (1998). Heart and estrogen/progestin replacement study (HERS): Design, methods and baseline characteristics. Controlled Clinical Trials, 19, 314–335.
22) Hulley, S., Grady, D., Bush, T., et al. (1998). Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. Journal of the American Medical Association, 280, 605–613.
================================
23) Wolinsky, Howard. “Disease mongering and drug marketing: Does the pharmaceutical industry manufacture diseases as well as drugs?.” EMBO reports 6.7 (2005): 612-614.
24) Kaczmarek, Emilia. “Promoting diseases to promote drugs: the role of the pharmaceutical industry in fostering good and bad medicalization.” British Journal of Clinical Pharmacology 88.1 (2022): 34-39.
25) Cetel, Jason S. “Disease-branding and drug-mongering: Could pharmaceutical industry promotional practices result in tort liability.” Seton Hall L. Rev. 42 (2012): 643.
26) Moynihan, Ray, et al. “Selling sickness: the pharmaceutical industry and disease mongering Commentary: Medicalisation of risk factors.” Bmj 324.7342 (2002): 886-891.
27) Lieberman, Allan, and Luke Curtis. “In defense of progesterone: a review of the literature.” Alternative Therapies in Health & Medicine 23.7 (2017).
============================================
Estrogen Causes Breast Cancer
===========================================
Henderson, Brian E., R. K. Ross, and Leslie Bernstein. “Estrogens as a cause of human cancer: the Richard and Hinda Rosenthal Foundation award lecture.” Cancer research 48.2 (1988): 246-253.
Henderson, Brian E., R. K. Ross, and Leslie Bernstein. “Estrogens as a cause of human cancer: the Richard and Hinda Rosenthal Foundation award lecture.” Cancer research 48.2 (1988): 246-253.
https://joe.bioscientifica.com/downlo...
194) Turan, V. K., et al. “The effects of steroidal estrogens in ACI rat mammary carcinogenesis: 17β-estradiol, 2-hydroxyestradiol, 4-hydroxyestradiol, 16α-hydroxyestradiol, and 4-hydroxyestrone.” Journal of endocrinology 183.1 (2004): 91-99.
Yager, James D., and Nancy E. Davidson. “Estrogen carcinogenesis in breast cancer.” New England Journal of Medicine 354.3 (2006): 270-282.
conclusions
Studies of breast cancer have consistently found an increased risk associated with elevated blood levels of endogenous estrogen, clinical indicators of persistently elevated blood estrogen levels, and exposure to exogenous estrogen plus progestin through hormone-replacement therapy and the use of oral contraceptives. In experimental animals, estrogen treatment leads to the development of mammary tumors. Together, these observations support the hypothesis that estrogen is a mammary-gland carcinogen.
The mechanisms through which estrogens contribute to each phase of the carcinogenic process (initiation, promotion, and progression) are complex. The evidence suggests the participation of genotoxic estrogen metabolites and estrogen-receptor–mediated genomic and nongenomic signaling that affect cell proliferation and apoptosis in mammary tissue. The extent to which these two pathways
contribute to estrogen-mediated carcinogenesis and the ways by which genetic polymorphisms and environmental factors modify the effects of these pathways require further exploration. Even so, knowledge of the central role of estrogen in breast cancer has already led to the development of new preventive and therapeutic interventions that block receptor function or drastically reduce the levels of endogenous estrogen through the inhibition of its synthesis. The development of additional strategies on the basis of the inhibition of estrogen metabolism, inactivation of the reactive quinones, and specific inhibition of membrane estrogen-receptor– activated second-messenger pathways will probably lead to the availability of additional effective intervention approaches.
https://www.ncbi.nlm.nih.gov/pmc/arti...
Russo, J. I. H. R., and Irma H. Russo. “The role of estrogen in the initiation of breast cancer.” The Journal of steroid biochemistry and molecular biology 102.1-5 (2006): 89-96.
17-β-estradiol is able to induce complete neoplastic transformation of human breast epithelial cells, as proven by the formation of tumors in SCID mice. This model demonstrates a sequence of chromosomal changes that correlates with specific stages of neoplastic progression. The data also support the concept that 17-β-estradiol can act as a carcinogenic agent without the need of the ERα, although we cannot rule out thus far the possibility that other receptors such as ERβ, or other mechanisms could play a role in the transformation of human breast epithelial cells. These are areas of active research in our laboratory. The knowledge that breast cancer in women is associated with prolonged exposure to high levels of estrogens gives relevance to this model of estrogen induced carcinogenesis (6,8-10,15,16). For this reason this model is extremely valuable for furthering our understanding of estrogen induced carcinogenicity.
Published on June 26th, 2024 by Jeffrey Dach MD
The post The Fear of Estrogen Part Two by Jeffrey Dach MD appeared first on Jeffrey Dach MD.
June 2, 2024
Peter McCullough MD on Art of War and Big Pharma

Peter McCullough MD on Art of War and Big Pharma May 17, 2024
[In this talk, Dr. Peter McCullough discusses] what happened in the last four years and the “Art of War” in a time where we are looking for who to trust and what information to believe about health, geopolitics, and virtually every aspect of our lives… The public now understands they were deceived by a narrative from the Bio-Pharmaceutical Complex, a syndicate of government agencies, NGO’s, and pharmaceutical companies that stymied them in order to carry out a psychological operation that led to tragic health consequences. Virtually every major public health initiative during the pandemic was completely wrong and dangerous. Therapeutic nihilism, fraud, and corruption swept into medicine. end quote Dr. McCullough.
Please enjoy this 90 minute stage presentation which was the third in a lecture series on the Art of War hosted by Pastor Frank Ramseur at the Calvary Chapel in Chattanooga, TN. Header Image: Courtesy of Peter McCullough MD and Courageous Discouse.
Click Here for the 90 minute video:
A Global Simultaneous, Great Medical Controversy Dr. McCullough Fought to Preserve Life while the Bio-Pharmaceutical Complex Used Tactics from the Art of War Peter A. McCullough, MD, MPH Jun 01, 2024 By Peter A. McCullough, MD, MPH
Click Here for the Slides that go with the talk:
Dr. Peter McCullough’s Power Point Presentation:
The Art of War is a Chinese military treatise dating from roughly 5th century BC. The work, which is attributed to the ancient Chinese military strategist Sun Tzu (“Master Sun”), is composed of 13 chapters. Each one is devoted to a different set of skills or art related to warfare and how it applies to military strategy and tactics. The book contains a detailed explanation and analysis of the 5th-century BC Chinese military featuring strategy and discipline. Sun also stressed the roles of intelligence operatives and espionage to the war effort. An important strategy was to deceive, incite division, and break unity among enemies. Considered one of history’s finest military tacticians and analysts, his teachings and strategies formed the basis of advanced military training throughout the world.
The lecture series name is applicable because the entire world was subjected to a PSYOP from the Bio-Pharmaceutical Complex that used deceptive tactics to create fear, confusion, and suffering that worked to sow division among families, churches, schools, and communities. Once divided, we faced casualties in the form of injury, disability, and death after SARS-CoV-2 infection and COVID-19 vaccination.
My message was one of unity for people around the globe as we navigate in the fifth year of the crisis. My central presentation themes included treatment of disabilities and preservation of life in the vaccinated while the greatest audience concerns focused on prosecution of perpetrators and justice for crimes committed against humanity. Several in the audience had personal losses due to therapeutic nihilism during acute COVID-19 treatment or fatal syndromes after COVID-19 vaccination.
Please subscribe to Courageous Discourse as a paying or founder member so we can continue to bring you the truth.
Peter A. McCullough, MD, MPH, President, McCullough Foundation, www.mcculloughfnd.org
==========================================================
Dr. Peter McCullough: ‘Art Of War’ Series: Who Is Winning The War Of Information? (Full Talk)
Who is Winning the War of Information?
Dr. McCullough On Stage in “Art of War” Series, Calvary Chapel, Chattanooga
By Peter A. McCullough, MD, MPH, May 19, 2024
Recently, I made a stage presentation to a large crowd at the Calvary Chapel in Chattanooga, TN. The last time I was there was December, 2021, in the heat of the pandemic, and the crowd pressed me then for the best treatment protocols at home to survive acute COVID-19. I credited Pastor Frank Ramseur for being correct from the beginning on masking, lockdowns, early treatment, and vaccines. The community needs to know when their leaders made the right calls and had the courage to hold strong.
Now I was back in Chattanooga on May 17, 2024, but the conversation was much different. It was about what happened in the last four years and the “Art of War” in a time where we are looking for who to trust and what information to believe about health, geopolitics, and virtually every aspect of our lives.
The audience confirmed that not a single public health agency, medical school, or hospital system held public forums so people could ask questions and have their concerns addressed. I took over an hour to answer every question in the room from open microphones on both ends.
The public now understands they were deceived by a narrative from the Bio-Pharmaceutical Complex, a syndicate of government agencies, NGO’s, and pharmaceutical companies that stymied them in order to carry out a psychological operation that led to tragic health consequences. Virtually every major public health initiative during the pandemic was completely wrong and dangerous. Therapeutic nihilism, fraud, and corruption swept into medicine.
I gave the audience a few tips to probe on the trust issue with doctors and nurses by asking questions.
1. How many COVID-19 vaccines they personally take and why they stopped?
2. Do they still recommend boosters now? Why?
3. Did they treat ambulatory COVID-19 in 2020 and beyond? Why not?
4. Do they have an remorse with an apology to offer?
If you are stonewalled on these four, or if worse, if you are pressed with the relentless narrative from the Bio-Pharmaceutical Complex, the Art of War would say to find new allies to be at your side as we gear up for the next battle.
Dr. Peter McCullough’s Power Point Presentation:
……………..
Dr. Peter McCullough videos featured on this Rumble channel:
The Courage To Face COVID-19:
Preventing Hospitalization And Death While Battling The Bio-Pharmaceutical Complex (Book)
By John Leake and Dr. Peter McCullough
Dr. Peter McCullough on X
Tweets by P_McCulloughMD
Dr. Peter McCullough on Substack
https://petermcculloughmd.substack.com/
Dr. Peter McCullough Website
https://www.petermcculloughmd.com/
Dr. Peter McCullough Resource Page
………………
COVID-19 Vaccine Injuries & Deaths
Increasing Death Rates, Plummeting Birth Rates, Sudden Adult Death Syndrome
Increasing Death Rates, Plummeting Birth Rates, Sudden Adult Death Syndrome (SADS)
Sudden Deaths, Excess Deaths, Plummeting Birth Rates on Rumble
https://rumble.com/playlists/diFxxaBXWgY
Study Finds Staggering 17 Million Global Deaths After Covid Jab Rollout (Rancourt, Baudin & Mercier)
Denis Rancourt videos on Rumble
https://rumble.com/playlists/egGCGix2XII
Collection Of Peer Reviewed Case Reports & Studies Citing Adverse Effects Post Covid Vaccination
https://react19.org/science
Covid-19 Vaccine Pharmacovigilance Report
https://worldcouncilforhealth.org/res...
More Than 1,000 Peer Reviewed Articles On COVID Vaccine Injuries
COMPILATION: PEER REVIEWED MEDICAL PAPERS OF COVID VACCINE INJURIES
The Statistical Trick That Made It Look Like Unvaccinated People Fared Worse Than Vaccinated People
COVID-19 Vaccination Stories, Side Effects & Healing
COVID-19 Vaccination Death & Injury Stories From Around The World
COVID-19 Vaccine Death & Injury Stories on Rumble
https://rumble.com/playlists/UtGOH2S6pVo
COVID-19 Vaccine Adverse Event Tracking System (VAERS)
COVID-19 Vaccine Bad Batches Reference Page
Bad Batches / Hot Lots on Rumble
https://rumble.com/playlists/N5UFz_VBbaE
Covid-19 – Vaccine-Induced T Cell Suppression, Virus Activation, Cancer, Parkinson’s, Alzheimer’s
Covid-19 – Vaccine-Induced T Cell Suppression, Virus Activation, Cancer, Parkinson’s, Alzheimer’s
Vaccine-Induced “Turbo Cancer”
https://rumble.com/search/all?q=sunfe...
Vaccine-Induced Cancer & Turbo Cancer on Rumble
https://rumble.com/playlists/dtgIqdwOPYY
COVID-19 Menstrual & Breast Milk Disruptions, Miscarriages, Infertility, Shedding, DNA Contamination
COVID-19 Menstrual & Breast Milk Disruptions, Miscarriages, Infertility, Shedding, DNA Contamination
Shedding videos on Rumble
https://rumble.com/playlists/ILbbXTB09dw
COVID-19 Vaccines For Children (& Childhood Vaccines In General) on Rumble
https://rumble.com/playlists/A87UF7Dy_Qc
COVID-19 Psychosis
COVID-19 – Mystery Clots In Vaccinated Deceased People
Blood Clots, Vaccinated Blood, Autopsies
https://rumble.com/playlists/FbkcPTknHGA
Has Our Blood Supply Been Contaminated By Vaccinated, Genetically-Modified Blood?
Has Our Blood Supply Been Contaminated By Vaccinated, Genetically-Modified Blood?
COVID-19 Healing Resources
How To Heal COVID Vaccine Injuries on Rumble
https://rumble.com/playlists/RaQVQsmVSS8
Published on June 2nd, 2024 by Jeffrey Dach MD
The post Peter McCullough MD on Art of War and Big Pharma appeared first on Jeffrey Dach MD.
May 28, 2024
New BMJ Study Creates Doubts About Omega-3 Fish Oil
 New BMJ Study Creates Doubts About Omega-3 Fish Oil
New BMJ Study Creates Doubts About Omega-3 Fish Oil
by Jeffrey Dach MD
A new BMJ study by Dr. Chen (2024) on Omega-3 Fish Oil and cardiovascular disease merely creates confusion among the population. The problem is this new BMJ study is “junk science”, a prospective cohort study with bizarre endpoints that merely confuse the issue. This 2024 BMJ study by Chen should be unceremoniously placed into the garbage can.
Here is the Correct Information:
For the correct information see this recent study by Dr. ShiChun Shen, (2022), a meta-analysis of 14 Randomized Clinical Trials shows Omega 3 fish oils are very beneficial in preventing cardiovascular death. This meta-analysis includes 14 Randomized Clinical Trials with 135,291 subjects, finding that Omega-3 Fish Oils reduces risk of heart attack and cardiovascular death. (1-4)
Conclusion: Fourteen Randomized Controlled Trials showing cardiovascular benefit of Omega-3 Fish-Oils trumps one negative prospective observational study.
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Header Image: Courtesy of Wikimedia Commons English: Salmon oil capsule. Salmon oil capsules contain salmon oil, which is extracted from salmon and is primarily in capsules available, as it has a very strong odor. Salmon oil has a high content of triglycerides, which contain omega-3 fatty acid residues. Date 27 February 2016, 22:32:49 Source Own work
Author Marco Almbauer. This file is licensed under the Creative Commons Attribution-Share Alike 4.0 International license.
References:
1) https://bmjmedicine.bmj.com/content/3/1/e000451.abstract
Chen, Ge, et al. “Regular use of fish oil supplements and course of cardiovascular diseases: prospective cohort study.” BMJ Medicine 3.1 (2024).
For people with a healthy cardiovascular profile, regular use of fish oil supplements, a choice of primary prevention, was associated with an increased risk of atrial fibrillation. For participants with a diagnosis of atrial fibrillation, however, regular use of fish oil supplements, as secondary prevention, had a protective effect or no effect on transitions from atrial fibrillation to major adverse cardiovascular events, atrial fibrillation to death, and major adverse cardiovascular events to death. When we divided major adverse cardiovascular events into three individual diseases (ie, heart failure, stroke, and myocardial infarction), we found associations that could suggest a mildly harmful effect between regular use of fish oil supplements and transitions from a healthy cardiovascular state to stroke, whereas potential beneficial associations were found between regular use of fish oil supplements and transitions from atrial fibrillation to myocardial infarction, atrial fibrillation to death, and heart failure to death.
Objective To examine the effects of fish oil supplements on the clinical course of cardiovascular disease, from a healthy state to atrial fibrillation, major adverse cardiovascular events, and subsequently death.
Design Prospective cohort study.
Setting UK Biobank study, 1 January 2006 to 31 December 2010, with follow-up to 31 March 2021 (median follow-up 11.9 years).
Participants 415 737 participants, aged 40-69 years, enrolled in the UK Biobank study.
Main outcome measures Incident cases of atrial fibrillation, major adverse cardiovascular events, and death, identified by linkage to hospital inpatient records and death registries. Role of fish oil supplements in different progressive stages of cardiovascular diseases, from healthy status (primary stage), to atrial fibrillation (secondary stage), major adverse cardiovascular events (tertiary stage), and death (end stage).
Results Among 415 737 participants free of cardiovascular diseases, 18 367 patients with incident atrial fibrillation, 22 636 with major adverse cardiovascular events, and 22 140 deaths during follow-up were identified. Regular use of fish oil supplements had different roles in the transitions from healthy status to atrial fibrillation, to major adverse cardiovascular events, and then to death. For people without cardiovascular disease, hazard ratios were 1.13 (95% confidence interval 1.10 to 1.17) for the transition from healthy status to atrial fibrillation and 1.05 (1.00 to 1.11) from healthy status to stroke. For participants with a diagnosis of a known cardiovascular disease, regular use of fish oil supplements was beneficial for transitions from atrial fibrillation to major adverse cardiovascular events (hazard ratio 0.92, 0.87 to 0.98), atrial fibrillation to myocardial infarction (0.85, 0.76 to 0.96), and heart failure to death (0.91, 0.84 to 0.99).
Conclusions Regular use of fish oil supplements might be a risk factor for atrial fibrillation and stroke among the general population but could be beneficial for progression of cardiovascular disease from atrial fibrillation to major adverse cardiovascular events, and from atrial fibrillation to death. Further studies are needed to determine the precise mechanisms for the development and prognosis of cardiovascular disease events with regular use of fish oil supplements.
=========================================
This study lends further support for use of Fish oil…..
2) https://hal.science/hal-03486871/document
Bellenger, Jérôme, et al. “N-3 polyunsaturated fatty acids: an innovative strategy against obesity and related metabolic disorders, intestinal alteration and gut microbiota dysbiosis.” (2019): 66-71.
Dietary n-3 PUFAs, affecting gut integrity, have been shown to reduce clinical colitis and colonic immunopathology by improving epithelial barrier function in animal models (37,38). EPA has been shown to up-regulate the expression of tight junctions and to increase the trans-epithelial electrical resistance (TER), thus reducing the permeability of the endothelial cells (39). EPA and DHA, by lowering permeability-induced inflammatory cytokines such as TNFa, IFNg and IL-4, can maintain gut barrier integrity (40, 41). In agreement, it has been shown that, following intravenous injections of E. coli LPS to animal models, dietary DHA supplementation significantly enhanced the expression of intestinal tight junctions as occludin and claudin-1 and decreased intestinal expression of TLR4 (42). Very few studies assessed the impact of n-3 fatty acids on metabolic endotoxemia. Nevertheless, Mani and co-workers (43) have shown in pigs that post-prandial endotoxemia was decreased by fish oil supplementation when it was increased by coconut oil (rich in saturated fatty acids). Recently,
enhanced levels of metabolic endotoxemia and systemic low-grade inflammation were observed in high n-6 PUFA-fed mice, whereas these parameters are drastically reduced in transgenic mice able to convert n-6-to-n-3 PUFAs in their tissues (44).
==================================
This is an animal study in 24 pigs first fed saturated fat to induce leaky gut, endotoxemia, and increased LPS in blood stream. The pigs were then fed omega 3 oils (marine fish oil) n-3 polyunsaturated fatty acids (PUFA) which reduced the endotoxemia by 50 percent. If cardiovascular disease is a result of endotoxemia, as I believe it is, then Marins fish oil (Omega3 oils) are beneficial, as long as the product is fresh and not rancid. And as long as the product is not contaminated with mercury heavy metals which go directly to the heart muscle and cause arrhythmia and CHF.
============================================================================
Further support for Omega 3 oils for prevention of cardiovascular disease…
3) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3577458/
Mani V, Hollis JH, & Gabler NK (2013) Dietary oil composition differentially modulates intestinal endotoxin transport and postprandial endotoxemia. Nutrition & Metabolism (Lond) 10(1):6.
Intestinal derived endotoxin and the subsequent endotoxemia can be considered major predisposing factors for diseases such as atherosclerosis, sepsis, obesity and diabetes.
We hypothesized that oils rich in saturated fatty acids (SFA) would augment, while oils rich in n-3 polyunsaturated fatty acids (PUFA) would attenuate intestinal endotoxin transport and circulating concentrations.
Postprandial endotoxemia was measured in twenty four pigs following a porridge meal made with either water (Control), fish oil (FO), vegetable oil (VO) or coconut oil (CO). Blood was collected at 0, 1, 2, 3 and 5 hours postprandial and measured for endotoxin. Furthermore, ex vivo ileum endotoxin transport was assessed using modified Ussing chambers and intestines were treated with either no oil or 12.5% (v/v) VO, FO, cod liver oil (CLO), CO or olive oil (OO). Ex vivo mucosal to serosal endotoxin transport permeability (Papp) was then measured by the addition of fluorescent labeled-lipopolysaccharide.
Postprandial serum endotoxin concentrations were increased after a meal rich in saturated fatty acids and decreased with higher n-3 PUFA intake. Compared to the no oil control, fish oil and CLO which are rich in n-3 fatty acids reduced ex vivo endotoxin Papp by 50% (P ================================
This meta-analysis included 14 Randomized Clinical Trials including 1,35,291 subjects, finding Omega-3 Fish Oils reduced risk of heart attacks….
4) https://www.frontiersin.org/articles/10.3389/fnut.2022.809311/full
Shen, ShiChun, et al. “Omega-3 fatty acid supplementation and coronary heart disease risks: a meta-analysis of randomized controlled clinical trials.” Frontiers in nutrition 9 (2022): 809311.
Results: This meta-analysis included 14 clinical RCTs, including 135,291 subjects. Omega-3 FA supplementation reduced the risk of MACE (RR; 0.95; CI: 0.91–0.99; p for heterogeneity 0.27; I2 = 20%; p = 0.03), cardiovascular death (RR; 0.94; CI: 0.89–0.99; p for heterogeneity 0.21; I2 = 25%; p = 0.02), and MI (RR; 0.86; CI: 0.79–0.93; p for heterogeneity 0.28; I2 = 19%; p < 0.01), but had no significant effect on all-cause death, stroke, and revascularization.
In the subgroup analysis, omega-3 FA supplementation decreased the incidence of MACE [Major Adverse Cardiac Event] and cardiovascular death in acute patients with MI, the risk of MI and stroke in patients with CHD, and the risk of MI in patients with high-risk CHD. 0.8–1.2 g omega-3 FA supplementation reduced the risk of MACE, cardiovascular death, and MI.
Conclusions: Omega-3 FA supplementation had a positive effect in reducing the incidence of MACE, cardiovascular death, MI. Regardless of the stage of CHD, omega-3 FA supplementation can prevent the occurrence of MI. The 0.8–1.2 g omega-3 FA supplementation alleviated CHD risk more effectively than lower or higher doses.
==============================================
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright (c) 2023 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on May 28th, 2024 by Jeffrey Dach MD
The post New BMJ Study Creates Doubts About Omega-3 Fish Oil appeared first on Jeffrey Dach MD.
May 14, 2024
AntiCancer Effects of Hydrogen Gas Inhalation
 AntiCancer Effects of Hydrogen Gas Inhalation by Jeffrey Dach MD
AntiCancer Effects of Hydrogen Gas Inhalation by Jeffrey Dach MD
Remission of Extensive Brain Mets with Inhalation of Hydrogen Gas
Case Number One: A 51-year-old female patient was presented to medical attention with left arm pain for a month. She was diagnosed with Non-Small Cell Lung Cancer (NSCLC) with multiple brain metastases. The patient was initially treated with Gefitinib and Osimertinib with no clinical response to these two Tyrosine Kinase Inhibitor drugs.
Note: Gefitinib, an oral tyrosine kinase inhibitor (TKI) against epidermal growth factor receptor (EGFR) was FDA approved in 2015 for metastatic non-small cell lung cancer (NSCLC) whose tumors have specific mutations in the gene for the epidermal growth factor receptor (EGFR). Osimertinib is a third-generation epidermal growth factor receptor tyrosine kinase inhibitor.
Following this, the patient received 28 days of Whole Brain Radiotherapy (WBRT). One week after completing the radiation therapy, the patient worsened with severe headache, vomiting, confusion, and incontinence. At this time, follow up brain MRI scan showed explosive worsening of the metastatic brain lesions (see above header image). Above Header Image: after Whole Brain Radiotherapy with Explosive Progression of Metasatic Lesions Courtesy of Xu, Kecheng, et al. “Explosive Progression of Brain Metastases from Lung Adenocarcinoma after Radiotherapy and Significant Reversal after Inhalation of Hydrogen-Oxygen Gas: A Case Report.” Ann Med Case Rep. 2022;4(1):1032.
Following this, having exhausted all conventional treatments, there was nothing left to offer this patient. As a palliative measure, the patient was treated with hydrogen gas inhalation therapy, using a mixture of 66% Hydrogen gas and 34% Oxygen, 3 liters/min, 6 hours a day. Within a week, the patient’s condition started to improve. One month later the patient was markedly improved. Remarkably, a follow up brain MRI scan at this time showed almost complete clearing of the metastatic lesions.

Above Image: Follow Up MRI Scan of Brain 2 Months after starting Hydrogen Gas Inhalation. Almost All Metastatic Lesion Have Cleared. This was durable remission on later follow up. Courtesy of Xu, Kecheng, et al. “Explosive Progression of Brain Metastases from Lung Adenocarcinoma after Radiotherapy and Significant Reversal after Inhalation of Hydrogen-Oxygen Gas: A Case Report.” Ann Med Case Rep. 2022;4(1):1032.
===============================================
Case Number Two :
 Above images: Remarkable MRI scan documentation of disappearance of brain metastatic lesions in a patient with small cell lung cancer after treatment with hydrogen gas inhalation.
Above images: Remarkable MRI scan documentation of disappearance of brain metastatic lesions in a patient with small cell lung cancer after treatment with hydrogen gas inhalation.
Thanks and credit to Daniel Stanciu, PhD for bringing this case report to my attention. See above images before and after hydrogen gas inhalation courtesy of Chen, Jibing, et al. “Brain metastases completely disappear in non-small cell lung cancer using hydrogen gas inhalation: A case report.” OncoTargets and therapy (2019): 11145-11151.
Conclusion: These two case reports show remarkable clearing and sustained remission of metastatic brain lesions from Non Small Cell Lung Cancer (NSCLC) with inhalation of hydrogen gas, a treatment widely available with inexpensive home generators. I would like to see a larger series patients with NSCLC treated with hydrogen gas inhalation at a large tertiary care cancer referral center such as MD Anderson in Houston. Also, possible synergies with repurposed drugs could be explored with preclinical studies in animal xenografts and cell cultures. For example, one wonders about synergy of hydrogen gas with mebendazole, Ivermectin, Propranolol, Dichloroacetate, Niclosamide, Melatonin, Berberine, etc in animal cancer xenograft or cell culture models.
 Cracking Cancer Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Did you like this article? You may wish to read my book: Cracking Cancer Toolkit available on Amazon.
Articles With Related Interest:
Paradoxical Prometastatic Effects of Chemotherapy
Ivermectin, Antiparasitic, Anticancer Wonder Drug
Artemisinin Our Best Cancer Weapon
All Cancer Articles by Jeffrey Dach MD on This Blog
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
References And Links
1) Xu, Kecheng, et al. “Explosive Progression of Brain Metastases from Lung Adenocarcinoma after Radiotherapy and Significant Reversal after Inhalation of Hydrogen-Oxygen Gas: A Case Report.” Ann Med Case Rep. 2022;4(1):1032.
Rationale: For multiple brain metastases complicated by Non-Small Cell Lung Cancer (NSCLC), Whole Brain Irradiation Therapy (WBRT) is the first choice for
treatment. But little is known about the explosive progression of brain metastases caused by radiotherapy and the reversal of hydrogen gas inhalation.
Patient concerns: A 51-year-old female patient was diagnosed with NSCLC with multiple brain metastases. After receiving Gefitinib and Osimertinib without
clinical response, she received 28 days of WBRT.
Diagnosis: One week after the end of WBRT, the patient’s general condition suddenly worsened, with severe headache, vomiting, confusion, and incontinence. MRI showed that the number and size of brain metastases increased explosively. Interventions and outcomes: In the absence of any special “anti-cancer” treatment available, the patient only receives hydrogen gas inhalation therapy, inhaling a mixture of hydrogen and oxygen (66% H2 and 34% O2), 3000 ml/min, at least 6 hours a day. The patient’s condition began to improve after a week, and markedly improved after one month. A reexamination of MRI showed that more than 90% of brain metastases disappeared.
Lessons: Radiotherapy is a double-edged sword. Doctors should pay attention to the adverse effects of radiotherapy, especially for brain metastases complicated
by lung cancer. Molecular hydrogen is a therapeutic gas that can selectively scavenge toxic free radicals, its role in cancer treatment is worthy of attention and
further research.
2) Chen, Jibing, et al. “Brain metastases completely disappear in non-small cell lung cancer using hydrogen gas inhalation: A case report.” OncoTargets and therapy (2019): 11145-11151.
Making Tumors Drop Off: Molecular Hydrogen Author: Daniel Stanciu, PhD Last update: Febraury 28th, 2021
Fu, Zhiling, and Jin Zhang. “Molecular hydrogen is a promising therapeutic agent for pulmonary disease.” Journal of Zhejiang University-SCIENCE B 23.2 (2022): 102-122.
Hirano, Shin-ichi, et al. “Molecular hydrogen as a novel antitumor agent: Possible mechanisms underlying gene expression.” International Journal of Molecular Sciences 22.16 (2021): 8724.
Noor, Muhammad Nooraiman Zufayri Mohd, et al. “A systematic review of molecular hydrogen therapy in cancer management.” Asian Pacific journal of cancer prevention: APJCP 24.1 (2023): 37.
Artamonov, Mikhail Yu, et al. “Molecular Hydrogen: From Molecular Effects to Stem Cells Management and Tissue Regeneration.” Antioxidants 12.3 (2023).
–
organoprotective effects;
minimization of the consequences of ischemic–reperfusion lesions;
limitation of systemic inflammatory responses;
antitumor effects;
anti-aging effects;
increasing the body’s resistance to stressors of various nature;
improved exercise tolerance.
Chen, Ji-Bing, You-Yong Lu, and Ke-Cheng Xu. “A narrative review of hydrogen oncology: from real world survey to real world evidence.” Medical Gas Research 10.3 (2020): 130.
Chen, Ji-Bing, et al. ““Real world survey” of hydrogen-controlled cancer: a follow-up report of 82 advanced cancer patients.” Medical Gas Research 9.3 (2019): 115-121.
Advanced cancer treatment is a huge challenge and new ideas and strategies are required. Hydrogen exerts antioxidant and anti-inflammatory effects that may be exploited to control cancer, the occurrence and progression of which is closely related to peroxidation and inflammation. We conducted a prospective follow-up study of 82 patients with stage III and IV cancer treated with hydrogen inhalation using the “real world evidence” method. After 3-46 months of follow-up, 12 patients died in stage IV. After 4 weeks of hydrogen inhalation, patients reported significant improvements in fatigue, insomnia, anorexia and pain. Furthermore, 41.5% of patients had improved physical status, with the best effect achieved in lung cancer patients and the poorest in patients with pancreatic and gynecologic cancers. Of the 58 cases with one or more abnormal tumor markers elevated, the markers were decreased at 13-45 days (median 23 days) after hydrogen inhalation in 36.2%. The greatest marker decrease was in achieved lung cancer and the lowest in pancreatic and hepatic malignancies. Of the 80 cases with tumors visible in imaging, the total disease control rate was 57.5%, with complete and partial remission appearing at 21-80 days (median 55 days) after hydrogen inhalation. The disease control rate was significantly higher in stage III patients than in stage IV patients (83.0% and 47.7%, respectively), with the lowest disease control rate in pancreatic cancer patients. No hematological toxicity was observed although minor adverse reactions that resolved spontaneously were seen in individual cases. In patients with advanced cancer, inhaled hydrogen can improve patients’ quality-of-life and control cancer progression. Hydrogen inhalation is a simple, low-cost treatment with few adverse reactions that warrants further investigation as a strategy for clinical rehabilitation of patients with advanced cancer. The study protocol received ethical approval from the Ethics Committee of Fuda Cancer Hospital of Jinan University on December 7, 2018 (approval number: Fuda20181207).
========================
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright (c) 2023 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on May 14th, 2024 by Jeffrey Dach MD
The post AntiCancer Effects of Hydrogen Gas Inhalation appeared first on Jeffrey Dach MD.
April 28, 2024
Spike Protein Detoxification Protocol of Dr Peter McCullough
 Spike Protein Detoxification Protocol of Dr Peter McCullough
Spike Protein Detoxification Protocol of Dr Peter McCullough
by Jeffrey Dach MD
Mike is a 62 year old hedge fund manager who took the multiple Ĉøѷϊƌ Ѷåććĩƞēs over the past three years. He was rushed to the hospital Emergency Room with chest pain, and quickly transferred to the Cardiac Catheter Laboratory where coronary angiography failed to show the cause of his chest pain. The doctors were perplexed. In any event, a stent was placed into one of the coronary arteries which was thought to be narrowed slightly. He went home and a few weeks later had another bout of chest pain. The above scenario was repeated with a quick trip back to the Cardiac Cath Lab, and again coronary angiogram showed very little findings. A second sent was placed anyway. He went home and a few weeks later, everything was repeated again. A third bout of chest pain sent him back to the hospital and a third stent was placed. And again, after he went home, he still complained of intermittent chest pain despite the three stents. The doctors were perplexed, and had nothing to further to offer the patient.
Header Image: Courtesy of McCullough, Peter A., et. al. “Clinical rationale for SARS-CoV-2 base spike protein detoxification in post COVID-19 and vaccine injury syndromes.” J Am Physicians Surg 28 (2023): 90-94.(1)
Mike’s story is typical for chest pain from myocarditis (inflammation of the heart muscle) induced by the Ĉøѷϊƌ Ѷåććĩƞē which causes ŝҏіке protein accumulation in the myocardium. Symptoms can include chest pain, as well as the more serious cardiac arrhythmia and sudden cardiac arrest. Myocardial function can be compromised leading to congestive heart failure with reduced ejection fraction. Cardiologists are willfully blind to these adverse effects of the Ĉøѷϊƌ Ѷåććĩƞēs, thus the futile repeated procedures in the Cath Lab.
The Ĉøѷϊƌ Ѷåććĩƞē is not really a Ѷåććĩƞē. It is genetic therapy which programs our cells with messenger RNA which instructs our cells to manufacture the ŝҏіке protein, an extremely toxic substance which induces an inflammatory reaction.There is no way to turn off this production, There is no “Off Switch”.
A commonly reported symptom after Ĉøѷϊƌ Ѷåććĩƞation is pain and tenderness within enlarged axillary lymph nodes which may last for months. This is caused by ŝҏіке protein accumulation within axillary lymph nodes. Unfortunately, spike protein is produced and accumulates in many other organ systems because of the lipid nanoparticle delivery vehicle. Thus, the messenger RNA delivered to the body by the Ĉøѷϊƌ Ѷåććĩƞē travels freely throughout the body and is incorporated into cells of many other organ systems, the heart, brain, nervous system, and ovaries etc., accounting for the extensive varied adverse side effects.
The next obvious question is, what can be done about all this ŝҏіке protein accumulating in the heart and other organs? What can we do to get rid of it? Unfortunately conventional medicine is of no help. Mainstream cardiologists simply throw up their hands and shrug their shoulders and have nothing useful to offer.
There is one eminent, highly published cardiologist who has offered a treatment protocol which, in my opinion, is highly effective for removing ŝҏіке protein. This is the Dr. Peter McCullough’s ŝҏіке protein detoxification protocol. This is the protocol Mike should have been taking from the beginning.
 Base Spike Detoxification Protocol from Dr Peter McCullough
Base Spike Detoxification Protocol from Dr Peter McCullough
Left Image: courtesy of McCullough, Peter A., Cade Wynn, and Brian C. Procter. “Clinical rationale for SARS-CoV-2 base spike protein detoxification in post COVID-19 and vaccine injury syndromes.” J Am Physicians Surg 28 (2023): 90-94.(1)
IN 2024, Dr Peter McCullough writes:
The spike protein is responsible for the pathogenicity of the SARS-CoV-2 infection and drives the development of adverse events, injuries, disabilities, and death after vaccination through immunologic and thrombotic mechanisms. The long-lasting spike protein has been found in the brain, heart, liver, kidneys, ovaries, testicles, and other vital organs at autopsy in cases of death after vaccination. In the case of vaccine-induced thrombotic injury, the spike protein has been found within the blood clot itself. Thus, there is strong rationale for considering residual SARS-CoV-2 spike protein as a treatment target in post COVID-19 and vaccine injury syndromes. The spike protein participates directly in pathophysiology, incites inflammation, and propels thrombosis. While specific syndromes (cardiovascular, neurological, endocrine, thrombotic, immunological) will require additional therapies, we propose the clinical rationale for a base detoxification regimen of oral nattokinase, bromelain, and curcumin for patients with post-acute sequalae from SARS-CoV-2 infection and COVID-19 vaccination. The empiric regimen can be continued for 3-12 months or more and be guided by clinical parameters:
– Nattokinase 2000 FU (100) mg orally twice a day without food
– Bromelain 500 mg orally once a day without food
– Curcumin 500 mg orally twice a day (nano, liposomal, or with piperine additive suggested)
No therapeutic claims can be made for this regimen because it has not been tested in large, prospective, double-blind, placebo controlled randomized trials. No such studies are planned or funded currently by federal or institutional sponsors. The main caveats are bleeding and allergic reactions. The regimen can be used in addition to anti-platelet and antithrombotic agents, however, caution is advised with respect to monitoring bleeding risks. (1)
How to Order Supplements On-Line
Nattokinase, Bromelain and Curcumin are nutritional supplements which can be purchased over the counter without a prescription. For your convenience, here are links to these products at my Pure Encapsulations Store for on-line ordering:
NSK-SD (Nattokinase) – each vegetable capsule contains: nattokinase (2000 FU) (soy) 100 mg
(Nattokinase) – each vegetable capsule contains: nattokinase (2000 FU) (soy) 100 mg
Nattokinase is a highly purified fibrinolytic enzyme that has demonstrated encouraging potential for supporting endogenous fibrinolytic activity and promoting healthy blood flow, circulation, and blood vessel function. Pure Encapsulations NSK- SD is standardized to contain a minimum of 20,000 FU (fibrinolytic units) per gram.
Bromelain 2400 Each vegetable capsule contains Bromelain (2,400 gdu/gram) 500 mg
Bromelain enhances digestion and maintains healthy musculoskeletal tissue. Bromelain is a proteolytic enzyme from the stem of the pineapple plant. Taken with food, bromelain aids in the healthy functioning of the digestive system. Taken between meals, bromelain maintains healthy kinin and fibrin production, supporting healthy musculoskeletal function. Bromelain 2400 nutritionally supports the body’s innate ability to digest food and to maintain musculoskeletal comfort at the cellular level.
Curcumin 500 with Bioperine® : each vegetable capsules contains:turmeric (Curcuma longa) extract (root)† (standardized to contain 95% curcuminoids) 500 mg. – Bioperine® (Piper nigrum) extract (fruit) †† 5.3 mg. Turmeric may be contra-indicated with blood thinning medications.
Curcumin 500 with Bioperine® provides powerful support for maintaining a healthy inflammatory response, promoting cellular health, and supporting healthy liver, colon and musculoskeletal function. Bioperine® is a black pepper extract that contains the alkaloid piperine. Research reveals that it has the potential to enhance the bioavailability of curcumin, promoting its absorption.
Empiric Therapy can be Pursued
In April 2024, Dr Frank Yap, M.D. discussed the lack of clinical trials for spike protein detoxification protocols. However Dr Frank Yap feels that empiric therapy can be pursued, writing:
Patients should push their doctors to refer them to clinical trials, and when that is not feasible, then empiric therapy can be pursued. It is important to realize that in the absence of completed large randomized placebo controlled randomized trials, which are easily 5 or more years away in the future, no therapeutic claims can be made. In the meantime we must be perceptive as patients and open-minded as clinicians to come up with reasonable approaches that can be used to help those sick now with post-COVID syndromes. (9)
Conclusion: Fibrinolytic and proteolytic enzymes have a long history of use in medicine. Spike protein detoxification is one of the more recent uses. Curcumin is a well known and popular anti-inflammatory supplement used for centuries. Thanks to Dr. Peter McCullough for making this spike protein detoxification protocol available for public use. Who should be taking this? Some doctors have suggested that everyone should be taking this protocol on a regular basis. This protocol is used on an empiric basis, as there are no validating long term medical studies as yet, and probably never will be.
Although nutritional supplements in this spike protein detoxification protocol are generally regarded as safe (GRAS), the reader is advised to consult and work closely with a knowledgeable physician before starting. (1-10)
The reader is advised to read this DISCLAIMER.
Jeffrey Dach MD
7450 Griffin Road Suite 180/190
Davie, Florida 33314
954-792-4663
====================================
Articles with related interest:
Fibrinolytic and Proteolytic Enzymes for Treatment of Various Conditions
References
ŝҏіке protein detoxification
1) McCullough, Peter A., Cade Wynn, and Brian C. Procter. “Clinical rationale for SARS-CoV-2 base spike protein detoxification in post COVID-19 and vaccine injury syndromes.” J Am Physicians Surg 28 (2023): 90-94.
2) Hulscher, Nicolas, et al. “Clinical approach to post-acute sequelae after COVID-19 infection and vaccination.” Cureus 15.11 (2023).
3) Kyriakopoulos, Anthony M., and Stephanie Seneff. “Proteolytic targets for SARS-CoV-2 spike protein degradation: Hope for systemic detoxification.” Journal of American Physicians and Surgeons 28.3 (2023): 86-93.
4) Halma, Matthew TJ, et al. “Strategies for the management of spike protein-related pathology.” Microorganisms 11.5 (2023): 1308.
5) Dhuli, K., et al. “Presence of viral spike protein and vaccinal spike protein in the blood serum of patients with long-COVID syndrome.” Eur Rev Med Pharmacol Sci 27.6 Suppl (2023): 13-19.
6) Craddock, Vaughn, et al. “Persistent circulation of soluble and extracellular vesicle‐linked Spike protein in individuals with postacute sequelae of COVID‐19.” Journal of Medical Virology 95.2 (2023): e28568.
7) Theoharides, Theoharis C. “Could SARS-CoV-2 spike protein be responsible for long-COVID syndrome?.” Molecular Neurobiology 59.3 (2022): 1850-1861.
======================================
8) Solving the covid challenge. Base Spike Detoxification Protocol by Dr. Peter McCullough
The spike protein is responsible for the pathogenicity of the SARS-CoV-2 infection and drives the development of adverse events, injuries, disabilities, and death after vaccination through immunologic and thrombotic mechanisms. The long-lasting spike protein has been found in the brain, heart, liver, kidneys, ovaries, testicles, and other vital organs at autopsy in cases of death after vaccination. In the case of vaccine-induced thrombotic injury, the spike protein has been found within the blood clot itself. Thus, there is strong rationale for considering residual SARS-CoV-2 spike protein as a treatment target in post COVID-19 and vaccine injury syndromes. The spike protein participates directly in pathophysiology, incites inflammation, and propels thrombosis. While specific syndromes (cardiovascular, neurological, endocrine, thrombotic, immunological) will require additional therapies, we propose the clinical rationale for a base detoxification regimen of oral nattokinase, bromelain, and curcumin for patients with post-acute sequalae from SARS-CoV-2 infection and COVID-19 vaccination.
The empiric regimen can be continued for 3-12 months or more and be guided by clinical parameters:
– Nattokinase 2000 FU (100) mg orally twice a day without food
– Bromelain 500 mg orally once a day without food
– Curcumin 500 mg orally twice a day (nano, liposomal, or with piperine additive suggested)
9) Dr Peter McCullough: How to Detox Spike Protein from Body
By Dr Frank Yap, M.D. – April 23, 2024
According to Dr Peter McCullough (in a Twitter post – July 2023):
Base Spike Detox is what I am currently using in my practice for those who have had COVID-19 multiple times, one or more of the COVID-19 vaccines, or both and believe persistent SARS-CoV-2 Spike protein could be causing problems in their body. A major publication is under review and editing; however, the information is far too important to hold back.
Update (Nov 2023): Published on August 25, 2023 in Journal of American Physicians and Surgeons. CLICK HERE FOR THE COMPLETE PAPER > Base Spike Protein Detoxification and on November 21, 2023 in Cureus (PubMed – November 2023)
I have arrived, based on the emerging scientific literature and my clinical observation, that three OTC products are essential as a triple base combination:
Nattokinase 2000 FU (100 mg) twice a day
Bromelain 500 mg once a day
Nano/Liposomal Curcumin 500 mg twice a day
Additional products can be added, including NAC, IVM (Ivermectin), HCQ (Hydroxychloroquine), fluvoxamine, low-dose naltrexone, and blood thinners, depending on the clinical evaluation and the syndrome. The therapeutic objective is to start treatment and allow the body to clear Spike and its fragments with the natural reticuloendothelial system. I believe this triple combination is the best approach.
Patients can get a big head start if they self-initiate Base Spike Detox as they get organized for appointments. I have found three months is a minimum duration, and some require more than a year. Don’t expect instant results, be patient. I have a major manuscript under review for publication that summarizes the clinical rationale and evidence supporting Base Spike Detox.
Important safety warnings include bleeding for those on blood thinners or who have bleeding disorders (e.g., hemophilia), soy allergy, allergies to any component of the combination, and gastrointestinal intolerance. Women of childbearing potential without contraception, pregnant, breastfeeding, and children should not take this combination unless directed by a doctor.
COVID-19 Vaccine Myocarditis Research Wins Award
We’re thrilled to announce that Dr Peter McCullough, won first place on Preprints.org for a study he co-authored on vaccine-induced myocarditis.
Preprints.org is a vital platform for the early dissemination of scholarly research before standard peer review and publication in scientific journals. By allowing research findings to be shared early with the scientific community, Preprints.org facilitates scientific communication and collaboration, enabling researchers to receive feedback and engage with the broader scientific community.
Autopsy Proven Fatal COVID-19 Vaccine-Induced Myocarditis claimed the top spot in the Medicine and Pharmacology category, specifically focusing on cardiac and cardiovascular systems. This research paper delves into a critical issue surrounding COVID-19 vaccination — the potential risk of myocarditis, particularly in cases where it leads to fatal outcomes.
Nattokinase and Spike Protein
Tanikawa et al. examined the effect of nattokinase on the spike protein of SARS-CoV-2. In the first experiment, they demonstrated that spike was degraded in a time and dose-dependent manner in a cell lysate preparation that could be analogous to a vaccine recipient. The second experiment demonstrated that nattokinase degraded the spike protein in SARS-CoV-2 infected cells. This was reproduced in a similar study done by Oba and colleagues in 2021.
Tanikawa T, Kiba Y, Yu J, Hsu K, Chen S, Ishii A, Yokogawa T, Suzuki R, Inoue Y, Kitamura M. Degradative Effect of Nattokinase on Spike Protein of SARS-CoV-2. Molecules. 2022 Aug 24;27(17):5405.
Nattokinase is dosed in fibrinolytic units (FU) per gram and can vary according to purity. Kurosawa and colleagues have shown in humans that after a single oral dose of 2000 FU D-dimer concentrations at six, and eight hours, and blood fibrin/fibrinogen degradation products at four hours after administration elevated significantly (p
Thus an empiric starting dose could be 2000 FU twice a day. Full pharmacokinetic and pharmacodynamic studies have not been completed, but several years of market use as an over-the-counter supplement suggests nattokinase is safe with the main caveat being excessive bleeding and cautions with concurrent antiplatelet and anticoagulant drugs.
Editor’s Note: We are aware of a fact-check article by AFP titled “Experts rubbish Covid vaccine ‘detoxification’ supplement”. In my humble opinion, the title may come across as excessively confident and strongly worded.
The article makes a claim that ‘There is no evidence that nattokinase dissolves the spike protein of SARS-CoV-2 in the human body,’ while also citing evidence from the Tanikawa study. It’s important to acknowledge that the Tanikawa study is a small lab study, which is a common starting point in the research process before moving on to larger studies.
Nevertheless, we agree that nattokinase is not a miracle drug, and further research is necessary. It’s worth noting that there are more than 200 studies related to nattokinase published on PubMed.
Moreover, it’s essential to recognize that there are multiple approaches to managing COVID-19. We encourage you to consult with your trusted healthcare provider to thoroughly discuss and assess the potential benefits and risks of various possible treatments.
Ivermectin and Spike Protein
Former NIH researcher David Scheim, PhD, early in the pandemic proposed that SARS-CoV-2 Spike protein was acting like a grappling hook pulling together circulating red blood cells (RBCs) into long chains and clumps in a process called hemagglutination (HA).
This explained why the red blood cells could not carry oxygen normally and was congruent with the finding of micro blood clots in the lungs. Boschi et al have provided additional support for this mechanism (source). By reversing the clumping of red blood cells, ivermectin enabled the patient’s proper respiratory function to return.
According to the authors:
“Ivermectin blocked HemAgglutination when added to RBCs prior to spike protein and reversed HA when added afterwards.”
In another spectacular publication, Stone et al, describes the prompt improvement of oxygenation in patients with ivermectin (source).
The published oxygenation curves from multiple studies clearly show this physiological effect of ivermectin occurs so rapidly, it must be explained by a direct anti-Spike protein effect of ivermectin. An anonymous video of a critically ill man demonstrates the very effect that Scheim, Stone, Hazan, and Babalola have described in the Figure above. So for the next critically ill patient with COVID-19, if the opportunity presents itself, push for the administration of ivermectin. This is the only published therapy for COVID-19 that improves oxygen saturation while the patient mounts a recovery. As in this man, it may be the critical factor for a turnaround and a chance to walk out of the hospital.
Key Takeaway
Patients should push their doctors to refer them to clinical trials, and when that is not feasible, then empiric therapy can be pursued. It is important to realize that in the absence of completed large randomized placebo controlled randomized trials, which are easily 5 or more years away in the future, no therapeutic claims can be made. In the meantime we must be perceptive as patients and open-minded as clinicians to come up with reasonable approaches that can be used to help those sick now with post-COVID syndromes.
References:
10) Halma, M.T.J.; Plothe, C.; Marik, P.; Lawrie, T.A. Strategies for the Management of Spike Protein-Related Pathology. Microorganisms 2023, 11, 1308. https://doi.org/10.3390/microorganism...
11) Tanikawa T, Kiba Y, Yu J, Hsu K, Chen S, Ishii A, Yokogawa T, Suzuki R, Inoue Y, Kitamura M. Degradative Effect of Nattokinase on Spike Protein of SARS-CoV-2. Molecules. 2022 Aug 24;27(17):5405. doi: 10.3390/molecules27175405. PMID: 36080170; PMCID: PMC9458005.
62% Normalization in SpO2 within 24 Hours for severe COVID-19 patients after Ivermectin-Based Combination Treatment.
Peter A. McCullough’s Substack.
Editor’s Note:
Why should you trust this article? While we don’t ask for blind trust, we do encourage you to trust in your own judgment. Our primary goal is to empower you to conduct thorough research and make informed healthcare decisions in consultation with your trusted medical doctor.
Though there are many spike protein detox treatment protocols out there, we consider and recommend the I-Recover protocol as one of the best.
Given the lack of clinical trials of long-haul COVID-19 syndrome, these recommendations are based on the abnormal changes within the body associated with the COVID-19 disease and post viral illnesses along with the collective experience of FLCCC members.
This protocol has also been used to treat post-vaccine inflammatory syndromes with similar success. As with all FLCCC Alliance protocols, the components, doses, and durations will evolve as more clinical data accumulates.
Due to the marked overlap between long COVID and post-vaccine syndrome, please refer to the I-RECOVER Post-Vaccine Treatment protocol for detailed treatment strategies.
This base spike protein detox protocol consists of these three powerful ingredients: Spike Support’s Nattokinase, Bromelain, and Tumeric Extract.
Vaccinated or not, prioritizing your well-being has never been more crucial.
Buy this ultimate detox bundle today, researched by Dr. Peter McCullough.
Recommended to maintain daily health for anyone exposed to COVID, vaccines, or shedding – and may help your body repair itself and remain at optimal health.
Where to buy Base Spike Detox Trio Formula: Available on The Wellness Company’s website. Here is the link: Base Spike Detox Trio
===================================================
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Copyright (c) 2024 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on April 28th, 2024 by Jeffrey Dach MD
The post Spike Protein Detoxification Protocol of Dr Peter McCullough appeared first on Jeffrey Dach MD.
April 9, 2024
Errors in Modern Medicine: The Fear of Estrogen

Errors in Modern Medicine: The Fear of Estrogen
Rebecca is a 52 year old post menopausal school teacher sitting in my office crying because she knows she needs menopausal hormone replacement if she wants to remain healthy, and yet her primary care doctor and OB/Gyne doctor have both told her estrogen is dangerous, causes breast cancer. Both doctors refused to prescribe hormone replacement for her. In addition, Rebecca’s two closest friends have advised her against it, citing a family member currently diagnosed with breast cancer undergoing chemotherapy. Clearly, Rebecca is torn between two opposing viewpoints, creating mental tension and despair (see left image). This is a recurring scenario all across the country. As is my usual practice, I explained to Rebecca there is no need to make a decision right now, there is plenty of time to study the issue. I even pointed her to reading material on my blogs, my newsletters, and book discussing the safety and efficacy of menopausal hormone replacement. I then told Rebecca that if she gains a greater understanding and feels more comfortable in the future, I would be glad to get her started on the hormone replacement program. There is no pressure, and I respect whatever decision she feels comfortable with. Finally, Rebecca agreed with the plan and left the office in good spirits. This is a recurring scenario in my office, duplicated in countless doctor’s offices across the country.
Left upper image: The Scream by Annemarie Busschers, painting, 250 x 160 cm 2010 private collection Miami, courtesy of Wikimedia Commons.
Errors in Modern Medicine
One of the most glaring errors in conventional medicine is the false idea that Estrogen is somehow bad, and causes breast cancer, blood clots, other adverse effects. Modern medicine falsely says that Estrogen should never be prescribed for the post-menopausal female, and especially never to breast cancer survivors. The resulting mass media propaganda campaign creates fear of estrogen throughout the population. Nothing could be farther from the truth. The reality is Menopausal Hormone Replacement with Estrogen is safe and effective. Not only does Estrogen not cause breast cancer, it is actually preventive of breast cancer. I will show you the studies why this is true. When applied via the transdermal route with topical creams, estrogen does not cause blood clots. That is why we use transdermal creams and avoid oral estrogen tablets (which are associated with blood clots, increased coagulation, deep venous thrombosis and pulmonary embolus).
Premarin-Alone (Estrogen) Users Have 23 percent less Breast Cancer Than Placebo
The second arm of the WHI study included 10,739 post-menopausal women after hysterectomy randomized to Estrogen (Premarin, CEE) or to placebo. In 2004, the data from the second arm of the Women’s Health Initiative (WHI) was published in JAMA 2004. This data included 6.8 years of follow up showing 23% less invasive breast cancer in the Premarin treated group (also called CEE) compared to placebo group. There were 94 breast cancer cases in the estrogen hormone group (CEE) and 124 cases of breast cancer in the placebo group.
Estrogen Group Second Arm of WHI: 45% Reduction in Mortality from Breast Cancer
The 18 year follow up showed a 45 percent reduction in mortality from breast cancer in the estrogen treated group compared to placebo. In 2017, Dr. JoAnn Manson reviewed the 18 year follow up of the Second Arm of the WHI (Premarin-Alone) showing a 45 percent reduction in breast cancer mortality in the Estrogen User Group !! Dr. Manson writes:
After 18 years of cumulative follow-up of the WHI-CEE cohort, breast cancer mortality was statistically significantly reduced by 45% (HR, 0.55; 95% CI, 0.33–0.92). This may well be the most significant and most over-looked finding of the WHI-CEE trial (1).
Breast Cancer Mortality in Both Arms of WHI
Here is the Data on the cumulative 18-year follow-up of 2 randomized clinical trials WHI First and Secoond Arms, between 1993 and 1998 and followed up through December 31, 2014
First Arm CEE plus MPA vs Placebo active=61/ Placebo=40 HR=1.44
Second Arm CEE alone vs Placebo active=22 /Placebo 41 HR 0.55
Premarin Plus Medroxyprogesterone – First Arm of the Women’s Health Initiative 26 percent greater Breast cancer in Hormone Users
Remember there are two arms of the WHI. We discussed the second arm from 2004 above. Now, we will go back two years to 2002 and discuss the first Arm.
In 2002, the first Arm of the Women’s Health Initiative (WHI) was published in JAMA, halted early after 5.2 years because of increased breast cancer in the estrogen treated group. This study created havoc in medical practice and in the general population. Fear of estrogen made women stop requesting and doctors stop prescribing Hormone Replacement Therapy (HRT). Following this 2002 publication in JAMA, the entire previous medical edifice of menopausal hormone replacement was dismantled. Training programs disappeared. New doctors no longer had training or expertise to even practice hormone replacement.
The first arm of the WHI randomized 16,608 post-menopausal women to either Prempro (Premarin plus Medroxyprogesterone) or placebo. After 5.2 years of follow up, there were 290 cases of breast cancer in the Prempro group which is 26% greater than the placebo group. The authors write:
Estimated hazard ratios (HRs) (nominal 95% confidence intervals [CIs]) were as follows: CHD, 1.29 (1.02-1.63) with 286 cases; breast cancer, 1.26 (1.00-1.59) with 290 cases; stroke, 1.41 (1.07-1.85) with 212 cases; PE, 2.13 (1.39-3.25) with 101 cases; colorectal cancer, 0.63 (0.43-0.92) with 112 cases; endometrial cancer, 0.83 (0.47-1.47) with 47 cases; hip fracture, 0.66 (0.45-0.98) with 106 cases; and death due to other causes, 0.92 (0.74-1.14) with 331 cases.
The synthetic progestin, Medroxyprogesterone (MPA), is a known breast cancer carcinogen, and commonly used to induce breast cancer in animal models.
Lanari, Claudia, et al. “The MPA mouse breast cancer model: evidence for a role of progesterone receptors in breast cancer.” Endocrine-related cancer 16.2 (2009): 333.
Re-Analysis of First Arm WHI Data Shows Glaring Error
In 2018, Dr. Howard Hodis and Phillip Sarrel re-analyzed the data from the WHI first and second arms. They found an error in the study. Some of the women in the placebo group had a history of prior HRT use. These women should have been removed from the placebo group, and were not. The prior use of estrogen confers protection from breast cancer, and falsely reduces the incidence of breast cancer in the placebo group. If the women with prior HRT use are removed from the placebo group, the data chart (see Figure 1 below) looks entirely different. There is a null effect, meaning no difference between the Prempro group and the Placebo group in terms of breast cancer incidence. Dr. Howard Hodis writes:
In fact, the increased HR [Hazard Ratio] was not due to an increased breast cancer incidence rate in women randomized to CEE + MPA [Prempro] therapy but rather due to a decreased and unexpectedly low breast cancer rate in the subgroup of women with prior HT [Hormone Therapy] use randomized to placebo. For women who were HT naïve when randomized to the WHI, the breast cancer incidence rate was not affected by CEE + MPA therapy relative to placebo for up to 11 years of follow-up…the data clearly show that CEE+MPA therapy had a null effect on breast cancer risk particularly in the subgroup of women representing the typical population of women treated with HT who are HT naïve before receiving menopausal HT…it is clear that breast outcome data from the WHI-CEE+MPA trial has been misinterpreted and overgeneralized. (2)
SEE Below FIG. 1: There are two different placebo groups. Left Chart shows placebo group with no prior hormone use. Notice Invasive breast cancer trend lines are superimposed. Right Chart shows placebo group with prior hormone use: Notice divergence in trend lines for breast cancer (Red Arrows). This divergence accounts for the false impression of increased cancer risk in the Prempro (Premarin +MPA) Group. This shows that prior hormone use is breast cancer protective! (2)

Above image Fig. 1 Courtesy of Hodis, Howard 2018: It is the divergence (Red Arrow- Right Chart) in the trend line for women with prior hormone therapy use randomized to placebo that accounts for the elevated hazard ratio for breast cancer falsely giving the impression that breast cancer incidence was increased in the trial due to conjugated equine estrogen plus medroxyprogesterone acetate where in fact the elevated hazard ratio was due to a DECREASED breast cancer incidence In the PLACEBO treated group. (2)
Dr. Rowan Chlebowski, December 2019
In 2019, Dr. Rowan Chlebowski reviewed the re-analysis of the data stating that estrogen alone reduces breast cancer, while estrogen plus medroxyprogresgerone has the opposite effect, writing:
Estrogen alone decreased, while adding progestin increased, breast cancer incidence…CEE-alone [Premarin-Alone] and CEE plus MPA [Medroxyprogesterone] use have opposite effects on breast cancer incidence. CEE alone significantly decreases breast cancer incidence which is long term and persists over a decade after discontinuing use. CEE plus MPA use significantly increases breast cancer incidence which is long term and persists over a decade after discontinuing use. (3)
Dr. Lindsay Berkson: Nothing Else Like Estrogen Therapies Has Ever Been Shown to Be So Breast Protective.
On October 2023, Dr Lindsay Berkson discussed this issue on her substack blog, writing:
The WHI 1 authors forgot to ask, and thus did not remove, in the placebo group, any women who had already taken estrogen therapies…Since estrogen was ultimately, on re-analysis found to be “breast protective” , and the synthetic progestins were huge adverse contributing issues, this made the incidence of breast cancer in the placebo group of ladies, lower, as women had already taken the protective estrogen…This made the experimental arm, women taking hormones, falsely appear as though they had more cases of breast cancer…When the data was re-analyzed, thus “righted” by taking out this “confounding issue”, and longer term effects of estrogen looked at with a fine tooth comb, the same original authors, re-published their re-analysis. This is now what I call the WHI 2…Conclusions of WHI 2: Women taking estrogen replacement therapy (ERT) had 23% less incidence or chance of getting breast cancer in the first place. And if you had been on ERT, and got breast cancer, you had a 44% decreased chance of dying from it. Progestins were more the breast damaging issue. Not estrogen. So, stunning as it is, being on ERT put you in a better position, even if you went on to get breast cancer! This is something that is now replicated. Substantiated. But not taught in most med schools or appreciated by most docs and women. Or lawyers!…Estrogen “protects” healthy breast tissue from getting breast cancer in the first place. And, if a women has been on estrogen therapies for an average of 5 years and then gets breast cancer, the estrogen therapies “reduce” her risk of dying from breast cancer by 44%. Nothing else like estrogen therapies has ever been shown to be so breast protective. (4)
Our Breast Cancer Prevention Program
Use human bioidentical progesterone, avoiding the carcinogenic synthetic progestins such as medroxyprogesterone and norethindrone (see below chart) .Include Estriol (E3) which is breast cancer protective.Include Progesterone which prevents endometrial hyperplasia, prevents endometrial cancer, and prevents breast cancer.Iodine supplementation – decreases breast cancer risk and useful in treatment of breast cancer. (Iodine Treats Breast Cancer)Testosterone- decreases breast cancer risk by 40 per cent. (See: Testosterone for Prevention and Treatment of Breast Cancer)DIM (Di-Indole-Methane) diverts estrogen metabolism toward favorable metabolic pathways.Selenium- low selenium increases cancer risk.Vitamin D3 – low D3 increases cancer risk.Methyl-Folate – methylation defects increase cancer riskWe do not perform screening mammography on the healthy population because screening mammography has been shown to have no effect on breast cancer mortality in national data. (see: Laura Esserman Questions Screening Mammography)Listing of progesterone and synthetic progestins. Progesterone is protective, all other synthetic progestins are carcinogenic:

Above chart courtesy of Siddique, Y. H., and M. Afzal. “A review on the genotoxic effects of some synthetic progestins.” Int J Pharmacol 4.6 (2008): 410-30. (5)
Conclusion: Thanks and credit goes to Dr. Lindsay Berkson for bringing to my attention the above re-analysis of the WHI by Dr. Hodis, who points out the placebo group included women with prior hormone use which confers protection from breast cancer and gives the false impression of increased breast cancer risk in the Premarin+ MPA group compared to placebo. When prior hormone use is removed from the placebo group, trend lines for breast cancer are superimposed for both groups (left chart Fig.1)
Articles with Related Interest
All Bioidentical Hormone Articles by Jeffrey Dach MD
Jeffrey Dach MD
7450 Griffin Road Suite 180/190
Davie, Fl 33314
954-792-4663
=======================================
References:
1) Manson, JoAnn E., et al. “Menopausal hormone therapy and long-term all-cause and cause-specific mortality: the Women’s Health Initiative randomized trials.” Jama 318.10 (2017): 927-938.
2) Hodis, Howard N., and P. M. Sarrel. “Menopausal hormone therapy and breast cancer: what is the evidence from randomized trials?.” Climacteric 21.6 (2018): 521-528.
3) Long-term Follow-up Shows Estrogen Alone and Estrogen Plus Progestin Have Opposite Effects on Breast Cancer Incidence in Postmenopausal Women by Rowan Chlebowski, Dec. 13, 2019
4) Substack article by Dr. Lindsay Berkson on Estrogen Hormone Replacement for Menopausal Women, a rebuttal to Mercola. Dr lindsay devaki berkson Oct 24, 2023
estrogen “protects” healthy breast tissue from getting breast cancer in the first place. And, if a women has been on estrogen therapies for an average of 5 years and then gets breast cancer, the estrogen therapies “reduce” her risk of dying from breast cancer by 44%. Nothing else like estrogen therapies has ever been shown to be so breast protective.
5) Siddique, Y. H., and M. Afzal. “A review on the genotoxic effects of some synthetic progestins.” Int J Pharmacol 4.6 (2008): 410-30.
6) The Anticancer Testosterone Metabolite 3β-Adiol. Published in: Townsend Letter By. Dr. Jonathan V. Wright, MD The bad side is that too much 16-OHE1 increases breast and prostate cancer risk.11-14 But like DHT, which also increases cancer risk, 16a-OHE1 s transformed into the anticarcinogenic
7) Warner, Margaret, et al. “25 years of ERβ: a personal journey.” Journal of Molecular Endocrinology 68.1 (2022): R1-R9.
8) Rymbai, Emdormi, et al. “Role of estrogen receptors in cancer: a special emphasis on the therapeutic potential of estrogen receptor ß.” Pharmaceutical Sciences Asia 49.5 (2022).
9) Wu, Wan-fu, et al. “Estrogen receptor β and treatment with a phytoestrogen are associated with inhibition of nuclear translocation of EGFR in the prostate.” Proceedings of the National Academy of Sciences 118.13 (2021): e2011269118.
10) Chimento, Adele, et al. “Estrogen receptors-mediated apoptosis in hormone-dependent cancers.” International journal of molecular sciences 23.3 (2022): 1242.
11) free pdf
Vasconsuelo, Andrea, et al. “Role of 17β-estradiol and testosterone in apoptosis.” Steroids 76.12 (2011): 1223-1231.
17b-Estradiol (E2) and Testosterone (T) exert actions in most animal tissues, in addition to the reproductive system. Thus, both sex steroid hormones affect growth and different cell functions in several organs. Accordingly, the nuclear estrogen (ER) and androgen (AR) receptors are ubiquitously expressed. Moreover, ER and AR may have non-classical intracellular localizations, e.g. plasma membrane, mitochondria and endoplasmic reticulum, raising additional complexity to the functional roles of E2 and T. In addition to the modulation of gene transcription by direct interaction with their cognate nuclear receptors, the steroids can rapidly activate signaling pathways by a non-genomic mechanism mediated by receptors identical to or different from known steroid receptors. Among various functions, E2 and T can regulate apoptosis through those pathways. In mitochondria, the presence of ER and AR and actions of estrogen and androgen have been shown, in keeping with the organelle being a control point of apoptosis. The most recurrent action for each steroid hormone is the protection of mitochondria against different insults, resulting in antiapoptosis. This review summarizes the molecular basis of the modulation of programmed cell death by E2 and T in several tissues.
12) https://www.sciencedirect.com/science...
Vasconsuelo, Andrea, et al. “Role of 17β-estradiol and testosterone in apoptosis.” Steroids 76.12 (2011): 1223-1231.
However, under some specific conditions E2 could trigger apoptosis in breast cancer cells, opposed to its well studied antiapoptotic role. This peculiar hormone behavior has
been observed in cells from breast cancer which have been longterm estrogen-deprived (LTED) or treated exhaustively with antiestrogens [87]. Curiously, the paradoxical induction of apoptosis by estrogen has been established under several unusual circumstances.
For example, in this case, the pre-conditions of prolonged estrogen depletion or exhaustive treatment with anti-estrogens of the breast cancer cells are mandatory requisites to trigger apoptosis by E2 and could explain the dual action of the steroid to stimulate growth or apoptosis. Thus, the development of antihormone resistance over years of therapy, reprograms the survival mechanism of the breast cancer cell so that estrogen no longer
functions as a survival factor but as a death signal.
13) https://www.ncbi.nlm.nih.gov/pmc/arti...
Rizza, Pietro, et al. “Estrogen receptor beta as a novel target of androgen receptor action in breast cancer cell lines.” Breast cancer research 16 (2014): 1-13.
The two isoforms of estrogen receptor (ER) alpha and beta play opposite roles in regulating proliferation and differentiation of breast cancers, with ER-alpha mediating mitogenic effects and ER-beta acting as a tumor suppressor. Emerging data have reported that androgen receptor (AR) activation inhibits ER-positive breast cancer progression mainly by antagonizing ER-alpha signaling. However, to date no studies have specifically evaluated a potential involvement of ER-beta in the inhibitory effects of androgens.
Collectively, these data provide evidence for a novel mechanism by which activated AR, through an up-regulation of ER-beta gene expression, inhibits breast cancer cell growth.
14) Pietri, Elisabetta, et al. “Androgen receptor signaling pathways as a target for breast cancer treatment.” Endocrine-related cancer 23.10 (2016): R485-R498.
15) https://pubmed.ncbi.nlm.nih.gov/33462...
Hickey, Theresa E., et al. “The androgen receptor is a tumor suppressor in estrogen receptor–positive breast cancer.” Nature medicine 27.2 (2021): 310-320.
Notably, AR agonists combined with standard-of-care agents enhanced therapeutic responses. Mechanistically, agonist activation of AR altered the genomic distribution of ER and essential co-activators (p300, SRC-3), resulting in repression of ER-regulated cell cycle genes and upregulation of AR target genes, including known tumor suppressors. A gene signature of AR activity positively predicted disease survival in multiple clinical ER-positive breast cancer cohorts. These findings provide unambiguous evidence that AR has a tumor suppressor role in ER-positive breast cancer and support AR agonism as the optimal AR-directed treatment strategy, revealing a rational therapeutic opportunity.
16) https://www.ncbi.nlm.nih.gov/pmc/arti...
You, Chan-Ping, et al. “Modulating the activity of androgen receptor for treating breast cancer.” International Journal of Molecular Sciences 23.23 (2022): 15342.
17) Traphagen, Nicole A., et al. “High estrogen receptor alpha activation confers resistance to estrogen deprivation and is required for therapeutic response to estrogen in breast cancer.” Oncogene 40.19 (2021): 3408-3421.
======================================
18) https://www.sabcs.org/sabcs/2019/pres...
presented at the yearly SA TX Breast Cancer Symposium see below including authors at 2019 SABCS.
Long-term Follow-up Shows Estrogen Alone and Estrogen Plus Progestin Have Opposite Effects on Breast Cancer Incidence in Postmenopausal Women by Rowan Chlebowski, Dec. 13, 2019
Estrogen alone decreased, while adding progestin increased, breast cancer incidence
SAN
CEE-alone and CEE plus MPA use have opposite effects on breast cancer incidence. CEE alone significantly decreases breast cancer incidence which is long term and persists over a decade after discontinuing use. CEE plus MPA use significantly increases breast cancer incidence which is long term and persists over a decade after discontinuing use. As a result of the attenuation of subgroup interactions: all postmenopausal women with prior hysterectomy using CEE-alone have the potential benefit of experiencing a reduction in breast cancer incidence while all postmenopausal women using CEE plus MPA have the potential risk of experiencing an increase in breast cancer incidence.
——————
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! BEST !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
19 https://www.ncbi.nlm.nih.gov/pmc/arti...
Hodis, Howard N., and P. M. Sarrel. “Menopausal hormone therapy and breast cancer: what is the evidence from randomized trials?.” Climacteric 21.6 (2018): 521-528.
The relationship between menopausal hormone therapy (HT) and breast cancer is complex and further complicated by misinformation, perception, and overgeneralization of data. These issues are addressed in this mini-review through the lens of the Women’s Health Initiative (WHI) that has colored the view of HT and breast cancer. In the WHI, unopposed conjugated equine estrogen (CEE) reduced breast cancer risk and mortality. In the WHI CEE plus continuously combined medroxyprogesterone acetate (MPA) trial, although the hazard ratio (HR) was elevated it was statistically non-significant for an association between CEE + MPA and breast cancer. In fact, the increased HR was not due to an increased breast cancer incidence rate in women randomized to CEE + MPA therapy but rather due to a decreased and unexpectedly low breast cancer rate in the subgroup of women with prior HT use randomized to placebo. For women who were HT naïve when randomized to the WHI, the breast cancer incidence rate was not affected by CEE + MPA therapy relative to placebo for up to 11 years of follow-up. The current state of science indicates that HT may or may not cause breast cancer but the totality of data neither establish nor refute this possibility. Further, any association that may exist between HT and breast cancer appears to be rare and no greater than other medications commonly used in clinical medicine.
any conclusions that HT causes breast cancer has eluded definitive proof for over 5 decades, including WHI.
However, the data clearly show that CEE+MPA therapy had a null effect on breast cancer risk particularly in the subgroup of women representing the typical population of women treated with HT who are HT naïve before receiving menopausal HT.
SEE FIGURE 1 !!!!!!!!!!!!!!!!!!!!!
Although the cause of this outlier low incidence rate of breast cancer in the placebo group of women who had prior HT use is unknown, it is stunning that this unappreciated fact has escaped a more conspicuous and transparent discussion of the important impact that this finding has on interpretation of the breast cancer results from the WHI-CEE+MPA trial.
it is clear that breast outcome data from the WHI-CEE+MPA trial has been misinterpreted and overgeneralized
That is, the WHI-CEE+MPA trial strongly refutes the possibility that CEE+MPA therapy increased the risk of breast cancer in this trial.
50 years of study has failed to conclusively prove cause-and-effect between HT and breast cancer with the preponderance of evidence supporting benefits over risks with amelioration of downstream morbidity and mortality.
!!!!!!!!!!!!!!!!!! ???????? !!!!!!!!
After 18 years of cumulative follow-up of the WHI-CEE cohort, breast cancer mortality was statistically significantly reduced by 45% (HR, 0.55; 95% CI, 0.33–0.92). This may well be the most significant and most over-looked finding of the WHI-CEE trial (7).
20) https://www.ncbi.nlm.nih.gov/pmc/arti...
Manson, JoAnn E., et al. “Menopausal hormone therapy and long-term all-cause and cause-specific mortality: the Women’s Health Initiative randomized trials.” Jama 318.10 (2017): 927-938.
cumulative 18-year follow-up,
2 randomized clinical trials between 1993 and 1998 and followed up through December 31,2014
Breast Cancer Mortality
CEE plus MPA vs Placebo active=61/ Placebo=40 HR=1.44
CEE alone vs Placebo
active=22 /Placebo 41 HR 0.55
cumulative 18-year follow-up of WHI
———————————–
Dr. Lindsay Berkson:
The WHI 1 authors forgot to ask, and thus did not remove, in the placebo group, any women who had already taken estrogen therapies.
Since estrogen was ultimately, on re-analysis found to be “breast protective” , and the synthetic progestins were huge adverse contributing issues, this made the incidence of breast cancer in the placebo group of ladies, lower, as women had already taken the protective estrogen.
This made the experimental arm, women taking hormones, falsely appear as though they had more cases of breast cancer.
When the data was re-analyzed, thus “righted” by taking out this “confounding issue”, and longer term effects of estrogen looked at with a fine tooth comb, the same original authors, re-published their re-analysis. This is now what I call the WHI 2.
Conclusions of WHI 2:
Women taking estrogen replacement therapy (ERT) had 23% less incidence or chance of getting breast cancer in the first place.
And if you had been on ERT, and got breast cancer, you had a 44% decreased chance of dying from it.
Progestins were more the breast damaging issue. Not estrogen.
So, stunning as it is, being on ERT put you in a better position, even if you went on to get breast cancer! This is something that is now replicated. Substantiated. But not taught in most med schools or appreciated by most docs and women. Or lawyers!
21) https://www.medrxiv.org/content/10.11...
Baik, Seo H., Fitsum Baye, and Clement J. McDonald. “Effects of Hormone Therapy on survival, cancer, cardiovascular and dementia risks in 7 million menopausal women over age 65: a retrospective observational study.” medRxiv (2022): 2022-05.
The 7 million menopause study
The 7 million NIH study, the largest study ever run on women, with 1.5 million American women on ERT, shows that women 65 and older on estrogen therapies have statistically “less” of all 5 cancers studied (breast, ovarian, uterine, lung and colon). As well as live almost 20% longer, healthier lives. With less heart disease (unless on oral estrogens) and less dementias.
The Arizona insurance study showed that women (almost 400,000) taking natural steroids had 79% less dementias (Association between menopausal hormone therapy and risk of neurodegenerative diseases: Implications for precision hormone therapy. Alzheimers Dement (N Y). 2021 May 13;7(1):e12174.).
22) https://pubmed.ncbi.nlm.nih.gov/34027...
Kim, Yu Jin, et al. “Association between menopausal hormone therapy and risk of neurodegenerative diseases: Implications for precision hormone therapy.” Alzheimer’s & Dementia: Translational Research & Clinical Interventions 7.1 (2021): e12174.
23) Evaluating Estrogen Detoxification to Understand Breast Cancer Risk
by Debbie Rice, ND, MPH
The most dangerous estrogen metabolite is the 4-OH-E1 metabolite.The 4-OH-E1 metabolite has the potential to become a reactive quinone that causes DNA damage. Thus, if the body is not able to neutralize the 4-OH metabolites well or efficiently, they can wreak havoc on DNA. When DNA is damaged, it disrupts cellular signaling and the body’s ability to repair itself and stop abnormal cell growth. There is correlation between increased 4-OH-E1 metabolites and breast cancer risk. Miao, et al state: “Among many alterations of sex hormone metabolisms, 4-hydroxy estrogen (4-OH-E) metabolite was found to be significantly increased in the urine samples of patients with breast cancer compared with the normal healthy controls. This was the most important risk factor for breast cancer”.
24) Does Estrogen Cause Breast Cancer ? The Answer is –
NO – Estrogen Does NOT Cause Breast Cancer by Jeffrey Dach MD
The results of the 11 year follow up of the Women’s Health Initiative was covered in my previous article.(1) Rather than causing breast cancer, estrogen prevented it. This study found a significant reduction in breast cancer rates for Post-Menopausal women using Estrogen Replacement (Premarin Only Arm)(To be exact, there was a 23% reduction in breast cancer in Premarin Users compared to placebo.)(1)
Rebuttal to Mercola’s Article on Hormone Therapy Lindsey Berkson, DC
Women taking estrogen replacement therapy (ERT) had 23% “less” incidence or chance of getting breast cancer in the first place.
And if you had been on ERT and got breast cancer, you had a “44%” decreased chance of dying from it.
Progestins were the more breast-damaging issue. Not estrogen.
https://price-pottenger.org/journal_a...
The True Power of Hormones: An Interview with Devaki Lindsey Berkson, DC by Steven Schindler / October 13, 2023
Price-Pottenger’s former executive director, Steven Schindler, on the important role of hormones in helping us achieve our highest possible levels of health and vitality.
https://drannacabeca.com/blogs/show/h...
Podcast with Dr Anna Cabeca and Dr. Lindsay Berkson discussing the myths surrounding Estrogen and HRT for women.
The Girlfriend Doctor w/ Dr. Anna Cabeca
Hormones and Breast Cancer with Dr. Devaki Lindsey Berkson
Dr. Anna Cabeca, the girlfriend doctor podcast. Importance of hippocampus volume
20 years after the WHI Trial.
Dr Lindsay Berkson Austin Texas
1977 Rotation in integrative medicine with Dr. Jonathan Wright. In practice for 52 years. My Current Age 75.
Dr Wright taught hormones and gut health were the most important. He had heidelberg capsule anaysis machine to test stomach acid production.
I wrote Hormone Deception about endocrine disruption. Basded on that book, I was invited to an estrogen think tank, and work as a distinuished estrogen scholar at Tulane Med SChool under John Mcclaughlin as my mentor. Worked with the scientists who discovered the first estrogen receptors. Jensen and Gustafson.
Women’s hormones are the most controversial and confusing topic in medicine today.
Most women are terrified of hormones, and really think estrogen is really a bad thing. This term estrogen dominance dominated the airways/ Lets have a conversation to clear some of this up.
very few doctors have heard of the re-analysis of the womens health initiative,
A big part of anti-aging comes from hippocamus volume. This is where memories and emotions, motivation, soul resides in brain. Hippocampus shrinks as we age.
Exercise and meditation does not preserve volume. However, HRT does preserve it.
Yale MedX study tracked volume of hippocampus.
Studies 20 years ago from McGill U by Catherine Lonhartford showed HRT restores hippocampus volume.
re-analysis of whi
peter attia
leon speroff said
Testosterone is Breast Cancer Preventive: Mechanism of Action
There are two estrogen receptors, Alpha and Beta. The Alpha receptor is pro-carcinogenic. The Beta Receptor is protective and suppresses carcinogenesis. Estradiol attached to both receptors 50:50. Estrone (E1) attaches mostly to ER-alpha, while Estriol (E3) attached mosty to ER Beta (protective). The most like likely mechanism for testosterone’s protective effect in breast cancer prevention is the testosterone metabolite 3β-Adiol which attaches to Estrogen Receptor Beta (ER-Beta), thus upregulated ER-Beta expression, thus inhibiting breast cancer cell growth.(38-49)
This is illustrated in 2014 by Dr. Pietro Rizzo who writes:
The two isoforms of estrogen receptor (ER) alpha and beta play opposite roles in regulating proliferation and differentiation of breast cancers, with ER-alpha mediating mitogenic effects and ER-beta acting as a tumor suppressor. …..Collectively, these data provide evidence for a novel mechanism by which activated AR [Androgen Receptor], through an up-regulation of ER-beta gene expression, inhibits breast cancer cell growth.(45) Emphasis Mine.
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Copyright (c) 2024 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on April 9th, 2024 by Jeffrey Dach MD
The post Errors in Modern Medicine: The Fear of Estrogen appeared first on Jeffrey Dach MD.
March 29, 2024
Increasing Childhood Autism and Cancer Rates
 Theresa Deisher on Increasing Childhood Autism and Cancer Rates
Theresa Deisher on Increasing Childhood Autism and Cancer Rates
by Jeffrey Dach MD
In 2017, Theresa Deisher MD presented her research studies on the causes of increasing childhood autism and cancer, implicating the childhood vaccine schedule as the main culprit. More specifically, it is the switch in vaccine manufacturing technique from animal cells to human fetal cells causing insertions mutagenesis in human stem cells, thus explaining for increasing autism and cancer rates. Hockey stick change point charts are quite convincing. Independent researchers have done studies in the gene therapy field.
Insertional Mutagenesis
To manufacture a \/axxine to a virus, the virus must first be replicated. However, viruses cannot replicate alone in a petri dish. In order to replicate, the virus must first enter a cell. Thus, the manufacturing process requires cells. In the past, animal cells were used. However, citing cost savings, the \/axxine manufacturer has been switched to human fetal cells. This creates the problem of DNA contamination inherent in using human fetal cells for viral replication. Massive amounts of cell debris including human fetal cell DNA contamination is present in the final \/axxine product, causing insertional mutagenesis, thus explainging rising childhood cancer and autism rates.
Hockey Stick Changes
Hockey stick change points occurred three times 1) when MMR \/axx manufacture was switched to human fetal cells, 2) when MMR vax rates were doubled from 40% to 80% in one year and the second MMR dose was added, and human fetal cell polio vaccine was introduced. 3) When the chickenpox vaccine was introduced, heavily contaminated with cell debris from the human fetal cell line. Later fetal cell hepatitis A was introduced further drove up autism rates.
When using human fetal cells to grow the virus for the \/axxine, a large amount of human cellular debris and human DNA remains in the sample. This is antigenic and invokes an immune response. There is also the problem of genome integration and insertional mutagenesis. When using animal cells, these problems do not arise. DNA contaminants in vaccines are incorporated 0.6% to 10 percent into DNA of human stem cells. These are mutations in human stem cells. Chldhood cancer have indeed gone up dramatically, such as Burkitt’s Lymphoma for example.
Dr Theresa Deisher’s Suggestions:
1) Umbilical stem cell infusions as treatment for autism are showing promise.
2) Ban the use of human fetal cells in manufacturing process for \/axxines
Watch Dr. Theresa Deisher’s presentation below:
Articles with related interest:
Which is Greater Threat, Measles or Measles Vaccine?
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
===================================================
Header image courtesy of HealthFreedom Ohio, Theresa Deisher and Soundchoice.com
1) Genes & Vaccines: Part B: Dr. Theresa Deisher
Problems inherent in using human fetal cell culture for viral replication. Massive amounts of Cell debris and human fetal cell DNA contamination in final \/axx product cause insertional mutagenesis, thus causing childhood cancer and autism rates to go up.
Hockey stick change points occurred three times 1) when MMR \/axx manufacture was switched to human fetal cell, 2) when MMR vax rates were doubled from 40% to 80% in one year and the second MMR dose was added, and human fetal cell polio vaccine was introduced. 3) The chickenpox vaccine introduced, was heavily contaminated with debris from the human fetal cell line. Later fetal cell hepatitis A was introduced further drove up autism rates.
When using human fetal cells to grow the virus for the \/axxine, a large amount of human cellular debris and human DNA remains in the sample. This is antigenic and invokes an immune response. There is also the problem of genome integration and insertional mutagenesis.
When using animal cells, these problems do not arise.
DNA contaminants in vaccines are incorporated 0.6% to 10 percent into DNA of human stem cells. These are mutations in human stem cells. Chldhood cancer have indeed gone up dramatically, such as Burkitt’s Lymphoma for example.
Suggestions:
1) umbilical stem cell infusions as treatment for autism showing promise.
2) Ban the use of human fetal cells in manufacturing process for \/axxines
This month Health Club members will hear from Theresa Deisher, Ph.D on the Commoditization of Human Beings and Potential DNA Mutagenesis of Vaccine Products.
Theresa A. Deisher, Ph.D. graduated from Stanford University School of Medicine with a doctoral degree in Molecular & Cellular Physiology. She has over 47 issued patents and 4 discoveries in clinical trials. She has had extensive scientific and management experience in the commercial biotechnology field at Genentech, Repligen, ZymoGenetics, Immunex, and Amgen. Dr. Deisher is the founder of both AVM Biotechnology and Sound Choice Pharmaceutical Institute.
Through the nonprofit Sound Choice Pharmaceutical Institute, Dr. Deisher researches and lectures on the scientific and medical implications of using aborted fetal material in vaccine manufacturing. At AVM Biotechnology, she and her team of scientists have developed a drug with a novel Mechanism of Action that mobilizes the body’s own natural immune cells to fight cancer and potentially COVID-19. Dr. Deisher was also one of the plaintiffs in the Sherley vs. Sebellius lawsuit that shut down embryo stem cell research and was an advisor to David Daleiden in the undercover filming of Planned Parenthood employees discussing the sale of aborted fetal parts for research.
Members will also hear from our lobbyist, Barry Sheets, on legislative directives and updates on bills we are interested in.
Please consider making a powerful impact by becoming an HFO Health Club Member and benefit from the monthly conference calls that will help us lead the way through these challenging times.
Health Club Memberships begin at $5/month or $60/year and go a long way in utilizing all of our resources to rise up triumphantly as we collectively strategize and proactively work together to preserve our rights. We know these are difficult times with extraordinary circumstances, which means we need to unite in these efforts. Your support is crucial to our overall success as a community of empowered individuals united to preserve that which is most sacred. Your health. Your life. Your way.
Link for memberships: https://healthfreedomohio.org/Join-us
———-
Also, please consider signing up for the upcoming webinar and fundraiser from Sound Choice featuring Robert F. Kennedy, Jr., Del Bigtree, Dr. James Neuenschwander, and many more powerful speakers. The event takes place this Saturday 10/24 from 5:00-7:30 PST.
The link to buy tickets: https://soundchoiceorg.regfox.com/hope-health-now.
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright (c) 2023 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on March 29th, 2024 by Jeffrey Dach MD
The post Increasing Childhood Autism and Cancer Rates appeared first on Jeffrey Dach MD.
Jeffrey Dach's Blog

- Jeffrey Dach's profile
- 3 followers


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}