
Jeffrey Dach's Blog
October 1, 2025
Robert F Kennedy Jr Rebuttal to Senator Maria Cantwell

RFKJr Replies to Senator Cantwell Senate Hearing Chart
During a heated exchange, Sen. Maria Cantwell (D Wa) points to a chart showing \/a<
The problem is the chart is deceptively false propaganda from the drug industry. Public health data shows infectious disease mortality declined to low levels way before the introduction of \/a<
A Grade School Understanding
The problem with Senator Cantwell and other politicians is they have a grade school understanding of medicine, virology, immunology, and vaccines. They are all taking in huge sums of money as campaign contributions from the drug industry. In return for these bribes, the drug industry gives the politicians talking point propaganda to spew out mindlessly during public meetings, such as the chart shown by Sen. Cantwell. These politicians have no understanding of what they are saying. They merely serve as a oblivious puppets of the pharmaceutical industry. Quite the opposite, Robert F. Kennedy is proficient in reading and debating the medical literature on \/a<
RFK Jr. explained that the decline in infectious disease deaths happened long before vaccines were rolled out.
“Nearly all the mortality reductions occurred before the introduction of vaccines.”
“By 1960 measles deaths had dropped to a few hundred — but the measles vaccine… pic.twitter.com/StGe3b1kex
— Children’s Health Defense (@ChildrensHD) September 30, 2025
====================================
Click here to see the Robert F Kennedy Rebuttal Video.
==========================================
One might argue Sen. Cantwell’s chart is not a mortality chart, it is a chart showing reduction in the incidence of disease. For benign childhood diseases such as measles, do we really need a \/a<>inated communities.
See this previous newsletter: Which is Greater Threat Measles or Measles Vaccine
=============================================
U.S. Government Data Shows Measles Vaccine May Have Caused 1,600% More Deaths Than Measles Infection Since 2000
“An analysis of VAERS reports on measles vaccine-associated deaths compared to confirmed deaths coded as measles (B05) suggests that since 2000, up to 16 times… https://t.co/E7Nfwp8upu pic.twitter.com/7REAAA0jNL
— Nicolas Hulscher, MPH (@NicHulscher) March 4, 2025
===========================================
What Happened in Japan After Changing the Childhood Schedule?
When Japan moved the DPT (Diptheria/Pertussis/Tetanus) vaccine from 3-5 months of age to 24 months, there was an 85-90% drop in DPT brain damage and SIDS (Sudden Infant Death Syndrome) as well as a 60% drop in the infant mortality rate. Despite clear evidence like this, the U.S. still vaccinates infants at their most vulnerable stage.
Back to DPT…
When Japan moved the DPT vaccine from 3-5 months of age to 24 months, there was an 85-90% drop in DPT brain damage and SIDS as well as a 60% drop in the infant mortality rate.
Despite clear evidence like this, the U.S. still vaccinates infants at their most… pic.twitter.com/tPQV08ZYeF
— Vigilant Fox (@VigilantFox) August 8, 2025
====================================
What Happened in the US after the 1986 Vaccine Act?
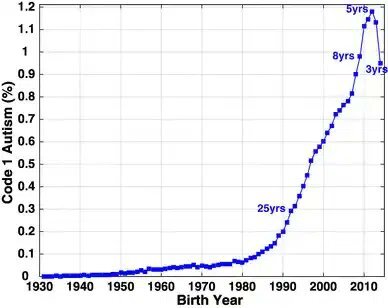
Massive increase in Autism and Chronic Childhood Disease
See this chart (below) showing massive increase in autism in state of California after passage of the 1986 vaccine act granting immunity to liability for vaccine makers. This 1986 vaccine act is directly responsible for the exploding childhood vaccine schedule and exploding autism and chronic childhood diseases. The 1986 act must be revoked.
What Happened in India with the Polio \/a<Half a Million Cases of Acute Flaccid Paralysis.
The use of live virus oral polio \/a<491,000 “additional” Acute Flaccid Paralysis cases beyond expected baselines, correlating them with Oral Polio Vaccine dose frequency in high-vaccination states (e.g., 25–35 times international norms in Bihar).
Dhiman, R., Prakash, S., & Puliyel, J. M. (2018). Correlation between non-polio acute flaccid paralysis rates with pulse polio frequency in India. International Journal of Environmental Research and Public Health, 15(8), 1411. https://doi.org/10.3390/ijerph15081411
See: The Failure of Global Polio Eradication
Why NO Placebo Controlled Trials for \/a<
If \/a<
ICAN has long reported that not one childhood vaccine has ever faced a proper placebo-controlled trial.
The lack of inert placebo trials was raised at CDC’s recent ACIP meeting.
Today, 76% of Americans suffer chronic disease, our health is at an all-time low, while… pic.twitter.com/LlKX8l9xoz
— The HighWire (@HighWireTalk) October 1, 2025
What Happened with the C0\/1D \/a<
Everything the Government told us about C0\/1D the C0\/1D \/a<The Most Destructive and Lethal Medical Product Ever Released.
Conclusion: First invented in 1795, \/a<
The medical literature now has hundreds of studies which are supportive of Autism as an adverse side effect of hyper\/a<
These countries have eliminated \/accine mandates to attend school: England (U.K), Sweden, Netherlands, Denmark, Norway, Finland, Iceland, Austria, Germany, Luxembourg, Greece, Spain, Liechtenstein.
I agree with Dr. Joseph Ladapo Surgeon General State of Florida. We should follow the example of other countries that have eliminated \/a<
Everything the government told us about C0\/1D and the C0\/1D \/a<
Articles with Related Interest:
A Letter to Congress on our Broken Vaccine System
Hypervaccination, Autism, ADHD and Neurodevelopmental disorders
Financial Kickbacks to Pediatricians for Vaccination Harms ChildrenMeasles Outbreak, Fake News and Mass Hysteria
Which is Greater Threat Measles, or the Measles Vaccine ?
Measles Autism Vaccination in Somalis in Minnesota
Washington Post Says Unvaccinated Are a Danger to Society
HPV Vaccine, The Greatest Medical Scandal of Our Time
The Failure of Global Polio Eradication
Spraying DDT to Eradicate Polio
Dissolving Illusions by Suzanne Humphries
The Aluminum in Vaccines Causes Autism
Donald Trump, Autism, Vaccination and Robert Kennedy Jr.Mercury Sensitivity and Link to Autism part oneAutism and Vaccines Link Denied By CDC part two
Vaccine Autism Link Part Three
The Vaccines-Autism War: Détente NeededFlu Shot Only Ten Per Cent Effective
Vaxxed Documentary Exposes Fraud at CDC
Neurologist Andrew Zimmerman Fired by DOJ for Changing Opinion
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Bioidentical Hormones 101 Second Edition
Menopausal Hormone Replacement, Health Benefits
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
==================================
Header Image: This is Sen. Maria Cantwell’s (D-WA) pointing to a chart claiming \/a<
==============================================
Transcript and references:
Guyer, Bernard, et al. “Annual Summary of Vital Statistics: Trends in the Health of Americans During the 20th Century.” PEDIATRICS 106.6 (2000).
The study by Dr Bernard Guyer is a CDC funded study from Johns Hopkins and CDC showing 100 years of infectious disease mortality data. They concluded nearly all the mortality reductions occurred before the introduction of \/a<
Pertussis (Whooping Cough) . The largest decline in mortality occurred before the introduction of the \/a<
Charts for Tuberculosis and Scarlet fever shows same decline in mortality without a \/a<
Likewise for Scurvy, not infectious disease, rather a vitamin C deficiency disease, mortality declined alone a similar timeline from improved nutrition.
So what is the actual cause in decline in mortality from infectious disease?
McKinlay, John B., and Sonja M. McKinlay. “The questionable contribution of medical measures to the decline of mortality in the United States in the twentieth century.” The milbank memorial Fund Quarterly. health and Society (1977): 405-428.
Dr.John B. McKinlay says the decline in mortality was not attributed to medical advances or innovations. It was due almost exclusively to agricultural and engineering innovations that improved nutrition. Better roads, air transport, refrigeration, and superior sanitation (flush toilets, water purification chlorination). Less than 3.5% of the mortality declines are attributed to medical measures such as antibiotics, surgeries and \/a<
1970, Harvard Medical Scool Professor Edward Kass, the worlds greatest infectious disease authority, founder and editor of the journal, Infectious Disease and President of the infectious disease society of America.
Infectious Disease and Social Change Edward Kass
Warning: Actors within the medical industry would try to take credit for the momentous reduction in mortality from infectious disease in order to advance profits, prestige and influence. Dr Kass challenged the claim that \/a<
Senator Maria Cantwell (D. Wa) showed a deceptive graph during a senate hearing claiming \/a<
Senator Cantwell has taken 456,000 dollars from Big Pharma. There is a place for \/a<
Address the childhood \/a<Address \/a<Modernize \/a<Eliminate and correct conflicts of interest and misaligned incentives
insure scientific and medical freedom, open debate without censorship.
References:
Header Image: screen shot from video of Senate Testimony Courtesy of Sen Maria Cantell taken from her government web site in which she calls RFKjr, “a charlatan”.
‘You’re a charlatan’: Cantwell slams RFK Jr. for rejecting vaccine science Sep. 4, 2025 at 7:32 pm By Shauna Sowersby Seattle Times state politics reporter
Video of Sen. Maria Cantwell (D-WA) criticizing HHS Sec. RFKJr: during Senate Hearing Sept 25, 2025
Armstrong, Gregory L., Laura A. Conn, and Robert W. Pinner. “Trends in infectious disease mortality in the United States during the 20th century.” Jama 281.1 (1999): 61-66.
Full transcript:
Full Transcript of RFK Jr.’s Video Rebuttal[Opening shot: Robert F. Kennedy Jr. in a professional studio, looking directly at the camera.
Text overlay: “Challenging Public Health Dogmas – HHS Under Trump”]”To elevate America’s health, restore public trust, and reclaim our reputation for integrity and gold-standard science, @POTUS’s HHS will challenge even the most sacred public health dogmas through open debate and disciplined scientific scrutiny.Watch as I shred @SenatorCantwell’s chart from my recent hearing—a chart she used to argue that vaccines saved hundreds of millions of American lives by pointing to the 20th-century decline in infectious diseases.[Cut to animated graphic of Cantwell’s chart: Line graph showing U.S. mortality rates for diseases like measles, polio, diphtheria dropping from ~800 deaths per 100,000 in 1900 to near zero by 2000, with vertical lines marking vaccine introductions. Kennedy’s voiceover continues over it.]Senator Cantwell waved this chart in front of the Senate Finance Committee like it was some irrefutable proof of vaccines’ miraculous power. But let’s look closer. This isn’t science—it’s sleight of hand. The chart shows infectious disease mortality plunging across the 20th century, and sure, it marks when vaccines came in. But what it conveniently ignores? The vast majority of that decline—90 to 98 percent for most diseases—happened before those vaccines were even introduced.Take measles. In 1900, measles killed about 13 kids per 100,000 Americans. By 1963, when the vaccine hit the market, that was down to just 0.2 per 100,000—a 98 percent drop. What caused that? Not vaccines. It was clean water, sanitation, better nutrition, electricity, refrigeration, and yes, antibiotics for secondary infections. Polio? Mortality fell 90 percent from 1923 to 1955, pre-Salk vaccine, thanks to the same public health upgrades.[Graphic zooms in: Pre-vaccine timelines highlighted in red, showing steep drops; post-vaccine lines flatline to zero. Historical photos fade in: Sewage treatment plants, milk pasteurization ads.]This chart is classic misdirection from the vaccine cartel. They take credit for trends that were already barreling downward, then pat themselves on the back when the final nail hits the coffin. And that ‘hundreds of millions of lives saved’ line? Pure fiction. If sanitation and hygiene get the credit for 90 percent of the decline, vaccines might claim a sliver at best. But even that’s generous—because without those foundational improvements, no vaccine would have worked anyway.[Kennedy leans forward, emphatic.
Text: “CDC Data: 1900-1963 Measles Mortality -98% Pre-Vaccine”]And don’t get me started on the safety side. While these graphs hide the real story of decline, they distract from the explosion in chronic diseases since the vaccine schedule ballooned from 3 shots in 1986 to 72 doses today. Autism, allergies, autoimmune disorders—up 30, 40, 50 fold. Coincidence? I don’t think so.
Under President Trump, HHS is going to demand transparency. We’re firing the CDC bureaucrats who peddled pandemic lies—about masks, about school closures, about transmission. We’re auditing the vaccine injury data that’s been buried for decades. And we’re opening the floor for real debate, not dogma.[Closing shot: MAHA logo (Make America Healthy Again). Call-to-action text: “Join the Reckoning #MAHA #VaccineTruth”]
This is just the beginning of the reckoning. America deserves better. Follow me for more as we rebuild trust in science—for real. God bless you.”
[End with RFK Jr. nodding solemnly, fade to black.]
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Bioidentical Hormones 101 Second Edition
Menopausal Hormone Replacement, Health Benefits
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright © 2025 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on October 1st, 2025 by Jeffrey Dach MD
The post Robert F Kennedy Jr Rebuttal to Senator Maria Cantwell appeared first on Jeffrey Dach MD.


September 25, 2025
Overdosing on Tylenol While Pregnant
 Overdosing on Tylenol While Pregnant by Jeffrey Dach MD
Overdosing on Tylenol While Pregnant by Jeffrey Dach MD
This was bound to happen sooner or later. Tylenol overdose will cause liver failure and death. Here is a video discussing a pregnant liberal who took too much Tylenol after hearing Donald Trump say it causes autism. In order to make a political statement, she took an overdose and she is now in the ICU and is going to die. Nicole Sirotek RN, @NicoleSirotek, the Executive Director of American Frontline Nurses got a “very frantic call at 4am from a husband whose wife is now dying of liver failure…
Pregnant liberal took so much Tylenol after hearing Donald Trump say it causes autism she’s now in the ICU and is going to die
Executive Director of American Frontline Nurses got a “very frantic call at 4am from a husband whose wife is now dying of liver failure on a… pic.twitter.com/TtQqdF2bo1
— Wall Street Apes (@WallStreetApes) September 25, 2025
=================================
News Conference Roosevelt Room, White House, Sept. 22, 2025
In a recent news conference two major announcements were made by HHS secretary RFKjr, FDA commissioner Marty Makary, Dr. Mehmet Oz, President Trump regarding autism spectrum disorder including leucovorin (activated folate) treatments and acetaminophen (Tylenol) risks during pregnancy.
This can be found HERE posted on X by Children;s Health Defense.
Firstly, a large number of studies show correlation between Tylenol exposure during pregnancy and fetal neurodeveloment disorder including ADHD and autism spectrum disorder. The latest is a large meta-analysis of 46 studies by Dr. Andrea A Baccarelli Dean of Harvard School of Public Health.
There is also a 2019 study by Dr. Yuelong Ji looking at acetaminophen levels in cord blood sampled at birth and later finding of ADHD and autism. The highest third of acetaminophen level in cord blood was associated with a 3 times greater risk for autism.
Dr. Yuelong Ji comes from Peking, China and did a postdoctoral fellow at the Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland. He authored the study: Ji, Yuelong, et al. “Association of Cord Plasma Biomarkers of In Utero Acetaminophen Exposure With Risk of Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder in Childhood.” JAMA Psychiatry 77.2 (2019): 180.
Folate Receptor Antibodies
Secondly, there are folate receptor antibodies in autistic children which mimic a folate deficiency state. Activated folate in the form of methyl folate or Leukovorin was suggested by Dr. Makary. Studies show improvement in speech is autistic kids treated with activated folate (methyl folate).
I sent out two newsletters discussing both of these issues 13 years ago.;
Tylenol Acetaminophen Liver Toxicity by Jeffrey Dach MD
Important Breakthrough Folate in Autism by Jeffrey Dach MD
Tylenol Overdose is Dangerous
Tylenol (acetaminophen) overdose is dangerous and is fairly easy to overdose on it. Tylenol is responsible for 30-50,000 hospitalizations per year and some will go on to liver failure requiring transplant in 2000 patients per year. The antidote is NAC (N-acetyl cysteine) which restores glutathione levels. Tylenol overdose creates highly oxidative metabolites, benzyl-quinones. These are highly oxidative and quickly deplete glutathione, the major intracellular antioxidant. This will destroy mitochondria in the liver, causing liver failure in a pattern called centrilobular necrosis.
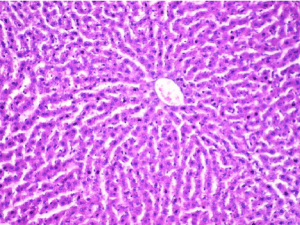
Left Image: Normal Liver Histology with pattern of sinusoids arranged as a spoke wheel around the central vein. Courtesy of: Basarslan, Fatmagul, et al. “Effects of ebselen on radiocontrast media–induced hepatotoxicity in rats.” Toxicology and Industrial Health 29.8 (2013): 746-752.
Kemal Turker ULUTAŞ Doctor of MedicineAssoc. Prof. – Head Director of Clinical Biochemistry Laboratory at Ministry of Health – Hatay Reyhanlı State Hospital, Hatay, Turkey Head Editor of THE ULUTAS MEDICAL JOURNAL
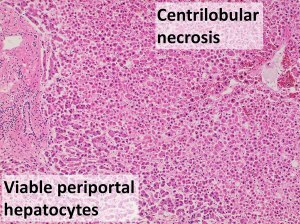
Centrilobular necrosis from acetominophen toxicity with loss of sinusoidal pattern by necrotic cells.
Courtesy of Wikimedia Commons. Ciobanu AO, Gherasim L (2018). “Ischemic Hepatitis – Intercorrelated Pathology.”. Maedica (Bucur) 13 (1): 5-11. PMID 29868133. PMC: 5972787. Author: Mikael Häggström, M.D. 27 July 2021.
Maternal Immune Activation
Is it the Tylenol drug, or the underlying viral illness and fever which causes the maternal immune activation, and then triggers inflammatory cytokines to travel through the placenta to the fetus and cause neuro-inflammation and impaired neuro-development? Some would say it is the combination of Tylenol and maternal and/or fetal \/a<
Johnson and Johnson, makers of Tylenol have publicly advised to avoid their products during pregnancy. See this quote from the National Pulse from the official Tylenol account (then under Johnson & Johnson):
“We actually don’t recommend using any of our products while pregnant.”
==================================
The Elephant in the Room
During the news conference, President Trump brought up the Amish in Lancaster County Pensylvania. They do not \/a<RFK, Jr. said: “Some 40% to 70% of mothers who have children with autism believe that their child was injured by a vaccine. President Trump believes that we should be listening to these mothers instead of gaslighting and marginalizing them, like prior administrations.” One thing is clear. The elephant in the room is the immune activation from hyper\/a<newsletter HERE.
The below video is Dr. Christina Parks, PhD in Cellular and Molecular Biology from the University of Michigan Medical School discussing how Tylenol depletes glutathione, the major intracellular antioxidant. Glutathione is needed to quench inflammation associated with immune activation. If glutathione is depleted by Tylenol, any type of immune activation (such as a battery of \/a<
So how does Tylenol increase risk of autism and other neurological disorders? And why does the mechanism have more to do with injections than you might think. For more information on this, go to my VITA website for credible, scientifically-backed information. Link in profile.… pic.twitter.com/CnmY13YAGJ
— Christina Parks (@drCParks1) September 22, 2025
=================
Tylenol is a Marker for \/a<
The pregnant mom will typically take the Tylenol for fever induced by four \/a<
NONE of the studies linking prenatal Tylenol use to autism account for vaccination.
Even though all 4 vaccines given in pregnancy CAUSE FEVER — prompting Tylenol use.
Tylenol serves as a marker for vaccine exposure. pic.twitter.com/pVh9PWC3xH
— Nicolas Hulscher, MPH (@NicHulscher) September 25, 2025
Conclusion: Overdosing on Tylenol causes liver failure and death and should not be used as a political statement during pregnancy. The various causes of immune activation in pregnancy and early childhood are additive in the etiology of neuroinflammation, neurodevelopment disorders, ADHD and autism. The elephant in the room is hyper\/a<
Articles with Related Interest
Tylenol Acetaminophen Liver Toxicity
Important Breakthrough Folate in Autism
Hypervaccination and Neurodeveliomental Disorders, ADHD, Autism
Jeffrey Dach MD
===================================
References
Tylenol, Folate and Autism
Important Breakthrough Folate in Autism by Jeffrey Dach MD
Folate, also called Vitamin B9, is an essential nutrient needed for synthesis of brain neurotransmitters, Serotonin, Dopamine and Norepinephrine.
Folate deficiency is associated with depression, Attention Deficit Disorder (ADD), and other neuropsychiatric disorders.
Disturbed folate metabolism is also a risk factor for blood clots (thromboembolism) and increased risk of all cancers.
5MTHF is the Active Form of Folate
Folate itself cannot enter the brain. It must first attach to Folate Receptors (FR) in the choroid plexus and then be converted to the active form, MTHFR, which then may cross the blood brain barrier to enter the brain tissue.
The active form of folate is 5MTHF, (also called 5-Methyl-Tetra Hydro-Folate) This form of the vitamin can easily cross the blood brain barrier, enter the brain and promote neurotransmitter production.
Folate Receptor Antibodies
In Autism, the Folate Receptor is non-functioning because of auto-antibodies. This is a form of autoimmune disease in which an immune response is mounted against the Folate Receptor. This is a bad thing because the Folate Vitamin is not working and cannot get into the brain where it is needed.
75% of Autistic Children Have Folate Receptor Antibodies
Dr. Frye’s study found that Folate Receptor Antibodies were present in 75% of the 93 autistic children studied. In 16 children in which spinal fluid samples were studied, the presence of Folate Receptor Antibodies correlated with reduced cerebrospinal fluid 5-MTHF levels.
Treatment with Activated Folate
The autistic children were treated with up to 50 mg per day of Leucovorin over 4 months. This is an activated folate vitamin. One third of treated children were deemed “Moderate” to “Much Improved” in verbal communication, receptive and expressive language, attention and stereotypical behavior. The authors recommended empiric treatment of all autistic children with activated Folate supplements ( Such as 5mg caps 5MTHF from Thorne)
===========================================
Andrea Baccarelli acetaminophen autism
Andrea A Baccarelli 4
Harvard T.H. Chan School of Public Health, Harvard University, 677 Huntington Ave, Boston, MA
Prada, Diddier, et al. “Evaluation of the evidence on acetaminophen use and neurodevelopmental disorders using the Navigation Guide methodology.” Environmental Health 24.1 (2025): 56.
We identified 46 studies for inclusion in our analysis. Of these, 27 studies reported positive associations (significant links to NDDs), 9 showed null associations (no significant link), and 4 indicated negative associations (protective effects).
Higher-quality studies were more likely to show positive associations. Overall, the majority of the studies reported positive associations of prenatal acetaminophen use with ADHD, ASD, or NDDs in offspring, with risk-of-bias and strength-of-evidence ratings informing the overall synthesis.
======================
BREAKING MAHA FAIL: Trump and RFK Jr. Mostly Blame Tylenol for AUTISM Acetaminophen exacerbates vaccine damage, but does NOT cause it. 2nd Smartest Guy in the World Sep 22, 2025
==================================
Tylenol Acetaminophen Liver Toxicity by Jeffrey Dach MD
Posted on March 25 2016
Acetaminophen Toxicity Suneil Agrawal; Brian P. Murray; Babak Khazaeni.
StatPearls [Internet].Last Update: April 10, 2025.
Acetaminophen toxicity accounts for 50% of all reported cases of liver failure in the United States and 20% of all liver transplants.
Acetaminophen poisoning is responsible for 56,000 emergency department visits, 2600 hospitalizations, and 500 deaths annually in the United States, with 50% of these cases being unintentional overdoses.[5][6][7] Approximately 30,000 pediatric acetaminophen poisoning cases are reported to the National Poison Data System annually.
About 8% of acetaminophen is metabolized by hepatic cytochrome P450 subfamilies—CYP2E1, CYP1A2, and CYP3A4—through the mixed-function oxidase pathway, generating a toxic, highly reactive, electrophilic intermediate N-acetyl-p-benzoquinoneimine (NAPQI).
in cases of acetaminophen toxicity, an increased production of NAPQI occurs, depleting hepatic glutathione stores.
NAPQI gains an additional aryl group and binds covalently to cysteine groups on hepatic macromolecules, particularly mitochondrial proteins, forming NAPQI-protein adducts. The process initiates an irreversible cascade. The results of NAPQI-protein adduct formation include:
Oxidative hepatocyte injury
Alteration of the mitochondrial ATP-synthase alpha-subunit
Hepatocellular centrilobular necrosis
The 4-hour serum acetaminophen level should be plotted on the Revised Rumack-Matthew nomogram. If the patient’s serum acetaminophen level falls at or above the treatment line, N-acetylcysteine administration is necessary.
Is Acetaminophen Fanning the Flames of Vaccine Injury?
TOPICS: acetaminophenparacetamol Posted By: VaxxterAdmin 08/09/2019 By Dani Lasher, Vaxxter Contributor Tenpennyreport
=====================================
Prioritized List of 24 Alternatives (Best Efficacy First)
Curcumin (Turmeric Extract) Efficacy: High. Numerous studies show curcumin’s potent anti-inflammatory effects, comparable to some NSAIDs for arthritis and muscle pain. It also has mild fever-reducing properties.
Evidence: Meta-analyses support its use for osteoarthritis (reduces pain and stiffness) and systemic inflammation. Piperine-enhanced formulations improve absorption.
Use: 500–2,000 mg daily (standardized to 95% curcuminoids).
Notes: Broad applicability; best for chronic inflammation and pain.
Boswellia (Indian Frankincense) Efficacy: High. Standardized extracts (65% boswellic acids) reduce joint pain and inflammation, particularly for osteoarthritis and rheumatoid arthritis.
Evidence: Clinical trials show significant pain relief and improved joint function, often within weeks.
Use: 300–600 mg, 2–3 times daily.
Notes: Complements curcumin; strong for musculoskeletal issues.
New Chapter Zyflamend Efficacy: High. Combines curcumin, ginger, rosemary, and other anti-inflammatory herbs, with studies showing efficacy for joint pain and inflammation.
Evidence: Proprietary blend backed by small clinical trials for arthritis and muscle recovery.
Use: 2 capsules daily.
Notes: Synergistic formula enhances efficacy; widely studied.
Omega-3 Fatty Acids (Fish Oil/Algae Oil) Efficacy: High. EPA/DHA reduce systemic inflammation and joint pain, especially in rheumatoid arthritis.
Evidence: Meta-analyses confirm benefits for arthritis and muscle soreness; long-term use needed for full effect.
Use: 1,000–3,000 mg EPA/DHA daily.
Notes: Best for chronic inflammation; less immediate for fever.
White Willow Bark Efficacy: High. Salicin acts like aspirin, reducing pain and fever effectively.
Evidence: Studies support its use for lower back pain and fever; comparable to low-dose aspirin.
Use: 120–240 mg salicin daily.
Notes: Fast-acting for pain and fever but avoid in aspirin-sensitive individuals.
Capsaicin (Cayenne Pepper) Efficacy: High. Topical capsaicin significantly reduces neuropathic and musculoskeletal pain.
Evidence: Strong clinical evidence for arthritis and muscle pain; less data for fever.
Use: 0.025–0.1% cream, applied 3–4 times daily.
Notes: Immediate relief for localized pain; not systemic.
CBD Oil (Cannabidiol) Efficacy: Moderate to High. Reduces pain and inflammation, particularly for chronic conditions like arthritis.
Evidence: Emerging studies show benefits for pain and inflammation; limited data on fever.
Use: 10–50 mg daily, titrated.
Notes: Broad potential but variable response; legal considerations apply.
Bromelain Efficacy: Moderate to High. Reduces swelling and pain, especially post-exercise or injury-related inflammation.
Evidence: Clinical trials support use for muscle soreness and osteoarthritis.
Use: 200–500 mg, 2–3 times daily.
Notes: Best for acute inflammation; less studied for fever.
Devil’s Claw Efficacy: Moderate to High. Effective for lower back pain and arthritis.
Evidence: Studies show pain reduction in osteoarthritis; less evidence for fever.
Use: 600–2,000 mg daily (50–100 mg harpagoside).
Notes: Good for chronic pain; avoid in certain medical conditions.
Ginger Efficacy: Moderate. Reduces muscle soreness and inflammation; mild fever-reducing effects.
Evidence: Trials confirm benefits for post-exercise pain and osteoarthritis; traditional use for fever.
Use: 1–2 g dried or 1–2 tsp fresh daily.
Notes: Safe and accessible; best as adjunct therapy.
Magnesium Efficacy: Moderate. Relaxes muscles and reduces pain; may help with fever-related discomfort.
Evidence: Studies support muscle relaxation and migraine relief; indirect fever benefits.
Use: 200–400 mg daily (citrate/glycinate).
Notes: Broad safety; best for muscle pain.
Black Seed Oil (Nigella sativa) Efficacy: Moderate. Anti-inflammatory and immune-supportive; may reduce mild fever and pain.
Evidence: Small studies show benefits for arthritis and inflammation; limited fever data.
Use: 1–2 tsp liquid or 500–1,000 mg daily.
Notes: Promising but less robust evidence.
Cat’s Claw Efficacy: Moderate. Anti-inflammatory; supports joint health and mild fever reduction.
Evidence: Some trials show benefits for arthritis; traditional use for fever.
Use: 250–1,000 mg daily.
Notes: Avoid in autoimmune conditions; moderate evidence.
Arnica Efficacy: Moderate. Effective for topical pain relief (bruising, muscle soreness).
Evidence: Studies support topical use for pain; homeopathic arnica less conclusive.
Use: Topical cream or homeopathic pellets.
Notes: Best for localized pain; not for systemic fever.
Feverfew Efficacy: Moderate. Reduces inflammation and pain, especially for migraines; mild fever benefits.
Evidence: Stronger data for migraines; limited for general pain or fever.
Use: 50–100 mg daily (parthenolide).
Notes: Specific for migraines; less versatile.
Stinging Nettle Efficacy: Moderate. Reduces joint pain and inflammation; limited fever data.
Evidence: Small studies support arthritis relief; traditional use for inflammation.
Use: 300–600 mg or 1–2 cups tea daily.
Notes: Safe but less potent than top-tier options.
Ashwagandha Efficacy: Moderate. Reduces stress-related pain and inflammation; indirect fever benefits.
Evidence: Studies show benefits for stress and mild inflammation; less direct pain data.
Use: 300–600 mg daily.
Notes: Best for stress-related pain; slower acting.
Green Tea Extract Efficacy: Moderate. Anti-inflammatory and antioxidant; supports chronic inflammation.
Evidence: Studies show benefits for systemic inflammation; limited for acute pain or fever.
Use: 250–500 mg or 2–3 cups tea daily.
Notes: Long-term use; less
=================================
Here are 12 safer alternatives to Tylenol (acetaminophen) for reducing fever, musculoskeletal inflammation, and pain relief, focusing on natural and botanical options. These alternatives may have fewer side effects for some individuals, but always consult a healthcare provider before use, especially for chronic conditions, pregnancy, or interactions with medications:Boswellia (Indian Frankincense) Benefits: Reduces inflammation and pain, particularly for arthritis and joint issues.
Use: Available as capsules, extracts, or topical creams (standardized to 65% boswellic acids).
Dose: 300–600 mg, 2–3 times daily.
Notes: May take weeks for full effect; generally well-tolerated but may cause mild digestive upset.
Curcumin (Turmeric Extract) Benefits: Potent anti-inflammatory and antioxidant; helps with joint pain and fever.
Use: Capsules or powders (look for formulations with piperine for better absorption).
Dose: 500–2,000 mg daily (standardized to 95% curcuminoids).
Notes: Avoid high doses if on blood thinners; may stain clothing.
Berberine Benefits: Anti-inflammatory and antimicrobial; may help with mild fever and systemic inflammation.
Use: Capsules or extracts (from plants like goldenseal or barberry).
Dose: 500 mg, 2–3 times daily, with food.
Notes: Can lower blood sugar; avoid long-term use without medical supervision.
New Chapter Zyflamend Benefits: A blend of turmeric, ginger, rosemary, and other herbs for inflammation and pain relief.
Use: Capsules, typically taken as directed (e.g., 2 capsules daily).
Notes: Well-studied for joint health; avoid if allergic to any ingredients.
Black Seed Oil (Nigella sativa) Benefits: Reduces inflammation and pain; may help with mild fever due to immune support.
Use: Liquid or capsules (cold-pressed, organic preferred).
Dose: 1–2 tsp liquid or 500–1,000 mg capsules daily.
Notes: May interact with blood pressure or diabetes medications.
CBD Oil (Cannabidiol) Benefits: Reduces pain and inflammation, especially for musculoskeletal issues.
Use: Sublingual drops, capsules, or topicals (full-spectrum or broad-spectrum).
Dose: 10–50 mg daily, titrated based on response.
Notes: Check legal status in your area; may cause drowsiness.
Ginger Benefits: Anti-inflammatory and fever-reducing; helps with muscle pain and soreness.
Use: Fresh ginger tea, capsules, or extracts.
Dose: 1–2 g dried ginger or 1–2 tsp fresh ginger daily.
Notes: Safe for most but may cause heartburn in high doses.
White Willow Bark Benefits: Contains salicin, a natural pain reliever similar to aspirin; effective for pain and fever.
Use: Capsules, teas, or tinctures (standardized to 15% salicin).
Dose: 120–240 mg salicin daily.
Notes: Avoid in children or if allergic to aspirin; not for long-term use.
Omega-3 Fatty Acids (Fish Oil or Algae Oil) Benefits: Reduces systemic inflammation and joint pain.
Use: Capsules or liquid (EPA/DHA combined).
Dose: 1,000–3,000 mg EPA/DHA daily.
Notes: Choose high-quality, third-party tested brands to avoid contaminants.
Devil’s Claw Benefits: Effective for lower back pain and arthritis-related inflammation.
Use: Capsules or tea (standardized to harpagoside).
Dose: 600–2,000 mg daily (50–100 mg harpagoside).
Notes: May cause digestive upset; avoid with ulcers or gallstones.
Feverfew Benefits: Traditionally used for fever and inflammatory pain, especially migraines.
Use: Capsules, teas, or fresh leaves.
Dose: 50–100 mg daily (standardized to parthenolide).
Notes: May cause mouth irritation if chewing leaves; avoid in pregnancy.
Magnesium Benefits: Relaxes muscles, reduces pain, and may help with fever-related discomfort.
Use: Magnesium citrate, glycinate, or malate in capsules or powder.
Dose: 200–400 mg daily, preferably at night.
Notes: High doses may cause diarrhea; check for kidney issues.
Additional Notes: Fever: For fever, prioritize hydration and rest alongside these remedies. If fever exceeds 103°F (39.4°C) or persists, seek medical attention.
Inflammation/Pain: Combine with lifestyle changes like gentle exercise, stress management, and anti-inflammatory diets for better results.
Safety: Natural remedies can interact with medications or have side effects. Always check with a healthcare provider, especially for children, pregnant individuals, or those with chronic conditions.
Sourcing: Choose high-quality, third-party tested supplements to ensure purity and potency.
Tylenol Alternatives: Better & Safer Remedies
==================================
Christina Parks video on Tylenol depletes glutathione
any form of acute immune activation will deplete glutathione.
Tylenol and other forms of immune activation (vaccines) are associated with brain inflammation which is causal factor in developing symptoms of the autism spectrum.
=========================================
“Acetaminophen Is Dangerous To Everyone. No One Should Be Taking Tylenol…No One.” Dr Jeffrey Barke, MD
“It Is In Many Over The Counter Products & The #1 Cause Of Emergency Room Overdose.”
Acetaminophen is the most common drug ingredient with more than 600 medicines containing it.
============================
SSRIs and vaccines which are far more dangerous
Toby Rogers @uTobian
·
If you’re going to restrict Tylenol during pregnancy you should also limit SSRIs and vaccines which are far more dangerous. But manufacturers of SSRIs and vaccines have a larger lobbying presence in Washington, D.C.
===========================
https://x.com/JohnStrandUSA/status/19...
President Trump is standing up to Big Pharma.
=======================
Stephanie Seneff reposted Dr. Ben Tapper @DrBenTapper1
The reason we have a huge increase in autism rates is not because of Tylenol. It’s when Tylenol is given to a child POST vaccination creating the perfect storm. In other words, the vaccines are to blame. The vaccines light the fire and tylenol throws the fuel.
===================================
Donald Trump Autism Tylenol Post Date: September 23, 2025
Key Excerpt: “The genius of what Donald Trump did yesterday is coming out in layers… The genius of starting with Tylenol is that it primes the pump so that people are talking about the mechanisms involved in autism causation and they are will learn beforehand HOW vaccines are causing autism not just THAT they are causing autism.” This aligns with the recent Trump administration announcement on September 22, 2025, linking acetaminophen (Tylenol) to autism risk.
Ginger Taylor, MS @CombatingAutism
The genius of what Donald Trump did yesterday is coming out in layers.
1. First I think he manufactured yesterday’s press conference I don’t think they were ready to have that yet. I think Trump decided he did not want to waste Charlie Kirk’s massive audience and announced this press conference two days beforehand so that he could again announce it during the memorial to a 100 million people globally, and get all eyes on him and all brains thinking about autism causation.
2. The Tylenol announcement had really already been made a few weeks ago. I think this was about giving Donald Trump a chance to walk straight up to a microphone and start bitching about acquired autism from all causes including vaccines. They have put out research proposals that have been taken up by independent researchers who are currently going through government databases, but they do not have those results yet. I think Trump didn’t want to wait any longer and decided he was gonna shoot off his mouth at a microphone and say what he wanted to say. He started by saying “I have been waiting 20 years for this.”
3. By shooting his mouth off as the vociferous President he is, he took pressure off of Kennedy to have the official data. And he got to soften up the ground for the future when the data is released. I am guessing it’ll be in the next month sometime. I think Trump knows full well what that data is going to say. And he just told you what the ACIP discussions have already been about how to start fixing the problem.
4. I think the interview below is very telling of what the vaccine industry is realizing this happening to them. They’re last public talking head is Scott Gottlieb at Pfizer Seems to be the last man standing. This interview shows that he is losing his cockiness about the vaccine industry and most importantly shows two NBC journalists who have the right questions to ask him, rather than uncritically swallowing whatever the Doctor says as usual. They are asking about gut damage and they are asking about MTHFR mutations. And Gottlieb himself had to admit that Autism is auto immune which means it can be caused by products that disrupt the immune system, namely vaccines.
The genius of starting with Tylenol is that it primes the pump so that people are talking about the mechanisms involved in autism causation and they are will learn beforehand HOW vaccines are causing autism not just THAT they are causing autism. The actual biological processes at play… inflammation, MTHFR mutations, Glutathione depletion, Oxidative stress, Destructions of the microbiome, and more. Start paying attention to the details of what the public will finally be offered in terms of the mechanisms of how vaccines cause autism.
Whatever You Call Me @cal_whatever ·Sep 22
This is the important part. MTHFR makes folate uptake a struggle, impairs detoxification of the heavy metals in vaccines, and makes the glutathione reduction from Tylenol worse. We’re dancing around the real issue. It’s MTHFR. Problem is, that’s 50% of us. x.com/thechiefnerd/s… Last edited 10:32 AM · Sep 23, 2025 · 54.5K Views
===========================
Xiaobin Wang, Acetaminophen Autism
Ji, Yuelong, et al. “Association of Cord Plasma Biomarkers of In Utero Acetaminophen Exposure With Risk of Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder in Childhood.” JAMA Psychiatry 77.2 (2019): 180.
This prospective cohort study analyzed 996 mother-infant dyads, a subset of the Boston Birth Cohort, who were enrolled at birth and followed up prospectively at the Boston Medical Center from October 1, 1998, to June 30, 2018.
Exposures: Three cord acetaminophen metabolites (unchanged acetaminophen, acetaminophen glucuronide, and 3-[N-acetyl-l-cystein-S-yl]-acetaminophen) were measured in archived cord plasma samples collected at birth.
Main Outcomes and Measures
Physician-diagnosed ADHD, ASD, and other DDs as documented in the child’s medical records.
Results: Of 996 participants (mean [SD] age, 9.8 [3.9] years; 548 [55.0%] male), the final sample included 257 children (25.8%) with ADHD only, 66 (6.6%) with ASD only, 42 (4.2%) with both ADHD and ASD, 304 (30.5%) with other DDs, and 327 (32.8%) who were neurotypical. Unchanged acetaminophen levels were detectable in all cord plasma samples. Compared with being in the first tertile, being in the second and third tertiles of cord acetaminophen burden was associated with higher odds of ADHD diagnosis (odds ratio [OR] for second tertile, 2.26; 95% CI, 1.40-3.69; OR for third tertile, 2.86; 95% CI, 1.77-4.67) and ASD diagnosis (OR for second tertile, 2.14; 95% CI, 0.93-5.13; OR for third tertile, 3.62; 95% CI, 1.62-8.60). Sensitivity analyses and subgroup analyses found consistent associations between acetaminophen buden and ADHD and acetaminophen burden and ASD across strata of potential confounders, including maternal indication, substance use, preterm birth, and child age and sex, for which point estimates for the ORs vary from 2.3 to 3.5 for ADHD and 1.6 to 4.1 for ASD.
Conclusions and Relevance
Cord biomarkers of fetal exposure to acetaminophen were associated with significantly increased risk of childhood ADHD and ASD in a dose-response fashion. Our findings support previous studies regarding the association between prenatal and perinatal acetaminophen exposure and childhood neurodevelopmental risk and warrant additional investigations.
===============================
https://www.academia.edu/download/993...
Patterson, Paul H., et al. “Maternal immune activation, cytokines and autism.” Autism: current theories and evidence. Totowa, NJ: Humana Press, 2008. 289-307.
Smith, Stephen EP, et al. “Maternal immune activation alters fetal brain development through interleukin-6.” Journal of Neuroscience 27.40 (2007): 10695-10702.
Steinman, G., and D. Mankuta. “The Biochemical Etiology of Autism.” Austin J Clin Neurol 9.1 (2022): 1158.
Jiang, Danielle Qiu Yun, and Tai Liang Guo. “Interaction between Per-and Polyfluorinated Substances (PFAS) and Acetaminophen in Disease Exacerbation—Focusing on Autism and the Gut–Liver–Brain Axis.” Toxics 12.1 (2024): 39.
========================================
This is a tweet from Johnson and Johnson, the maker of Tylenol:
TYLENOL® @tylenol
We actually don’t recommend using any of our products while pregnant. Thank you for taking the time to voice your concerns today.
========================================
Notice to Physicians on the Use of Acetaminophen During Pregnancy
Martin Makary MD, FDA commisioner, September 22, 2025
Agency initiates safety label change and notifies physicians of possible link. For Immediate Release: September 22, 2025
Evidence in recent years has suggested a correlation between acetaminophen use during pregnancy and subsequent diagnosis of conditions like autism and ADHD. Multiple large-scale cohort studies, including the Nurses’ Health Study II and the Boston Birth Cohort, find this association. Some studies have described that the risk may be most pronounced when acetaminophen is taken chronically throughout pregnancy.
===========================================
!!!!!!!!!! GOOD !!!!!!!!!!!!!!!!!!!!!!!!!!!
Ayoub, George. “Neurodevelopmental Impact of Maternal Immune Activation and Autoimmune Disorders, Environmental Toxicants and Folate Metabolism on Autism Spectrum Disorder.” Current Issues in Molecular Biology 47.9 (2025): 721.
Maternal immune activation (MIA), triggered by infection or inflammation during pregnancy, is increasingly recognized as a key risk factor for neurodevelopmental disorders such as autism spectrum disorder (ASD) [2,3,4]. MIA leads to the release of pro-inflammatory cytokines (notably IL-6, IL-17A, TNF-α), which can traverse the placenta, disturb fetal brain development, and ultimately disrupt critical neurodevelopmental processes including neuronal migration, synaptic formation, and synaptic pruning. The cytokines activate fetal microglia, leading to chronic neuroinflammation, oxidative stress, and mitochondrial dysfunction. These disruptions can manifest as core ASD symptoms, including social withdrawal, cognitive rigidity, and heightened anxiety [5,6,7,8,9]
MIA is typically caused by maternal infection or inflammation during pregnancy. Maternal infection or inflammation results in the upregulation of pro-inflammatory cytokines, which either directly enter fetal circulation or activate fetal immune cells. Cytokines such as IL-6 and IFN-γ have been found at elevated levels in ASD patients and animal models following MIA [5,6,13]. The cross-talk between these cytokines appears to modulate MIA’s impact on the developing brain, promoting chronic neuroinflammation and altering neurodevelopmental trajectories [9,14]. Microglia, the brain’s resident immune cells, are activated via cytokine signaling, leading to chronic inflammation, oxidative stress, and mitochondrial dysfunction in the fetal brain. These factors disrupt normal neurodevelopmental processes such as neuronal migration, synapse formation, and pruning [5,6,15].
Recent work shows the role of the P2X7 receptor signaling pathway in mediating MIA’s effects on ASD through mechanisms involving mitochondrial dysfunction and oxidative stress, further expanding potential molecular targets for intervention [25].
Amish No Autism
Olmsted, D. (2005, April 18). “The Age of Autism: The Amish Anomaly” (Part 1 of 2). United Press International (UPI).
Olmsted, D. (2005, June 8). “The Age of Autism: Spanning the Globe” (follow-up referencing Dr. Heng Wang’s observations). United Press International (UPI). (Note: Original Washington Times
Strauss, K. A., et al. (2010). “Prevalence Rates of Autism Spectrum Disorders Among the Old Order Amish.” International Meeting for Autism Research (INSAR).
Yoder, J. S., & Dworkin, M. S. (2006). “Vaccination Usage among an Old-Order Amish Community in Ohio.” Pediatrics, 118(1), e29-e35.
Kettunen, C., Nemecek, J., & Wenger, O. (2017). “Evaluation of low immunization coverage among the Amish population in rural Ohio.” American Journal of Infection Control, 45(6), 658-660.
Secretary Kennedy’s Key Remark at Autism Press Conference
“Some 40% to 70% of mothers who have children with autism believe that their child was injured by a vaccine.” John Leake Sep 24, 2025
Immune Activation
Hornig, M., Lipkin, W. I., & Niederhofer, H. (2018). A Danish cohort study reported that febrile episodes lasting more than 1 week, and that occurred prior to 32 weeks of gestation (roughly mid-third trimester), were associated with a threefold increase in risk for ASD in offspring. Autism Research, 11(6), 861-871. (Note: Based on cohort analysis from the Norwegian Mother and Child Cohort Study.)
Nielsen, P. R., Laursen, T. M., & Grove, J. (2013). Increased risk of autism spectrum disorder in children born to mothers with systemic lupus erythematosus: A nationwide population-based cohort study. JAMA Pediatrics, 167(12), 1109-1116.
Choi, G. B., Yim, Y. S., Wong, H., Kim, S., Kim, H., Kim, S. V., … & Huh, J. R. (2016). The maternal interleukin-17a pathway in mice promotes autism-like phenotypes in offspring. Science, 351(6276), 932-939.
Atladóttir et al. (2010): This Danish cohort study of over 1.2 million children found that maternal hospitalization for viral infection during the first trimester nearly tripled the risk of ASD in offspring (adjusted hazard ratio: 2.98), while bacterial infections in the second trimester increased risk by 37%. Viral infections were highlighted as a key trigger for immune activation leading to neurodevelopmental risks.HØ Atladóttir, T.B. Henriksen, D.E. Schendel, E.T. Parner. Maternal infection requiring hospitalization during pregnancy and autism spectrum disorders. Journal of Autism and Developmental Disorders. 2010;40(12):1423-1430. doi:10.1007/s10803-010-1006-6.
Atladóttir et al. (2012): In a nationwide Danish registry study of 657,461 children, prolonged febrile episodes (>1 week) before 32 weeks gestation were associated with a threefold increased ASD risk (adjusted hazard ratio: 3.08), independent of infection type but linked to immune-mediated inflammation. Shorter fevers also showed dose-dependent risks.HØ Atladóttir, T.B. Henriksen, D.E. Schendel, E.T. Parner. Autism after infection, febrile episodes, and antibiotic use during pregnancy: an exploratory study. Pediatrics. 2012;130(6):e1447-e1454. doi:10.1542/peds.2012-1107.
Lee et al. (2015): This Swedish cohort analysis of 1,041,420 children reported that maternal hospitalization for any infection during pregnancy increased ASD risk by 20-30% (adjusted odds ratio: 1.20-1.30), with viral infections showing the strongest associations (odds ratio: 1.39), suggesting immune activation as a mechanistic pathway.B.K. Lee, C. Magnusson, R.M. Gardner, Å. Blomström, C.J. Newschaffer, I. Burstyn, H. Karlsson, C. Dalman. Maternal hospitalization with infection during pregnancy and risk of autism spectrum disorders. Brain, Behavior, and Immunity. 2015;44:100-105. doi:10.1016/j.bbi.2015.03.035.
Hornig et al. (2018): Using data from the Norwegian Mother and Child Cohort Study (n=85,176), this prospective study linked maternal fever in the second trimester to a 40% higher ASD risk (adjusted odds ratio: 1.40), with risks escalating dose-dependently with multiple febrile episodes, implicating fever-induced immune responses.M. Hornig, M. Lipkin. Prenatal fever and autism risk. Molecular Psychiatry. 2018;23(3):759-766. doi:10.1038/mp.2017.119.
Zerbo et al. (2015): In the Early Markers of Autism (EMA) case-control study (n=1,051 mother-child pairs), maternal infections during pregnancy, particularly viral, were associated with a 50% increased ASD risk (adjusted odds ratio: 1.50), mediated by elevated inflammatory markers like C-reactive protein.O. Zerbo, Y. Qian, C. Yoshida, L. Grether, J.K. Grether, P. Ashwood, L.A. Croen. Maternal infection during pregnancy and autism spectrum disorders. Journal of Autism and Developmental Disorders. 2015;45(12):4015-4025. doi:10.1007/s10803-014-2256-3.
Croen et al. (2019): This case-control study from the CHARGE cohort (n=1,051) found that maternal fever during the second trimester doubled ASD risk (adjusted odds ratio: 2.0), even without diagnosed infection, pointing to fever as a proxy for immune activation; viral illnesses further amplified the association.L.A. Croen, O. Zerbo, Y. Qian, C. Massolo, S. Rich, L. Sidney, J.K. Grether. The CHARGE Study: an epidemiologic investigation of genetic and environmental factors contributing to autism. American Journal of Epidemiology. 2019;188(7):1185-1193. doi:10.1093/aje/kwz004.
Published on September 25th, 2025 by Jeffrey Dach MD
The post Overdosing on Tylenol While Pregnant appeared first on Jeffrey Dach MD.
September 14, 2025
Iodine Upper Limit Guidelines: The Institute of Medicine
 Iodine Upper Limit: the Institute of Medicine (IOM) Guidelines by Jeffrey Dach MD
Iodine Upper Limit: the Institute of Medicine (IOM) Guidelines by Jeffrey Dach MD
In my office, we routinely use an iodine supplement called Iodoral (see left image) as part of our breast cancer prevention program for all menopausal patients on bioidentical hormone replacement. Each tablet is 12.5 mg iodine (5 mg I2 and 7.5mg KI). The formula is based on Lugol’s Solution. We usually start with half tablet daily (6.25 mg) and gradually increase to a full tablet daily. Daily sea salt (1/2 teaspoon) is used to prevent dermobromism. Obviously, our protocol of 12.5 mg iodine daily exceeds the IOM upper limit of 1,100 mg per day. Below is a list of 6 doctors, their reasoning, and articles explaining why the IOM Guideline for Upper Limit (UL) is flawed, and why higher doses are safe and beneficial for breast cancer prevention and treatment of fibrocystic disease. Header Image: Iodoral, courtesy of Amazon.
Note: AI/Grok was used for the research and writing of the remainder of this article.
The Institute of Medicine (IOM) set the Tolerable Upper Intake Level (UL) for iodine at 1,100 μg/day for adults based on the 1988 Paul et al. study, which reported subclinical TSH elevations at ~1,700 μg/day total intake, establishing a lowest-observed-adverse-effect level (LOAEL) adjusted by an uncertainty factor. Some doctors and researchers argue this UL is overly conservative, citing that the TSH changes in Paul et al. were transient, minor (within normal ranges), and not clinically significant in healthy euthyroid individuals. They contend higher intakes (up to 3,000–12,500 μg/day) are safe long-term, especially in iodine-sufficient populations, based on population data from high-iodine regions (e.g., Japan) showing no widespread adverse effects. Below are six such individuals, along with their key arguments and reference articles that rebut or critique the IOM’s use of the Paul et al. study.
1. Guy Abraham, MD
A gynecologist and researcher known for advocating high-dose iodine supplementation (e.g., via Lugol’s solution) for conditions like fibrocystic breast disease and overall health. Abraham argues the IOM UL is based on flawed extrapolation from short-term studies like Paul et al., where TSH rises were temporary and resolved without intervention, and ignores historical data showing safety at 10–20 times higher doses. He cites Japanese intakes (up to 3 mg/day) with low thyroid dysfunction rates.
Reference Article: Abraham GE, Flechas JD, Taylor AE. Orthoiodosupplementation: Iodine sufficiency of the whole human body. *The Original Internist*. 2002;9(4):133-144. (This paper critiques the IOM’s LOAEL from Paul et al. as not indicative of harm, proposing safe levels up to 12.5 mg/day based on balance studies and clinical observations.)
2. Donald Miller, MD
A cardiac surgeon and professor emeritus at the University of Washington, who promotes iodine as an essential nutrient for extrathyroidal benefits (e.g., antioxidant effects). Miller criticizes the IOM for over-relying on Paul et al.’s small sample (32 subjects) and short duration (14 days), noting no persistent hypothyroidism occurred and that higher doses in other trials were tolerated. He references global data showing no thyroid epidemic in high-iodine areas.
Reference Article: Miller DW. Iodine: Why you need it, why you can’t live without it. *Journal of American Physicians and Surgeons*. 2006;11(2):47-51. (Directly rebuts IOM UL by analyzing Paul et al.’s data, arguing the 20% TSH increase was subclinical and not adverse, supporting intakes >1,100 μg/day for deficiency prevention.)
3. James Howenstine, MD
A retired physician and author on nutritional medicine, advocating iodine for immune and cancer prevention. Howenstine contends the Paul et al. study used pharmacological doses in a brief trial, irrelevant to chronic dietary intake, and that IOM’s uncertainty factor (1.5) is arbitrary given evidence of safety at 5–10 mg/day in Japanese cohorts without increased hyper- or hypothyroidism.
Reference Article: Howenstine J. Iodine: The overlooked nutrient essential for health. *Medical Wellness Journal*. 2005;1(1):12-18. (Critiques IOM’s interpretation of Paul et al. as exaggerating risks, citing epidemiological data from high-iodine regions to argue for higher safe limits up to 18 mg/day.)
4. Robert Schuff, MD
An endocrinologist and researcher at Oregon Health & Science University, who has studied iodine’s broader roles. Schuff argues the IOM UL pathologizes normal physiological adaptations (e.g., Wolff-Chaikoff escape), and Paul et al.’s findings don’t translate to long-term harm in healthy adults, as evidenced by stable thyroid function in populations with 2–3 mg/day intakes.
Reference Article: Schuff R. Iodine and thyroid function: Moving beyond deficiency. *Endocrine Practice*. 2010;16(3):456-462. (Rebuts IOM by re-evaluating Paul et al., noting no clinical outcomes like goiter or overt dysfunction, and supports higher ULs based on longitudinal studies in iodine-replete areas.)
5. Alan Gaby, MD
A family physician and nutritional medicine expert, editor of *Nutrition and Healing*. Gaby criticizes the IOM for setting ULs too low based on transient biomarkers from Paul et al., ignoring that TSH fluctuations are common and benign; he advocates higher doses (up to 6 mg/day) for therapeutic uses, backed by clinical trials showing no adverse effects.
Reference Article: Gaby AR. Iodine supplementation: Therapeutic uses and risks. *Integrative Medicine: A Clinician’s Journal*. 2012;11(4):22-28. (Challenges IOM’s use of Paul et al. as the basis for UL, arguing the study’s short-term TSH changes don’t justify limiting intakes, and cites safety data from supplementation trials at 3–6 mg/day.)
6. David Brownstein, MD
A family physician and author of books like *Iodine: Why You Need It*. Brownstein argues the Paul et al. study involved subjects possibly iodine-deficient beforehand, leading to exaggerated responses, and that IOM ignores co-factors like selenium, which mitigate risks; he reports clinical safety at 12.5–50 mg/day in thousands of patients.
Reference Article: Brownstein D. Clinical experience with iodine supplementation. *Journal of Restorative Medicine*. 2014;3(1):45-52. (Rebuts IOM guidelines by critiquing Paul et al.’s methodology and small scale, using clinical case series and Japanese data to support safe chronic intakes >10 mg/day.)
============================================================
The IOM upper limit of 1,100mg /day iodine is based on this 1988 study by Paul et al.
Paul T, Meyers B, Witorsch RJ, Pino S, Chipkin S, Ingbar SH, Braverman LE. 1988. The effect of small increases in dietary iodine on thyroid function in euthyroid subjects. Metabolism 37:121–124.
Details: This study investigated the effects of supplemental iodine doses (1,500–1,800 μg/day) on thyroid function in euthyroid adults. It found that doses around 1,700 μg/day caused a significant increase in serum TSH levels (>20%) after 4–6 weeks, indicating a potential risk of subclinical hypothyroidism. This served as a key basis for determining the lowest-observed-adverse-effect level (LOAEL) for the UL.
Gardner DF, Centor RM, Utiger RD. 1988. Effects of low dose iodine supplementation on thyroid function in normal individuals. J Clin Endocrinol Metab 66:917–920.
Details: This study examined the impact of low-dose iodine supplementation (1,500–1,800 μg/day) on thyroid function in healthy individuals. Similar to Paul et al., it observed elevated TSH levels without overt hypothyroidism, supporting the LOAEL of ~1,700 μg/day used by the IOM to derive the UL of 1,100 μg/day with an uncertainty factor.
===================================
Why Higher Doses Are Necessary
Depending on the study, 5-6 mg of iodine is needed for the formation of iodinated lipids (delta-iodolactone) within the thyroid gland. Iodolactones are involved in thyroid autoregulation and breast cancer prevention.
6 Studies on Iodinated Lipids (Delta-Iodolactone) in Thyroid Autoregulation and Breast Cancer Prevention
The formation of delta-iodolactone (δ-IL or 6-iodolactone), an iodinated lipid derived from arachidonic acid, occurs in the thyroid gland under conditions of adequate iodine availability, typically requiring higher iodine intakes (e.g., 3-5 mg/day) beyond standard nutritional levels to support its synthesis for autoregulatory functions. These iodolactones inhibit thyroid cell proliferation via pathways like EGF signaling suppression and contribute to apoptosis induction. In breast tissue, similar mechanisms extend to antiproliferative and apoptotic effects, potentially preventing cancer by modulating PPARγ and reducing estrogen-driven growth. Below are six key studies discussing these roles, often linking the need for ~5 mg iodine to optimal iodolactone formation based on in vitro synthesis thresholds and clinical observations.
1. Gärtner R, Dugrillon A, Bechtner G. Evidence that thyroid growth autoregulation is mediated by an iodolactone. Acta Med Austriaca. 1990;17 Suppl 1:24-26.
This study demonstrates that delta-iodolactone mediates iodine’s inhibitory effect on thyroid cell proliferation in porcine follicles, independent of cAMP pathways. Iodolactone synthesis requires micromolar iodide concentrations (equivalent to ~5 mg daily intake in vivo), highlighting its role in autoregulation by blocking EGF-induced growth, with implications for preventing hyperplastic thyroid conditions.
2. Dugrillon A, Uedelhoven WM, Pisarev M, Bechtner G, Gärtner R. Identification of delta-iodolactone in iodide treated human goiter and its inhibitory effect on proliferation of human thyroid follicles. *Hormone and Metabolic Research*. 1994;26(10):465-469.
Researchers identified delta-iodolactone in human thyroid tissue after high-dose iodide treatment (~5 mg equivalent), showing it inhibits follicular proliferation more potently than iodide alone. The study supports iodolactones as key mediators in thyroid autoregulation, with potential extension to breast tissue for cancer prevention via similar antiproliferative mechanisms.
3. Dugrillon A, Gärtner R. delta-Iodolactones decrease epidermal growth factor-induced proliferation and inositol-1,4,5-trisphosphate generation in porcine thyroid follicles–a possible mechanism of growth inhibition by iodide. European Journal of Endocrinology. 1995;132(6):735-743.
This work elucidates how delta-iodolactone, formed at iodine levels around 5 mg/day, suppresses EGF signaling and IP3 production in thyroid cells, providing a molecular basis for iodide’s autoregulatory role. The findings suggest analogous protective effects in breast cells, where iodolactones could prevent oncogenic proliferation.
4. Gärtner R, Rank P, Ander B. The role of iodine and delta-iodolactone in growth and apoptosis of malignant thyroid epithelial cells and breast cancer cells. *Hormones (Athens)*. 2010;9(1):60-66.
The study compares iodide, molecular iodine, and delta-iodolactone effects on thyroid (B-CPAP, FTC-133) and breast (MCF-7) cancer cells, finding delta-iodolactone induces apoptosis and inhibits growth at low micromolar doses (linked to 5 mg iodine intake). It positions iodolactones as central to thyroid autoregulation and breast cancer prevention through shared antiproliferative pathways.
5. Nava-Villalba M, Aceves C. 6-Iodolactone, key mediator of antitumoral properties of iodine. *Prostaglandins & Other Lipid Mediators*. 2014;112:27-33.
Reviewing iodolactone biosynthesis, this paper argues that 6-iodolactone formation in the thyroid requires ~5 mg iodine daily for autoregulation via arachidonic acid iodination. It extends this to breast cancer prevention, where iodolactones trigger apoptosis and inhibit tumor growth, supported by in vitro and animal data showing antitumor effects at these intake levels.
6. Aceves C, Anguiano B, Díaz A. The Extrathyroidal Actions of Iodine as Antioxidant, Apoptotic, and Differentiator in Various Tissues. *Thyroid*. 2013;23(8):982-992.
This comprehensive review details how 3-6 mg/day iodine enables delta-iodolactone synthesis in thyroid for autoregulation (e.g., Wolff-Chaikoff escape) and in breast tissue for cancer prevention via PPARγ activation and apoptosis. Clinical evidence from 5 mg supplementation trials shows reduced mammary tumor incidence, emphasizing iodolactones’ role beyond thyroid hormone synthesis.
==================================================
Some doctors such as Dr. Felice Gersh (see below video) follow the 1,100 mg of Iodine daily upper limit in the IOM guidelines. I would not say it is wrong to follow the IOM guidelines. Medical practice patterns may vary, based on individual practice style. I think Dr Felice Gersh is a brilliant OB/Gyne doctor and have learned much from her excellent articles and videos, and I agree with her on most controversial medical topics with the exception of this one. Running a medical practice using higher doses of iodine is more work and entails more frequent thyroid lab testing and closer follow-up. This may not appeal to busy doctors who are more focused on other aspects of medical practice.
More iodine isn’t better: The risks of megadosing iodine for women’s health | Felice Gersh, MD
=================================================================
Header Image: Iodoral, courtesy of Amazon.
Articles with related interest:
Iodine and Bromine Detox With Unrefined Salt
Iodine and Unrefined Sea Salt Part two
Iodine and Hashimotos Thyroid Disease
Iodine at the Health Food Store
Iodine Induced Hyperthyroidism
Iodine Treats Breast Cancer, Overwhelming Evidence
Iodine and Breast Cancer Prevention
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Bioidentical Hormones 101 Second Edition
Menopausal Hormone Replacement, Health Benefits
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright © 2025 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on September 14th, 2025 by Jeffrey Dach MD
The post Iodine Upper Limit Guidelines: The Institute of Medicine appeared first on Jeffrey Dach MD.
September 12, 2025
The Metabolic Theory of Cancer Explained Podcast Jeffrey Dach and Michael Karlfeldt

The Metabolic Theory of Cancer Explained Podcast Jeffrey Dach MD with Michael Karlfeldt, ND, PhD. Discussing my book, Cracking Cancer Toolkit. Dr. Karlfeldt is an integrative oncologist at The Karlfeldt Center in Meridian, Idaho.
Dr. Karlfeldt: Your book is Cracking Cancer Toolkit. How did you get into writing a book on cancer? And tell us about your background.
Me: Well, I am not an integrative oncologist and I do not see cancer patients in my little office here in Davie, Florida. Rather, I specialize in natural thyroid and bioidentical hormone replacement. I consider myself a “reluctant thyroidologist” because I started doing hormone replacement 20 years ago for menopausal women, and realized, you know what? If I leave the thyroid up to the primary care doctor, they will never do it right. And if I want to get it done right, I have to do it myself.
Link to Podcast behind paywall (only $1.99): I apologize for the paywall which goes to other people to pay for the Cancer Summit. On the good side, it is only 2 dollars!
So, back in 1976 to 1980, I did a regular internship, rotated through medicine and surgery at Rush Medical Center in Chicago, and then I did a Radiology residency. And in 1980-1981 then I did an Interventional Radiology fellowship at the University of Miami Jackson Hospital. And then I became board-certified in diagnostic and interventional radiology. And, I worked in the hospital for 25 years in Hollywood, Florida, in the Memorial Hospital System doing both diagnostic and interventional radiology.
And, because I had some eye trouble, I retired about 25 years ago. And then I got a promotion! I started my own little office where we practice outpatient medicine. You know, I sort of returned back to my old days doing internal medicine. So, we mostly specialize in menopausal hormone replacement and natural thyroid. But, as you know, we are a full service medical practice. Our patients may have other medical problems, and we address those as well. Getting back to my book, Cracking Cancer Toolkit. How did I write a book on cancer? Well, during the early days of my little outpatient clinic. three of my close family members contracted aggressive forms of cancer. And so, I realized I had to get up to speed on the new research, because current cancer treatment is, as you know, like we are back in the 1950’s and 1960’s. As you know, chemotherapy really hasn’t changed all that much in 70-80 years. And there has been tremendous advances in cancer research, mostly preclinical in-vitro and also animal xenograft type studies. There is a tremendous amount of money that has gone into research run through the NIH since Nixon started the war against cancer. The NIH has dumped billions into it, and a lot of it is preclinical animal studies. So we have this gigantic volume of research which is largely untapped, and so I learned as much of this material as I could and used it for my three family members with aggressive cancers, and all three had good outcomes. So I thought, you know what? I should write a book about it so everyone else can receive the benefits of this type of book.
One of the things that I learned early on was that chemotherapy treatments will shrink the tumor temporarily, but the net result is that the tumor recurs with a much more aggressive cell type. And the reason for that is that chemotherapy causes a tremendous increase in inflammation, which can be measured with the Cytokine IL-6. This is the one most commonly measured. The inflammatory master controller is the nuclear factor kappa B pathway which is massively upregulated by chemotherapy. The net result of chemotherapy is that in most cases, it makes the cancer worse. After a brief remission, the cancer becomes drug-resistant and much more aggressive, and spreads and becomes metastatic.
Su, Jin-xuan, et al. “Chemotherapy-induced metastasis: molecular mechanisms and clinical therapies.” Acta Pharmacologica Sinica 44.9 (2023): 1725-1736.
Vyas, Dinesh, Gieric Laput, and Arpitak K. Vyas. “Chemotherapy-enhanced inflammation may lead to the failure of therapy and metastasis.” OncoTargets and therapy (2014): 1015-1023.
Karagiannis, George S., John S. Condeelis, and Maja H. Oktay. “Chemotherapy-induced metastasis: molecular mechanisms, clinical manifestations, therapeutic interventions.” Cancer research 79.18 (2019): 4567-4576.
I consider chemotherapy an obsolete technology. The exception is testicular cancer, where the cancer stem cells are sensitive to chemotherapy. And that brings us to the cancer stem cell. What is the reason why cancers recur after chemotherapy? The bottom line is that chemotherapy eradicates the tumor bulk cells, but leaves the cancer stem cells unharmed. The reason for that: the cancer stem cells are hibernating. They are actually dormant, sort of like a hibernating bear in the winter. And they are not actively dividing. So, chemotherapy will target the actively replicating, actively dividing cells in the cancer and also in the human body. And that is the genesis of most of the adverse side effects of chemotherapy. We have rapidly dividing cells in the Gastrointestinal tract, the epithelium will be denuded. Our bone marrow cells are rapidly dividing and so they are also targeted by chemotherapy. Patients receiving chemotherapy will develop anemia and low white count. So the combination of denudation of the epithelial layer of the Gastrointestinal tract from chemotherapy, which causes leaky gut and gram negative endotoxemia (sepsis), you know, that combination, along with leukopenia, a very low white count, that’s a highly fatal combination. You know, septic shock with no white count.
Dr. Karlfeldt: what makes the cancer stem cells get active once the chemotherapy is done?
There are various triggers for cancer cells, for example, lymphoma cells. Lymphomas are known to be dormant. Many of them tend to be slow-growing, which is measured by the KI-67 proliferation marker. Many lymphomas and even breast cancers have a low KI-67.
Dr. Karlfeldt: What triggers them to become more aggressive?
Me: That is a good question. Environmental triggers? One of the triggers is inflammation. Increased inflammation in the body. The vast majority of cancers will become much more aggressive in an inflammatory micro-environment. One of the drawbacks of chemotherapy is that it creates a massively inflammatory microenvironment. The lymphomas, you know, some of them will respond well to chemotherapy and you can have a “cure”, but the aggressive lymphomas will regress and the patient will have a negative PET scan. But then a few months later, the lymphoma comes back with a vengeance, and I believe that’s the inflammatory conditions in the micro-environment created by chemotherapy causing it to come back.
Dr Karlfelt: That makes sense because we know when we have an injury body, lets say hurt knee or something, that triggers an inflammatory response to then signal to stem cells and to other growth factors to get to that location to repair the area. It makes sense that the inflammatory environment in the tumor micro environment, you know, really activates the cancer stem cells to try to heal that damage.
Me: Exactly. That is a good point. So, you know, the other thing perpetuating the chemotherapy paradigm, and it’s amazing how very few people know this, is called the chemotherapy concession. In most of medicine, it is illegal for a doctor to self-refer. For example, when I worked in radiology, I was in a large group, and in our meetings we would talk about how there are laws that prevent us from referring patients to an imaging center that we own. If we own an outpatient imaging center, we can not refer patients to our own center. It is illegal. It’s called the Stark Law. There a number of laws, state and federal, that make it a criminal offense for a doctor to self-refer. These are called anti-kickback laws.
It is illegal for a doctor to receive a kickback. For example, if a refer a patient to a clinic down the street, and ask them for a kickback, you know that patient generates a certain amount of money for that clinic that I refer to, and I ask for a 10 per cent commission, which is commonly done in real estate and other business transactions, but in medicine, that is illegal. And the doctor can go to jail for doing that, receiving a kickback.
A Call to Eliminate ‘Chemotherapy Concession‘ Nick Mulcahy January 02, 2013
Chemotherapy: A financial gain for oncologists Concession Stand by Jenny Thompson
Health Sciences Institute
For some inexplicable reason, the oncologists receive a kickback from the sale of chemotherapy and other oncology drugs. It is called the chemotherapy concession. It has been going on now, going back to the 1960s, 60-70 years. And it is not well known because the mainstream media does not publicize that the oncologists are receiving a kickback. And that is one of the main mechanisms perpetuating an obsolete technology called chemotherapy. It is basically an obsolete technology from the 1950’s.
So I think it should be illegal for oncologists to receive kickbacks. And if you think back, it was common practice for oncologists back 20-30 years ago to do high intensity chemotherapy that would wipe out the bone marrow in women with breast cancer. Because they were receiving a kickback, they wanted to use more and more chemotherapy. The more chemotherapy they used, the more money they would make. So they came up with the idea, well, if we can’t give too much chemotherapy because it wipes out the patient’s bone marrow, and then they die, so let’s do this thing called bone marrow transplantation. We will harvest the bone marrow first, before the patient receives treatment, and then after the bone marrow is totally wiped out and the patient is helpless, they are going to die, they then receive a transfusion of the bone marrow. The patient’s own bone marrow, back into their body , which saves them. And that is the bone marrow transplant for breast cancer. That was done for many years until finally it was studied, it was the subject of 6 randomized controlled trials reported by Dr. Donald Berry in 2011, and they discovered, guess what? Surprise! It has no clinical benefit. And so the whole practice was discredited and they stopped doing it.
Berry, Donald A., et al. “High-dose chemotherapy with autologous hematopoietic stem-cell transplantation in metastatic breast cancer: overview of six randomized trials.” Journal of Clinical Oncology 29.24 (2011): 3224-3231.
Stadtmauer, Edward A., et al. “Conventional-dose chemotherapy compared with high-dose chemotherapy plus autologous hematopoietic stem-cell transplantation for metastatic breast cancer.” New England Journal of Medicine 342.15 (2000): 1069-1076.
You know, you have other problems with conventional oncology. The drug companies decided to invent a recombinant erythropoetin called Procrit and it was approved for kidney failure patients because they would frequently have anemia, and later, was Procrit was approved for the anemia of cancer patients receiving chemotherapy. And the Procrit was given commonly to increase the blood count in chemotherapy patients who had anemia. And they did that for many years until they discovered that the erythropoietin stimulates red cell production, and guess what? Surprise! It also stimulates cancer growth and cancer production, so that was discredited and oncologists stopped using it. They don’t talk about it. It is one of those things that became politically incorrect.
Henke, Michael, et al. “Erythropoietin to treat head and neck cancer patients with anaemia undergoing radiotherapy: randomised, double-blind, placebo-controlled trial.” The Lancet 362.9392 (2003): 1255-1260.
Leyland-Jones, Brian, et al. “Maintaining normal hemoglobin levels with epoetin alfa in mainly nonanemic patients with metastatic breast cancer receiving first-line chemotherapy: a survival study.” Journal of Clinical Oncology 23.25 (2005): 5960-5972.
There is a new drug, granulocyte colony stimulator, GCSF, which stimulates white cell production. And that is still very commonly used in chemotherapy patients because the chemotherapy will wipe out the white cells, and they have leukopenia which is dangerous because they can die of sepsis when the white count is low like that. So they will give them a Neupogen shot, this is the brand name for one of the GCSF drugs which stimulates white cell production.
So the big question is: What is happening to the cancer? If the patient has a leukemia, for example guess what? Leukemias are white cells. And so there a number of studies showing, and you know what, the cancer is probably being stimulated by the Neupogen shot, and they are just willing to accept that in order to avoid the septicemia and septic shock. I think we are going to find over the next few years that this is going to be a real problem because If you ask what will stimulate cancer stem cells and trigger them to grow again? A drug like that, a drug like Neupogen, can do it. That is one of the many problems with conventional oncology. It is really money-oriented, based on a business model. The whole oncology system has got to be 40-60 years behind current cancer research.
Karagiannidis, Ioannis, et al. “G-CSF in tumors: Aggressiveness, tumor microenvironment and immune cell regulation.” Cytokine 142 (2021): 155479.
Morris, K. T., et al. “G-CSF and G-CSFR are highly expressed in human gastric and colon cancers and promote carcinoma cell proliferation and migration.” British journal of cancer 110.5 (2014): 1211-1220.
So you would think that writing a book like this would be difficult. And it was difficult in the sense of learning a new jargon used in the molecular biology of cancer. This is like learning a new language. That was the difficult part. The fun and enjoyable part is we have all of these new cancer treatments that actually do work, and so in the dedication of the book, I made the statement, this book is dedicated to the half a million patients who died last year of cancer and to the half a million patients next year who won’t. And that is where we are at. Using repurposed drugs and understanding the various cancer metabolic pathways, it is now possible to cure cancer.
Michael Kärlfelft: What causes cancer? You have metabolic, trophoblastic, parasitic, genetic, what is your opinion?
Me: When it comes to choosing a combination of drugs, right at the top of the list we have the metabolic disturbance in cancer which was described by Otto Warburg in the early 1920’s. He received the Nobel prize for discovering that cancer cells have a different metabolic set up that is called aerobic glycolysis. We have much better molecular biology tools now. We know that the metabolic derangement involves a translocation of Hexokinase from the cytoplasm of the cell to the mitochondria. These little pores on the surface of the mitochondria are called voltage-dependent anion channels you know, VDAC for short. It is easier to pronounce “VDAC”.
The hexokinase enzyme is the first enzyme step in the metabolism of glucose. The hexokinase II is not the normal hexokinase. It is an embryonic form. So the normal hexokinase is replaced with an embryonic form of hexokinase called hexokinase II (HK-II), and that is translocated to the VDAC. It is not supposed to be there.
Chiara, Federica, et al. “Hexokinase II detachment from mitochondria triggers apoptosis through the permeability transition pore independent of voltage-dependent anion channels.” PloS one 3.3 (2008): e1852.
Krasnov, George S., et al. “Targeting VDAC-bound hexokinase II: a promising approach for concomitant anti-cancer therapy.” Expert opinion on therapeutic targets 17.10 (2013): 1221-1233.
It then influences the mitochondria, and one of the things that it does, it immortalizes the cell. Normally, cells that are damaged or metabolically deranged in any way will undergo programmed cell death, which is called apoptosis. Sydney Brenner and two other doctors who discovered apoptosis received the Nobel prize in medicine. Is it that important. So when the Hexokinase II is relocated to the VDAC, that turns off the ability of the cell to undergo apoptosis, which is controlled by the mitochondria. So now the cancer cell is immortal and can not commit apoptosis.
And simply by a maneuver, a drug or some agent that will detach the Hexokinase II from the VDAC, this will restore the ability of the cancer cell to undergo programmed cell death. So, that is a valid anticancer strategy. There are a number of repurposed drugs that can do that, which we highlight in the book, because you know, they are widely available at the corner drug store. Drugs like fenofibrate and itraconazole. Fenofibrate is an old lipid drug, and itraconazole is an old antifungal drug. Both have been in use for decades. Both of those two drugs, and there are others, we highlight those two because they are widely available, and they will separate the hexokinase II from the VDAC.
When we look at the metabolic pathways, we are interested in eradicating the cancer stem cells. The thing about cancer stem cells is that they have metabolic plasticity which means they can shift their major energy pathway. From the three major energy pathways, they will shift back and forth depending on what is available, depending on what nutients are available, depending what kind of drug treatment.
So some stem cells will use the glycolytic pathway preferentially, which is the Warbug effect originally described by Otto Warburg, and that is this massive utilization of glucose, relatively bypassing the mitochondria. The second major pathway is oxidative phosphorylation through the mitochondria, which is much more efficient. So if a cancer stem cell is mostly using oxidative phosphorylation, and is given a drug that blocks oxidative phosphorylation, that cancer stem cell will then switch to the glycolytic pathway in the cytoplasm.
The third major pathway, which is highly active in cancer stem cells, is called autophagy. Autophagy is ignored by conventional oncology. I discovered the importance of autophagy when I was researching an anti-malaria drug called artemisinin which was actually discovered by the Chinese. There was a Chinese doctor by the name of Too You You, and in 2015, she received the Nobel prize in Medicine for discovering artemisinin, an anti-malaria drug, which is now a first-line treatment. It is given intravenously in third-world countries as first-line treatment for malaria. It turns out that artemisinin is also an excellent anti-cancer drug, as many of the anti-parasitic drugs will have a dual purpose and can be used as anti-cancer drugs very effectively.
Liu, Wenxiu, and Yue Liu. “Youyou Tu: significance of winning the 2015 Nobel Prize in Physiology or Medicine.” Cardiovascular diagnosis and therapy 6.1 (2016): 1.
Tambo, Ernest, et al. “Nobel prize for the artemisinin and ivermectin discoveries: a great boost towards elimination of the global infectious diseases of poverty.” Infectious diseases of poverty 4.1 (2015): 58.
So, when I was reading about the artemisinin, I saw many of these studies are done in-vitro. They also have animal models in which cancer cells are injected into mice. Specifically, with the in-vitro cancer cell cultures, when they add the artemisinin, they can observe the cells under the microscope and they will see the lysosomes migrate from the periphery of the cancer cell towards the center, near the nucleus. That is called protective autophagy. Autophagy is really a process involving the lysosomes, the entire lysosomal system.
Yang, Nai-Di, et al. “Artesunate induces cell death in human cancer cells via enhancing lysosomal function and lysosomal degradation of ferritin.” Journal of Biological Chemistry 289.48 (2014): 33425-33441.
Jerabkova-Roda, Katerina, et al. “Peripheral positioning of lysosomes supports melanoma aggressiveness.” Nature Communications 16.1 (2025): 3375.
Cabukusta, Birol, and Jacques Neefjes. “Mechanisms of lysosomal positioning and movement.” Traffic 19.10 (2018): 761-769.
Lysosomes are the little bags of digestive enzymes and acid. These are acidified little bags that digest old, unwanted proteins and unwanted organelles. Lysosomes are also involved in other processes, for example, Macropinocytosis, which is shared by single-celled organisms like the amoeba. Everybody remembers biology class when they showed you a movie of an amoeba under the microscope, and it looks like “the blob” and it slides around and engulfs its food. You know, it sends out these pods which engulf the food, and then it brings it into the cell and digests it. That is using autophagy of the lysosome system. So, our cells do the same thing.
Tejeda-Muñoz, Nydia, et al. “Wnt canonical pathway activates macropinocytosis and lysosomal degradation of extracellular proteins.” Proceedings of the National Academy of Sciences 116.21 (2019): 10402-10411.
When the cancer cell is dormant, the lysosomes in this entire autophagy system migrate centrally in the perinuclear area where they hibernate. When the cancer cell becomes aggressive, meaning metastatic potential, the lysosomes will then migrate towards the cell membrane, where they can release acid and digestive enzymes into the microenvironment and actually digest the proteins and tissues surrounding the cancer and obtain nutrition that way, just like other organisms and parasites would do. So autophagy pathways are used by the cancer cells, and to eradicate cancer stem cells, we use an autophagy inhibitor.
It turns out that we have a lot of autophagy inhibitor drugs at the corner drug store. For example, some of the antihistamines such as loratidine which accumulates in the lysosomes and inhibits lysosomal function. We also have proton pump inhibitors, antacids like omeprazole which turn off the acid production in the lysosomes. The lysosomes have an ATP-ase pump, this is a molecular machine that makes the acid. The proton pump inhibitor drugs inhibit these ATP-ase pumps. The lysosomes can not make acid and they become dysfunctional.
Some cancers such as leukemias, have unusually large lysosomes, and they are much more sensitive to autophagy inhibitors that cause the lysosomes to become dysfunctional. And that is one of the main mechanisms for artemisinin which accumulates in the lysosomes of the cancer cell which have a very high iron content, a major difference compared to normal cells.
Cancer cells tend to accumulate iron in the lysosomes. The artemisinin has this “peroxide bridge” which is an oxygen molecule “sticking off” the larger artemesinin molecule, ready to react with pretty much anything. So the oxygen will react with the iron in the lysosomes and create ROS, reactive oxygen species, which then cause the lysosomes to burst, releasing its contents, all that acid and “goop” into the cytoplasm, which kills the cancer cell.
Dr. Karlfeldt: What about safety?
Me: Artemisinin (Artusenate) is extremely safe with low incidence of serious adverse effects. Everything is a matter of dosage and iron content. Normal cells do not have the same iron content as cancer cells. That is the main differential feature that protects normal cells. You can reach a toxic dose if you give enough artusenate, obviously. For treatment of malaria patients with IV artusenate, standard dosage is 2.4 mg/kg per dose, administered intravenously at 0 hours, 12 hours, and 24 hours, then once daily thereafter. This is considered very safe.
Some of the other autophagy inhibitors do have more pronounced, more worrisome adverse side effects. For example. there is a whole class of autophagy inhibitor anti-malarial drugs, mefloquine, chloroquine and hydroxychloroquine, all related, and originally from quinine from the cinchona tree. The safest of the three is hydroxychloroquine. The most effective and yet the one with the most adverse side effects is mefloquine which accumulates in the lysosomes and disrupts lysosomal function. It is highly effective and an excellent cancer stem cell agent, an anticancer drug, and also very good anti-malaria drug. The problem is it causes neuropsychiatric disturbances, and brain degeneration in animal studies.
With many of these anticancer drugs, you have to be careful of adverse side effects, especially with the OXPhos inhibitors, oxidative phosphoylation inhibitors tend to be mitochondrial toxins. maybe one agent is fairly safe, like metformin targets Complex One of the Electron Transport Chain.
There are millions of people taking metformin. They do okay with it. But if you add another mitochondrial agent, you know another, or a third, or a fourth, then you start to get more adverse side effects from mitochondrial toxicity.
For example, if you add a statin drug, which is also a mitochondrial toxin. If a statin is added to metformin or another oxphos inhibitor, for example, niclosamide is a mitochondrial uncoupling agent, another antiparasitic drug, commonly used for tapeworm. Niclosamide is a very good anticancer agent because it is both an OXPHOS inhibitor and Autophagy inhibitor. You can add a Glycolysis inhibitor to Niclosamide and you are now blocking all three major pathways, OXPHOS, Glycolysis and Autophagy.
So the idea is to get synthetic lethality, which means you are preventing metabolic plasticity, you are preventing the cancer cell from shifting to a different metabolic pathway, and preventing the cancer cell from defeating the drug cocktail. So, you have to block all three metabolic pathways, OXPHOS, Glycolysis (Warburg Effect) and Autophagy.
The last third of the book is devoted to Inflammation and Immune Evasion.
The cancer cells will hijack the immune system. They make themselves invisible to the immune system. And a lot of treatments are involved in restoring immune surveillance.
The inflammatory pathways are hijacked by cancer cells, and they use that to make themselves more aggressive. We have anti-inflammatory drugs such as celecoxib (Celebrex) and other NSAIDS. Those studies have been done and published showing that if you give Celebrex along with chemotherapy, it downregulates the inflammatory cytokines produced by the chemotherapy, and the patients have better outcomes.
Ye, Shi-Yu, et al. “The efficacy and safety of celecoxib in addition to standard cancer therapy: a systematic review and meta-analysis of randomized controlled trials.” Current Oncology 29.9 (2022): 6137-6153.
The Mouse That Defeated Cancer
Getting back to the immune system, I was intrigued by a research project at Wake Forest Medical School in Winston Salem. They had medical students injecting mice
with cancer cells. This went on for months and months. All the mice died! And then, out of the blue one day, the medical student held up the mouse. This one mouse did not die and was still alive after a cancer injection. They named the mouse the SR/CR mouse, spontaneous regression, complete remission mouse. And they were very excited about finding this mouse that could defeat cancer. And so they did further studies. They asked the question: What if we transfer the SR/CR mouse’s immune system, the T cells, to a normal wild-type mouse? Would that confer protection? Sure enough, they were protected, and that was the beginning of immunotherapy. They were able to transfer the immune system of a cancer resistant (SR/CR) mouse and confer this resistance to a second mouse.
Hicks, Amy M., et al. “Transferable anticancer innate immunity in spontaneous regression/complete resistance mice.” Proceedings of the National Academy of Sciences 103.20 (2006): 7753-7758.
Koch, Janne, et al. “Immune cells from SR/CR mice induce the regression of established tumors in BALB/c and C57BL/6 mice.” PloS one 8.3 (2013): e59995.
Coley’s Toxins
The doctor who really pioneered immunotherapy in the early 1900’s was an orthopedic surgeon in New York City by the name of William Coley. In those days, they didn’t have much to offer. The big cancer of the bone was osteosarcoma, and it still is. Dr. Coley did 100 amputations for osteosarcoma. One of the patients was a young female patient with an osteosarcoma of the hand. Dr Coley did an amputation of the hand, and the patient died a few months later of metastatic disease. He was so distraught that he reviewed the last 100 cases he operated on. There was only one survivor. And he noticed in the chart that this survivor had a postoperative strep infection. And so he speculated that
the bacterial infection must have stimulated the immune system, and that’s what made the difference in that one surviving patient. So, he came up with a concoction of bacterial toxins. It was dubbed Coley’s Toxins, named after him, and he would inject these toxins into the cancer patients. Not everybody, of course, had remissions, but there were many remarkable remissions that he published in the medical literature of his day. And of course, when chemotherapy was invented, that is when the FDA closed down Coley’s toxins.
Coley was one of the pioneers and now, current day immunotherapy is done with checkpoint inhibitors. The problem with checkpoint inhibitors is they don’t work on everybody. If they do work, patients develop drug resistance fairly quickly. There was a mad rush to find out how to make the checkpoint inhibitors work better. The discovery was made, guess what? it is the microbiome. You know, the friendly bacteria in the gut that make the immunotherapy work. And how did they discover that?
The Year of the Microbiome
It is very, very common for chemotherapy patients to develop sepsis because of the low white count and the leaky gut. And so it is very common for them to receive antibiotics. So they looked back and saw that in the patients who received antibiotics that wiped out the microbiome, they did not do well with the checkpoint inhibitors. So they did further studies and sure enough, there are certain bacterial strains in the microbiome that make the checkpoint immunotherapy work. That was discovered in 2017, the year of the microbiome.
Cimetidine
Another surprising discovery that was made in the 1980’s or early 1990’s regarding immunotherapy was that there were case reports of gastric lymphoma cases. They would do upper endoscopy and see a big ulcerated mass in the stomach. Biopsy shows lymphoma. They couldn’t operate right away because the patient had a huge ulcer, so they would treat the patient with an antacid drug for 6 weeks and then operate. In those days, the anti-ulcer drug was Tagamet, the brand name for cimetidine, which is actually an antihistamine-type drug and an anti-acid. Since then, Cimetidine has been replaced by the newer PPI drugs. Cimetidine is still available over the counter at the corner drug store. They noticed in these two cases where the patients were treated for six weeks with Cimetidine, they go in to do the operation and they find the ulcer is gone, and rebiopsy shows the lymphoma is totally GONE! So they realized that the Cimetidine cured the lymphoma cancer.
Sure enough when you do the pre-clinical studies, Cimetidine upregulates the immune system, a valid anticancer strategy. In addition, Cimetidine upregulation of the immune system can be used for anti-viral treatment.
Cimetidine for Cutaneous Warts
For example, there was a series published on the medical literature on 8 children who received a heart transplant for whatever reason. 7 out of the 8 had complete resolution of recalcitrant cutaneous warts on cimetidine. They give immunosuppressive drugs to prevent rejection. And because they are immunosuppressed, the children are prone to re-activated viral disease that can go rampant. The common is a strain of HPV, human papilloma virus which causes warts on the fingers that grow into long protruding growths, warts, on the tips of the fingers. They showed them with photographs in the journal. You cant miss it . It is very obvious. One of the doctors had the bright idea of giving Cimetidine to the children with the viral warts, and 7 of the 8 children cleared up with cimetidine because of upregulation of the immune system. That gives you an idea of what an over-the-counter repurposed drug can do to boost the immune system. Used along with other repurposed drugs as a complete program, everything is additive, and it does help.
references:
Das, Bibhuti B., et al. “Cimetidine: a safe treatment option for cutaneous warts in pediatric heart transplant recipients.” Medical Sciences 6.2 (2018): 30.
Tan, Sien Hui, et al. “Cimetidine for recurrent respiratory papillomatosis in pregnancy as an alternative adjuvant treatment.” European Archives of Oto-Rhino-Laryngology 281.2 (2024): 1053-1055.
Levy, D. W., A. K. Banerjee, and Helen P. Glenny. “Cimetidine in the treatment of herpes zoster.” Journal of the Royal College of Physicians of London 19.2 (1985): 96.
Beta Glucans / AHCC
The other available immune stimulator, widely available over the counter, is called beta-glucan at the health food store. It is a long chain sugar-like molecule found in cereals, certain mushrooms, yeast and other foods. These have a molecular pattern which mimic pathogenic patterns, pathogenic pattern mimicry. These are called Pathogen-Associated Molecular Patterns (PAMPs) which stimulate the immune system of the patient.
Out of a number of case reports, the one I remember from the book is an elderly man in his late 70’s with metastatc prostate cancer to the bones. The doctors tried everything, every conventional treatment you can imagine, and it is finally refractory to all treatments. His PSA is sky high, like 1100. The patient declines all further treatment and instead takes one of these beta-glucan products. The most popular one is called AHCC, a product from Japan. 6-8 weeks later the PSA has come down dramatically, and he is feeling much better and exercising. That is a dramatic case report of success with upregulating the immune system with a beta glucan type product. That is very impressive.
Wu, Lijuan, et al. “Antitumor effect of soluble β-glucan as an immune stimulant.” International journal of biological macromolecules 179 (2021): 116-124.
Mishra, Vartika, et al. “Beta glucan as an immune stimulant in tumor microenvironment—Insight into lessons and promises from past decade.” International Journal of Biological Macromolecules 234 (2023): 123617.
McFarlin, Brian K., et al. “Discovery of Innate Immune Response mRNAs That Are Impacted by Structure-Specific Oral Baker’s Yeast Beta Glucan Consumption.” BioTech 14.1 (2025): 4.
Stephen Bigelsen, M.D
There a lot of these very impressive case reports in the medical literature. The other one that was very impressive, I thought, was Steven Bigelsen, a doctor at Cornell Medical Center who in 2016, comes down with metastatic pancreatic cancer. And he was a smart guy. He realized that prognosis with chemotherapy was not good, so he researched the medical literature and devised his own program, which was a high dose vitamin D analog called paricalcitol, hydroxychloroquine, intravenous vitamin C, statins, metformin, curcumin, and aspirin. And he is now cancer-free and is still alive. I looked it up. He is still alive, 10 years later! That is a really remarkable story.
Bigelsen, Stephen. “Evidence-based complementary treatment of pancreatic cancer: A review of adjunct therapies including paricalcitol, hydroxychloroquine, intravenous vitamin C, statins, metformin, curcumin, and aspirin.” Cancer management and research (2018): 2003-2018.
There are a couple of cancer survivors who inspired my book. One is Ben Williams who wrote: Surviving Terminal Cancer published in 2002. He was a psychology professor at U of Cal San Diego, close to the border with Mexico. This was before the internet, so he would do his research in the University medical library and then drive across the border into Mexico to buy the repurposed drugs. One of them was Accutane, a vitamin A derivative used for acne. He came up with an entire cocktail of repurposed drugs and he is still alive today after a diagnosis of glioblastoma, a brain tumor which is invariably fatal. His book was one of the inspirations for my book.
Partial List of Repurposed Drugs Used by Ben Williams (from his book) :
Accutane (Isotretinoin) (Vitamin A derivative)
Celebrex (Celecoxib): COX-2 inhibitor, NSAID anti-inflammatory drug.
Fenofibrate: old lipid drug
Chloroquine: An antimalarial drug autophagy inhibitor.
Metformin: Diabetes drug, OxPhos Inhibitor,
Cimetidine: An H2 receptor blocker for ulcers, to upregulate immune response, Melatonin, PSK (a Turkey Tail mushroom extract): β-glucans, standard treatments ( temozolomide, radiation, neurosurgery )
Jane McClellan Starving Cancer
And the other inspiration is Jane McClellan’s book, Starving Cancer. I met Jane McClellan at the Annie Appleseed meeting one year in West Palm Beach, which is not too far from my office in Davie, Florida. So I was able to drive there to the meeting.
Joe Tippens and Fenbendazole
I also met Joe Tippens at the same meeting. They were both there. Joe was a cattle rancher in Oklahoma in 2017 when he came down with small cell lung cancer with extensive metastatic spread. Joe was treated at MD Anderson in Texas with an experimental immunotherapy drug, and sent home with a poor prognosis. Once home, a veterinarian friend told him to try fenbendazole, a veterinary dog dewormer, which he took along with Vitamin E, Curcumin and CBD oil. 3 months later, repeat PET scan at MD Anderson showed he was cancer free, the only one of 1,100 patients in the immunotherapy clinical trial using pembrolizumab (Keytruda) that survived.
Fenbendazole, a veterinary drug, is not approved for human use. The drug is widely available at pet stores, and is similar in molecular structure to mebendazole, which is FDA approved for human use. Both drugs are microtubule inhibitors which is an entire class of anticancer drugs.
Fenbendazole Combined with Ivermectin
Some integrative oncologists are combining Fenbendazole (or mebendazole) with Ivermectin for synergistic effect. Partial list: William Makis MD, Paul Marik MD, Dr. Ilyes Baghli, MD, Jason R. Williams, MD, Pierre Kory, MD, Imran Khan, MD
Those are the inspirations for my book. If these types of approaches are widely adopted, I think we are going to see a huge turnaround in cancer in the country. It is integrative oncologists who are leading the way with that.
Get Your List of Integrative Oncologists
As I said earlier, I don’t treat cancer patients myself in my own practice. I do not treat cancer patients. I don’t see cancer patients regularly. It is not my specialty. And so we have a list of integrative oncologists, which we provide to anyone who calls the office interested in treatment. For any one interested in the list of integrative oncologists, contact me at my contact page for the List. We will be happy to send you our list.
—————————————————————————————-
 Cracking Cancer Toolkit
Cracking Cancer Toolkit
If you liked this article, you might like my book, Cracking Cancer Toolkit, available as a pdf file download for $22.00. The book was published in 2020 on Amazon and had about 100 reviews with a rating of 4.8 out of 5.0 stars. Amazon banned the book in 2025 for “Offensive Content”. Sure, “Offensive” to the chemotherapy industry.
******************* BUY eBOOK HERE *************
Click Here Download eBook pdf file for $22.00
**** FREE Lecture Videos on Cracking Cancer Toolkit *******
Click Here for FREE Cracking Cancer Lecture Video Series for FREE
Articles with related interest:
All Cancer videos and articles by Jeffrey Dach MD
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Bioidentical Hormones 101 Second Edition
Menopausal Hormone Replacement, Health Benefits
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright © 2025 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on September 12th, 2025 by Jeffrey Dach MD
The post The Metabolic Theory of Cancer Explained Podcast Jeffrey Dach and Michael Karlfeldt appeared first on Jeffrey Dach MD.
September 8, 2025
10 Million Women Study: Does HRT Benefit the Elderly?
 10 Million Elderly Women HRT Study: Does HRT Benefit the Elderly? by Jeffrey Dach MD
10 Million Elderly Women HRT Study: Does HRT Benefit the Elderly? by Jeffrey Dach MD
I frequently get this question on HRT for the elderly: What about HRT for women older than 65? Is there a benefit? And what is the risk? Should doctors offer the elderly woman over 65, menopausal hormone replacement (HRT)? Lucky for us, the answer was published in 2024 by Dr. Seo H. Baik in the Journal, Menopause. Dr. Baik examined Medicare records for 10 million senior Medicare women from 2007-2020.
Estrogen Monotherapy After Age 65
The use of estrogen monotherapy after age 65 was compared to never use or discontinued use. Estrogen use was associated with almost 20% risk reduction in mortality. Other risk reductions in percentages were: breast cancer 16%, lung cancer 13%, and colorectal cancer 12% risk reduction. These benefits are seen in women aged 65 to 79 using low-dose transdermal or vaginal estrogen for managing menopausal symptoms like hot flashes and night sweats. (1)
Combined Estrogen/Progestin
The use of estrogen and progestogen combo-therapy exhibited significant risk reductions in endometrial cancer (45%) and ovarian cancer (21%).
So, yes, there is a benefit.
Adverse effects are related to excessive estrogen dosage, which may cause breast tenderness, fullness, or pain. These symptoms are obvious to the patient, who will then take a few days off from the topical hormone product, and once symptoms have resolved, then resume at a lower dosage.
In 2025, Dr. Panagiotis Anagnostis writes:
However, low or ultra-low dose (25 or 12.5 μg of 17β-E2), preferably by the transdermal route, conveys the safest option for postmenopausal women in this age group who have troublesome VMS (vasomotor symptoms), in the absence of contraindications (e.g. history of hormone-sensitive cancer. (2)
Other Benefits of Estrogen
In 2024, Dr. Chengmei Zhang studied the benefits of estrogen in the elderly, finding estrogen has potent neuroprotective properties. Estrogen plays an important bioenergetic role in mitochondrial metabolism in skeletal muscle in prevention of sarcopenia, a form of muscle wasting seen in the elderly. Dr. Zhang writes:
The deficiency of estrogen in menopause has been linked to changes in brain structure, connectivity, energy metabolism. Therewith, these are crucial factors in cognitive function and the risk of Alzheimer’s diseases. Besides, it leads to endocrine and metabolic dysfunction, resulting in osteoporosis, metabolic syndrome, and a tendency toward decreased muscle mass and strength. Estrogen’s influence on mitochondrial function is particularly relevant to aging, as it affects the production of ATP and the overall metabolic health of the brain. Estrogen decline in women skeletal muscle mass is usually related to sarcopenia, a prevalent disease observed in vulnerable elderly individuals. (3)
Conclusion: Yes, there is considerable benefit for the over-65 age group, and my office will provide these women HRT using bioidentical hormone formulas.
 If you liked this article, you might like my new book, Bioidentical Hormones 101 2nd Edition (2025) paperback and ebooks on Amazon.
If you liked this article, you might like my new book, Bioidentical Hormones 101 2nd Edition (2025) paperback and ebooks on Amazon.
Click Here for link to ebook Bioidentical Hormones 101 Second Edition (2025) by Jeffrey Dach MD. This is a Three Volume Series e-book
Paperback Version of Bioidentical Hormones 101 second edition (2025). The p aperback contains all three volumes.
Free Video Introduction to Book:
Introduction Video to Bioidentical Hormones 101 Second Edition (2025)
Bioidentical Hormones for Breast Cancer Survivors Video Presentation
Articles with Related Interest:
Hormone Replacement for Breast Cancer Survivors Part One
Hormone Replacement for Breast Cancer Survivors Part Two
Estrogen Metabolism, Iodine, 2MEO Part Three
Testosterone for Breast Cancer Prevention and Treatment
All Bioidentical Hormone Articles
Header Image: Courtesy of Wikimedia Commons. Portrait of Aline Pasquiou-Quivoron, Mère de l’artiste, 1860, oil on canvas Source/Photographer Artbook – Impressionism and its overlooked Woman 2024. Public Domain.
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Bioidentical Hormones 101 Second Edition
Menopausal Hormone Replacement, Health Benefits
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
References:
1) Baik, Seo H., Fitsum Baye, and Clement J. McDonald. “Use of menopausal hormone therapy beyond age 65 years and its effects on women’s health outcomes by types, routes, and doses.” Menopause (2024): 10-1097.
Objectives: The study aims to assess the use of menopausal hormone therapy beyond age 65 years and its health implications by types of estrogen/progestogen, routes of administration, and dose strengths.
Methods: Using prescription drug and encounter records of 10 million senior Medicare women from 2007-2020 and Cox regression analyses adjusted for time-varying characteristics of the women, we examined the effects of different preparations of menopausal hormone therapy on all-cause mortality, five cancers, six cardiovascular diseases, and dementia.
Results: Compared with never use or discontinuation of menopausal hormone therapy after age 65 years, the use of estrogen monotherapy beyond age 65 years was associated with significant risk reductions in mortality (19% or adjusted hazards ratio, 0.81; 95% CI, 0.79-0.82), breast cancer (16%), lung cancer (13%), colorectal cancer (12%), congestive heart failure (CHF) (5%), venous thromboembolism (3%), atrial fibrillation (4%), acute myocardial infarction (11%), and dementia (2%). For the use of estrogen and progestogen combo-therapy, both E+ progestin and E+ progesterone were associated with increased risk of breast cancer by 10%-19%, but such risk can be mitigated using low dose of transdermal or vaginal E+ progestin. Moreover, E+ progestin exhibited significant risk reductions in endometrial cancer (45% or adjusted hazards ratio, 0.55; 95% CI, 0.50-0.60), ovarian cancer (21%), ischemic heart disease (5%), CHF (5%), and venous thromboembolism (5%), whereas E+ progesterone exhibited risk reduction only in CHF (4%).
Conclusions: Among senior Medicare women, the implications of menopausal hormone therapy use beyond age 65 years vary by types, routes, and strengths. In general, risk reductions appear to be greater with low rather than medium or high doses, vaginal or transdermal rather than oral preparations, and with E2 rather than conjugated estrogen.
A recent study analyzing data from 10 million senior Medicare women between 2007 and 2020 found that hormone therapy (HT) use beyond age 65 may be safe and even beneficial for managing menopause symptoms like hot flashes. The study suggests that age alone should not be a reason to discontinue HT, but that the type, route, and dose of therapy matter. It also found that estrogen monotherapy beyond age 65 was associated with reduced mortality and other health benefits.
2) Anagnostis, Panagiotis, et al. “Can menopausal hormone therapy be considered in postmenopausal women who are older than 60 years?.” Gynecological Endocrinology 41.1 (2025): 2468957.
However, low or ultra-low dose (25 or 12.5 μg of 17β-E2), preferably by the transdermal route, conveys the safest option for postmenopausal women in this age group who have
troublesome VMS, in the absence of contraindications (e.g. history of hormone-sensitive cancer.
3) Zhang, Chengmei, et al. “Research progress on the correlation between estrogen and estrogen receptor on postmenopausal sarcopenia.” Frontiers in endocrinology 15 (2024): 1494972.
Estrogen is a necessary sex steroid and potent neuroprotective hormone. It plays a multifaceted role beyond the reproductive system, extending its influence to the brain, skeletal muscle, and other organs. Estrogen’s role in cognition, mood, autonomic regulation, and neuroprotection involves interactions with neurotransmitters, neuromodulators in a distributed manner. Notably, the
impact of estrogen on mitochondrial metabolism in skeletal muscle is particularly significant due to a unique modulated bioenergetic profiles, synaptic plasticity, and neuronal health. The deficiency of estrogen in menopause has been linked to changes in brain structure, connectivity, energy
metabolism. Therewith, these are crucial factors in cognitive function and the risk of Alzheimer’s diseases. Besides, it leads to endocrine and metabolic dysfunction, resulting in osteoporosis, metabolic syndrome, and a tendency toward decreased muscle mass and strength. Estrogen’s influence on mitochondrial function is particularly relevant to aging, as it affects the production of ATP and the overall metabolic health of the brain. Estrogen decline in women skeletal muscle mass is usually related to sarcopenia, a prevalent disease observed in vulnerable elderly individuals. Therefore, estrogen is considered to play a crucial role in skeletal muscle homeostasis and motor ability, although the exact mechanism remains unclear. This paper reviews the literature on the impact of estrogen on postmenopausal skeletal muscle diseases and the underlying molecular mechanisms, especially in terms of mitochondrial metabolism. In summary, estrogen plays an important role in the health of skeletal muscle in postmenopausal women, and its impact on mitochondrial function and homeostasis offers potential targets for the development of new strategies to treat sarcopenia
===============================
Published on September 8th, 2025 by Jeffrey Dach MD
The post 10 Million Women Study: Does HRT Benefit the Elderly? appeared first on Jeffrey Dach MD.
September 4, 2025
Keeping Abreast with Jenn Simmons and Jeffrey Dach Podcast
 Keeping Abreast, Dr. Jenn Simmons Welcomes Dr. Jeffrey Dach Podcast
Keeping Abreast, Dr. Jenn Simmons Welcomes Dr. Jeffrey Dach Podcast
In this thought-provoking episode of Keeping Abreast, Dr. Jenn Simmons welcomes Dr. Jeffrey Dach for a powerful discussion on bioidentical hormones, estrogen, and the myths that have shaped women’s health for decades. Dr. Dach draws from over 40 years of clinical experience and research to challenge the mainstream narrative that estrogen causes breast cancer. Together, he and Dr. Jenn explore how estrogen protects DNA integrity, why natural progesterone is vastly different from synthetic progestins, and how iodine and testosterone play overlooked but vital roles in breast cancer prevention. Along the way, they trace the history of hormone therapies—from DES and Tamoxifen to modern-day aromatase inhibitors—revealing both the progress and the persistent dogmas of conventional medicine. This is a conversation about evidence, empowerment, and the urgent need to rethink how we approach women’s health. Because of its depth and importance, this conversation has been divided into two parts.
This episode is Part 1 of 2. In This Episode, You Will Learn:
Why estrogen may protect against breast cancer rather than cause it.
The truth about estrogen receptors and how they shape cancer risk.
The critical difference between natural progesterone and synthetic progestins How testosterone supports breast cancer prevention.
Why iodine deficiency remains a hidden driver of disease.
The historical evolution of hormone therapies—from DES to Tamoxifen How entrenched medical dogmas persist despite new evidence.
107: Estrogen Myths & Bioidentical Truths with Jeffrey Dach, MD (Part 1)
======================================================================
108: Estrogen Myths & Bioidentical Truths with Jeffrey Dach, MD (Part 2)
In the conclusion of this two-part conversation, Dr. Jenn Simmons and Dr. Jeffrey Dach go deeper on bioidentical hormones, long-term estrogen deprivation (LTED), and why “have” vs. “had” breast cancer matters when discussing HRT. They examine apoptosis after LTED, the role of estrogen in genomic stability, and how overdiagnosis from screening can drive unnecessary treatment. They also cover practical prevention pillars—iodine, DIM, selenium, and vitamin D—and what thoughtful, individualized care can look like for women navigating menopause and survivorship.
In This Episode, You Will Learn:
How reintroducing estrogen can trigger apoptosis in specific contexts.
Why “have” vs. “had” breast cancer changes the HRT conversation.
How screening, overdiagnosis, and rising mastectomy rates intersect.
The difference between natural progesterone and synthetic progestins.
How iodine, DIM, selenium, and vitamin D factor into prevention programs.
What estrogen metabolites (2-hydroxy vs 4-hydroxy) and COMT mean for risk.
Where integrative oncology and repurposed therapies fit into patient-centered care.
======================================================================
Click Here for the link to my ebook on Amazon: ebook Bioidentical Hormones 101 Second Edition (2025) by Jeffrey Dach MD. This is a Three Volume Series e-book.
Click Here for Paperback Version of Bioidentical Hormones 101 second edition (2025). The paperback contains all three volumes.
======================================================================
 About Dr. Jennifer Simmons, MD, FACS
About Dr. Jennifer Simmons, MD, FACS
Breast Surgeon, Chief of Breast Surgery and Director of the Breast Program at the Einstein Medical Center and Director of the Breast Program at Aria Health.
M.D. from Jefferson Medical College at Thomas Jefferson University
Dr. Jennifer Simmons is a breast surgeon, integrative oncologist, author, podcast host, Summit Host, and founder of Perfeqtion Imaging.
Dr. Jenn Simmons started her professional career as Philadelphia’s first fellowship trained breast surgeon and spent 17 years as Philadelphia’s top breast surgeon. Her own illness led her to discover functional medicine. Dr. Jenn left traditional medicine in 2019 and founded Real Health MD to help women along their breast cancer journey truly heal.
In 2017, Dr. Jenn experienced her own serious health crisis with chronic fatigue and became a patient of the mainstream medical system. Rejecting the harsh treatments of conventional medicine, Dr Jenn turned to functional medicine approaches, leading to complete recovery. After her recovery, Dr. Simmons transitioned from surgical oncology to functional medicine, with a special emphasis on prevention and treatment of breast cancer. In 2019, Dr. Simmons founded Real Health MD, a virtual medical oncology practice supporting women at any stage of the breast cancer journey—from prevention and diagnosis to post-treatment recovery. Dr. Simmons hosted the Breast Cancer Breakthroughs Summit and is the founder of PerfeQTion Imaging, an innovative breast ultrasound technique that creates high-resolution 3D images of the breast as an alternative to screening mammography.
Education and Training
Medical Degree (MD): Jefferson Medical College (now Sidney Kimmel Medical College at Thomas Jefferson University), Philadelphia, PA (graduation circa 1998–2000).
Residency: General Surgery, Albany Medical Center (Albany Med), Albany, NY (completed circa 2000–2003).
Fellowship: Breast Disease/Breast Surgery, Thomas Jefferson University Hospital/Breast Health Institute, Philadelphia, PA (2003–2004; first such fellowship in Philadelphia).
Certification in Functional Medicine: Institute for Functional Medicine (IFM), completed 2019.
Board Certifications
Board-Certified in General Surgery (American Board of Surgery).
Specialization in Breast Surgery.
Professional Experience and Positions
2004–2019: Breast Surgeon, Einstein Medical Center Montgomery, Norristown, PA.
Chief of Breast Surgery.
Director of the Breast Program.
Medical Director of the Cancer Program.
2019–Present: Founder and Lead Practitioner, Real Health MD (virtual integrative oncology practice).
2020–Present: Founder, PerfeQTion Imaging (breast screening centers using QT technology).
Affiliations: Geisinger Bloomsburg Hospital (PA); MercyOne Cedar Falls Medical Center (IA); former roles at UCLA and other centers (not primary).
Publications and Authorship
The Smart Woman’s Guide to Breast Cancer: The Functional Medicine Approach That Will Free You From Your Diagnosis (2024, independently published; international bestseller on Amazon). Covers personalized prevention, treatment, recovery, genetics, inflammation, diet, and toxins.
Recipes for Real Health (date not specified; cookbook tied to her programs).
Awards and Honors
Founders Award, Living Beyond Breast Cancer (2016)
“Top Doc,” Philadelphia Magazine (6 years consecutive, up to ~2018).
“Top Doc,” Main Line Today (2018) and Suburban Life.
Speaking and Media
Podcast Host: Keeping Abreast with Dr. Jenn podcast (2023–present; 100+ episodes).
Summit Host: Breast Cancer Breakthroughs Summit (3x, latest 2024).
Guest Appearances: Wellness Mama (2024), Rupa Health (2024), Integrative Women’s Health Institute (2024), and more.
Dr. Jenn is a devoted wife, mother, stepmother, grandmother, and athlete. Her life’s mission is deeply personal, rooted in her cousin’s memory, and driven by a desire to make a lasting impact on all those who desire breast health. As she famously says, “Breast Health is Health!”
Connect with Dr. Jenn Simmons at her Website
==========================================================================
Click Here for link to books on Amazon:
ebook Bioidentical Hormones 101 Second Edition (2025) by Jeffrey Dach MD. This is a Three Volume Series e-book
Paperback Version of Bioidentical Hormones 101 second edition (2025). The p aperback contains all three volumes.
Free Video Introduction to Book:
Introduction Video to Bioidentical Hormones 101 Second Edition (2025)
Bioidentical Hormones for Breast Cancer Survivors Video Presentation
Articles with Related Interest:
Hormone Replacement for Breast Cancer Survivors Part One
Hormone Replacement for Breast Cancer Survivors Part Two
Estrogen Metabolism, Iodine, 2MEO Part Three
Testosterone for Breast Cancer Prevention and Treatment
All Bioidentical Hormone Articles
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Bioidentical Hormones 101 Second Edition
Menopausal Hormone Replacement, Health Benefits
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Copyright © 2025 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on September 4th, 2025 by Jeffrey Dach MD
The post Keeping Abreast with Jenn Simmons and Jeffrey Dach Podcast appeared first on Jeffrey Dach MD.
August 27, 2025
Jeffrey Dach MD Podcast Estrogen is Cancer Preventative
 Jeffrey Dach MD Podcast Estrogen is Cancer Preventative
Jeffrey Dach MD Podcast Estrogen is Cancer Preventative
Many thanks to Corinne Furnari and Carol Petersen for inviting me onto their podcast show to discuss my new book, Bioidentical Hormones 101 second edition (2025) available on Amazon.
===================================
==================================
 Corinne Furnari, PA CCN
Corinne Furnari, PA CCN
62 S. Phillips Ave. PO 147
Remsenburg, New York, 11960
Text 646-734-9437
Take Charge of Your Health
Facebook: Corinne Furnari RPA CCN
Website: Furnarihealth.com
corinnehealth.com
Ms. Furnari has been practicing integrative medicine in private and group practice for approximately twenty-five years. She is a Certified Clinical Nutritionist, part of the first group of clinicians to be certified as a clinical nutritionist in New York State. A licensed Physician’s Assistant, she is a graduate of USC Physician’s Assistant Program, qualifying with honors on her national boards in general medicine and surgery. She is a Certified Nutrition Specialist qualified and Board Certified by the International Society of Cosmetology in Office-Based Medical Cosmetic Procedures.
============================================
 Carol Petersen, RPh, CNP
Carol Petersen, RPh, CNP
The Wellness by Design Project
Madison, Wisconsin
Phone: 608-469-8821
ca***@************************ct.com
With her Wellness by Design Project, Carol provides Bioidentical Hormone Consultation and Coaching Support. You are invited to join her to explore aging gently with vitality and exuberance at The Wellness by Design Project. Carol Petersen is an accomplished compounding pharmacist with decades of experience helping patients improve their quality of life through bio-identical hormone replacement therapy. She graduated from the University of Wisconsin School of Pharmacy and is a Certified Nutritional Practitioner. Her passion for optimizing health and commitment to compounding is evident in her involvement with organizations including the International College of Integrated Medicine and the American College of Apothecaries, the American Pharmacists Association, and the Alliance for Pharmacy Compounding She was also the founder and first chair of the Compounding Special Interest Group with the American Pharmacists Association. She is the chair of the Integrated Medicine Consortium. She co-hosts a radio program “Take Charge of Your Health” in the greater New York area. She is on the Medical Advisory Board for the Centre for Menstrual Cycle and Ovulation Research (CeMCOR.ca)
=======================================================
 Click Here for link to books on Amazon:
Click Here for link to books on Amazon:
ebook Bioidentical Hormones 101 Second Edition (2025) by Jeffrey Dach MD. This is a Three Volume Series e-book
Paperback Version of Bioidentical Hormones 101 second edition (2025). The p aperback contains all three volumes.
Free Video Introduction to Book:
Introduction Video to Bioidentical Hormones 101 Second Edition (2025)
Bioidentical Hormones for Breast Cancer Survivors Video Presentation
Articles with Related Interest:
Hormone Replacement for Breast Cancer Survivors Part One
Hormone Replacement for Breast Cancer Survivors Part Two
Estrogen Metabolism, Iodine, 2MEO Part Three
Testosterone for Breast Cancer Prevention and Treatment
All Bioidentical Hormone Articles
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Bioidentical Hormones 101 Second Edition
Menopausal Hormone Replacement, Health Benefits
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright © 2025 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on August 27th, 2025 by Jeffrey Dach MD
The post Jeffrey Dach MD Podcast Estrogen is Cancer Preventative appeared first on Jeffrey Dach MD.
August 25, 2025
Cracking Cancer Toolkit Banned From Amazon
Cracking Cancer Toolkit Banned From Amazon
by Jeffrey Dach MD
Don’t worry! You can download your copy here.
After 5 years on Amazon, they banned the book for “Offensive Content”.
Sure, Offensive to the Chemotherapy Industry.
*******************Still Under Construction *************
Book Download will be ready in about a week or two. Thank you for your patience. Sorry for the inconvenience.
*************************************************************************************************************
In the meantime, check out this free video series introduction to the book:
***************** FREE ***********************
Cracking Cancer Lecture Video Series for FREE
***************** FREE ***********************
Published on August 25th, 2025 by Jeffrey Dach MD
The post Cracking Cancer Toolkit Banned From Amazon appeared first on Jeffrey Dach MD.
August 20, 2025
Does the C0\/1D \/axxine Cause Cancer?
 Does the C0\/1D \/a<
Does the C0\/1D \/a<
I was quite surprised last week to find a one-line Google Review of my medical practice by a person who is not a patient in my office —a young mother from Topeka, Kansas, with no basic knowledge of medicine or molecular biology. Here is the Review, which was deleted by Google a few days later and is no longer visible on the Internet:
Sharing with your patients that the C9\/1D \/a<
As it turns out there are at least 100 studies in the medical literature suggesting seventeen mechanisms for carcinogenicity for the C0\/1D \/a<
Does the C0\/1D \/a<
Thanks and credit goes to Nicolas Hulscher, MPH for his article on this question, and to Mathilde Debord who did a comprehensive literature review on mechanisms the mRNA injections may induce, accelerate, or reactivate cancer through 17 distinct biologic mechanisms.
17 Biological Mechanisms which may Initiate, Accelerate, or Reactivate Malignant Processes taken from 100 Peer-Reviewed Studies:
1. Genome Instability
mRNA may be reverse-transcribed and integrated into host DNA, triggering mutations that initiate cancer.
2. Immune Escape
The spike protein binds and inhibits tumor suppressor genes like p53 and BRCA1, shielding cancer cells from immune destruction.
3. Impaired DNA Repair Mechanism
The spike protein interferes with essential DNA repair enzymes, increasing the risk of unchecked mutations.
4. Chronic Inflammation
Lipid nanoparticles and spike protein cause long-lasting inflammation, a well-known driver of cancer.
5. Dysregulation of the Immune System
Suppression of T cells and type I interferon weakens cancer surveillance and promotes immune evasion.
6. RNA Disruption
Codon optimization disrupts microRNA networks, destabilizing cell growth regulation and apoptosis.
7. Activation of Oncogenic Pathways
The spike protein indirectly activates MAPK and PI3K/mTOR signaling, fueling tumor growth and metastasis.
8. Tumor Microenvironment Alteration
Lipid nanoparticles accumulate in tumors, enhancing permeability and potentially accelerating cancer spread.
9. Awakening Dormant Cancers
Post-vaccination inflammation and immune disruption may trigger recurrence in patients previously in remission.
10. Alteration of Immune Surveillance
Modified mRNA blocks toll-like receptors, making tumor cells “invisible” to the immune system.
11. Frameshift Errors
The synthetic mRNA sometimes produces unintended, aberrant proteins, contributing to oncogenic risk.
12. Multiple Injections
Repeated doses exhaust the immune system and drive class switching to IgG4, promoting tolerance to tumors.
13. DNA Contamination
Residual plasmid DNA found in vaccine vials is replication-competent and could integrate into host genomes.
14. Oncogenic SV40 DNA Sequences
SV40 promoter sequences in Pfizer vials may facilitate genome insertion—this same element is used to induce tumors in lab animals.
15. Deregulation of the Renin-Angiotensin System (RAS)
Spike-induced AT1R activation fosters oxidative stress and uncontrolled cell proliferation.
16. Destruction of the Microbiota
The injections deplete bifidobacteria, weakening immune balance and impairing anti-cancer responses.
17. Increased Resistance to Treatments
Spike exposure prolongs cancer cell survival during chemotherapy, possibly driving treatment resistance.
References for 17 Mechanisms for Carcinogenicity:
17 Ways mRNA Shots May Cause Cancer, According to Over 100 Studies Nicolas Hulscher, MPH Jun 24, 2025
Les vaccins ARNm anti-COVID peuvent induire le cancer de 17 manières distinctes selon plus de 100 études Mathilde Debord | 19 juin 2025
First Peer-Reviewed Paper Defines COVID-19 Vaccine-Induced “Turbo Cancer”
For the first time, “turbo cancers” move from censorship into the peer-reviewed medical literature. Nicolas Hulscher, MPH Aug 19, 2025
What Causes Cancer in General?
On the question of what causes cancer in general, the answer is complicated and involves a review of animal models of breast cancer. Researchers induce breast cancer in mice by injecting them with carcinogenic chemicals such as DMBA. The agency, IARC, has listed 120 environmental chemicals as carcinogenic to humans. A few are: Tobacco Smoke, Alcoholic Beverages, Asbestos, Benzene, Arsenic, Aflatoxins, Formaldehyde, and Polychlorinated Biphenyls (PCBs). The second animal model is the genetically modified mouse which spontaneously develops breast cancer. Likewise, in humans there are genetic abnormalities which increase cancer risk. So, we can look at any substance or chemical and try to assess the cancer risk. However, it is not possible to state with certainty which of the 120 environmental chemicals or other risk factors have definitively caused a person’s cancer. We can only suggest a benefit in reducing exposure to carcinogenic chemicals and substances in the environment.
Are \/a<
A number of researchers such as Dr. Theresa Deisher think so. Dr Deisher says there are problems inherent in using human fetal cell cultures for viral replication in the vaccine manufacturing process. Dr. Deisher says the final product contains human fetal cell DNA contamination causing insertional mutagenesis, a mechanism for carcinogenicity. Other independent laboratories (U.S., Canada, Australia, Germany, France) have confirmed plasmid DNA contamination of certain \/a<
More on Insertional Mutagenesis from Contaminating DNA fragments
The Florida Department of Heath, Surgeon General Dr Joseph Ladapo has advised all citizens in the State of Florida to decline C0\/1D \/a<previous newsletter.
Let’s Ask Grok
I asked Grok, the AI program developed by Elon Musk on Twitter:
Assuming there is DNA contamination, could this cause insertional mutagenesis?
Here is Grok’s Answer:
Yes, if DNA contamination is present in a biological system, such as during gene therapy, \/a<
Here’s a concise explanation: Insertional mutagenesis occurs when foreign DNA integrates into the host genome and disrupts or alters the function of genes at or near the insertion site. This can lead to various outcomes, including activation of oncogenes, inactivation of tumor suppressor genes, or other genetic dysregulation, potentially increasing the risk of diseases like cancer.
If a biological product (e.g., a \/a<. (Grok’s reply in italics, emphasis mine)
Why Is There Excess Cancer Mortality?
Another disturbing finding is the increase in cancer deaths in national data charts. See rising line (red arrow) indicating excess cancer deaths in the chart below:

Above Chart: Cancer Mortality from CDC Data
17 Ways mRNA Shots May Cause Cancer, According to Over 100 Studies
Comprehensive literature review reveals how mRNA injections may induce, accelerate, or reactivate cancer through 17 distinct pathways
1. Genome instability – mRNA may integrate into DNA, causing mutations.… pic.twitter.com/4gq0Zc4Fq9
— Nicolas Hulscher, MPH (@NicHulscher) June 24, 2025
Conclusion: Although we have no long-term studies of carcinogenicity for \/a<
Articles with related Interest:
Florida Dept of Health, Surgeon General, Joseph Ladapo, MD, Advises Against Use of mRNA C0\/lD \/a<
Turbo Cancer: Rapid Progression of Lymphoma After C0\/lD Booster
Lies My Government Told Me about the C0\/lD \/a<
Teresa Deisher Concerns About Insertional Mutagenesis
Header Image: Tumor cells under microscope labeled with fluorescent molecules By Vshivkova, Shutterstock stock photo ID: 173060636 under enhanced license to jeffrey dach md (paid)
References:
17 Ways mRNA Shots May Cause Cancer, According to Over 100 Studies Nicolas Hulscher, MPH Jun 24, 2025
Les vaccins ARNm anti-COVID peuvent induire le cancer de 17 manières distinctes selon plus de 100 études Mathilde Debord | 19 juin 2025
100 Peer Review Studies showing mechanism of carcinogenicity:
[1] Acevedo-Whitehouse K, Bruno R. Potential health risks of mRNA-based vaccine therapy: A hypothesis. Med Hypotheses. 2023 Feb;171:111015. https://doi.org/10.1016/j.mehy.2023.1....
[2] Valdes Angues R, Perea Bustos Y. SARS-CoV-2 Vaccination and the multi-hit hypothesis of oncogenesis Cureus. 2023 Dec 17;15(12):e50703. https://doi.org/10.7759/cureus.50703.
[3] Aldén M, Olofsson Falla F, Yang D, Barghouth M, Luan C, Rasmussen M, et al. Intracellular reverse transcription of Pfizer BioNTech COVID-19 mRNA vaccine BNT162b2 in vitro in human liver cell line. Curr Issues Mol Biol. 2022 Feb 25;44(3):1115-26. https://doi.org/10.3390/cimb44030073.
[4] Chandramouly G, Zhao J, McDevit S, Rusanov T, Hoang T, Borisonnik N, et al. Polθ reverse transcribes RNA and promotes RNA-templated DNA repair. Sci Adv. 2021 Jun 11;7(24):eabf1771. https://doi.org/10.1126/sciadv.abf1771.
[5] Zhang L, Richards A, Barrasa MI, Hughes SH, Young RA, Jaenisch R.. Reverse-transcribed SARS-CoV-2 RNA can integrate into the genome of cultured human cells and can be expressed in patient-derived tissues. PNAS. 2021 May 25;118(21):e2105968118. https://doi.org/10.1073/pnas.2105968118.
[6] Breda L, Papp TE, Triebwasser MP, Yadegari A, Fedorky MT, Tanaka N, et al. In vivo hematopoietic stem cell modification by mRNA delivery. Science. 2023 Jul 28;381(6656):436-443. https://www.doi.org/10.1126/science.a....
[7] Le Dr McKernan a fait cette découverte en analysant la biopsie du cancer du côlon d’une personne ayant reçu quatre injections d’ARNm de Pfizer. Le député et ancien ministre japonais Kazuhiro Haraguchi a déclaré publiquement fin mai que de la protéine Spike vaccinale avait également été retrouvée dans les cellules cancéreuses de son lymphome malin.
[8] https://x.com/tatiann69922625/status/.... Cette découverte a fait l’objet d’une discussion avec l’épidémiologiste Nicolas Hulscher : https://www.thefocalpoints.com/p/brea....
[9] Singh N, Singh AB. S2 Subunit of SARS-nCoV-2 interacts with tumor suppressor protein p53 and BRCA: an in silico study. Transl Oncol. 2020 Oct;13(10):100814. https://doi.org/10.1016/j.tranon.2020.... Les résultats de cette étude ont été publiés le 30 juin 2020.
[10] Chen X, Zhang T, Su W, Dou Z, Zhao D, Jin X, et al. Mutant p53 in cancer: from molecular mechanism to therapeutic modulation. Cell Death Dis. 2022 Nov 18;13(11):974. https://doi.org/10.1038/s41419-022-05....
[11] Selon Valdes Angues et al., « Les cancers associés aux mutations TP53 incluent le cancer du sein, les sarcomes des tissus osseux et mous, les tumeurs cérébrales et les carcinomes corticosurrénaliens. D’autres cancers moins fréquents incluent la leucémie, le cancer de l’estomac et le cancer colorectal. Les cancers associés à une altération de l’activité de BRCA1 comprennent le cancer du sein, de l’utérus et de l’ovaire chez les femmes, le cancer de la prostate et du sein chez les hommes, et une augmentation modeste du cancer du pancréas chez les hommes et les femmes. Les cancers les plus fréquemment rapportés avec des mutations BRCA2 incluent le pancréas, la prostate chez les hommes et le mélanome ».
[12] Jiang H, Mei YF. SARS-CoV-2 spike impairs DNA damage repair and inhibits v(d)j recombination in vitro. Viruses. 2021;13(10):2056. https://doi.org/10.3390/v13102056. Lien vers l’étude en français : https://www-mdpi-com.translate.goog/1....
[13] Zhang S, El-Deiry WS. SARS-CoV-2 Spike protein inhibits tumor suppressor p53 and creates a vulnerability to cancer. bioRxiv (preprint). 2024 Apr 15. https://doi.org/10.1101/2024.04.12.58....
[14] Zhang S, El-Deiry WS. Transfected SARS-CoV-2 spike DNA for mammalian cell expression inhibits p53 activation of p21(WAF1), TRAIL Death Receptor DR5 and MDM2 proteins in cancer cells and increases cancer cell viability after chemotherapy exposure. Oncotarget. 2024 May 3;15:275-284. https://doi.org/10.18632/oncotarget.2....
[15] Seneff S, Nigh G, Kyriakopoulos AM, McCullough PA. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs. Food Chem Toxicol. 2022 Apr 15;164:113008. https://doi.org/10.1016/j.fct.2022.11....
[16] Ambati BK, Varshney A, Lundstrom K, Palú G, Uhal BD, Uversky VN, et al. MSH3 homology and potential recombination link to SARS-CoV-2 furin cleavage site. Front Virol. 2022 Feb;2:834808. https://doi.org/10.3389/fviro.2022.83....
[17] http://genatlas.medecine.univ-paris5.....
[18] Başaran N, Szewczyk-Roszczenko O, Roszczenko P, Vassetzky Y, Sjakste N. Genotoxic risks in patients with COVID-19. Infect Genet Evol. 2025 Apr;129:105728. https://doi.org/10.1016/j.meegid.2025....
[19] Kedmi R, Ben-Arie N, Peer D. The systemic toxicity of positively charged lipid nanoparticles and the role of Toll-like receptor 4 in immune activation. Biomaterials. 2010 Sep;31(26):6867-75. https://doi.org/10.1016/j.biomaterial....
[20] Turni C, Lefringhausen A. Covid-19 vaccines: An Australian review. J. Clin. Exp. Immunol. 2022 Sep 21;7(3):491-508. https://blog.fdik.org/2023-03/covid19....
[21] Ndeupen S, Qin Z, Jacobsen S, Bouteau A, Estanbouli H, Igyártó BZ.The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory. iScience. 2021 Dec 17;24(12):103479. https://doi.org/10.1016/j.isci.2021.1....
[22] Alameh MG, Tombácz I, Bettini E, Lederer K, Sittplangkoon C, Wilmore JR, et al. Lipid nanoparticles enhance the efficacy of mRNA and protein subunit vaccines by inducing robust T follicular helper cell and humoral responses. Immunity. 2021 Dec 14;54(12):2877-2892.e7. https://doi.org/10.1016/j.immuni.2021....
[23] Theoharides TC. Potential association of mast cell activation by the SARS-CoV-2 spike protein with cancer progression. Med Hypoth. 2022;160:110774. https://doi.org/10.1016/j.mehy.2022.1....
[24] Sagala G. Apparent cytotoxicity and intrinsic cytotoxicity of lipid nanomaterials contained in a COVID-19 mRNA Vaccine. IJVTPR. 2023 Oct 16;3(1):957-72. https://doi.org/10.56098/ijvtpr.v3i1.84.
[25] Estep BK, Kuhlmann CJ, Osuka S, Suryavanshi GW, Nagaoka-Kamata Y, Samuel CN, et al. Skewed fate and hematopoiesis of CD34 HSPCs in umbilical cord blood amid the COVID-19 pandemic. iScience. 2022 Dec 22;25(12):105544. https://doi.org/10.1016/j.isci.2022.1....
[26] Jahankhani K, Ahangari F, Adcock IM, Mortaz E. Possible cancer-causing capacity of COVID-19: Is SARS-CoV-2 an oncogenic agent? Biochimie. 2023 May 23;S0300-9084(23)00136-0. https://doi.org/10.1016/j.biochi.2023....
[27] Australian Therapeutic Goods Administration (TGA). Nonclinical evaluation report: BNT162b2 [mRNA] COVID-19 vaccine (COMIRNATYTM). 2021 Jan. p. 45. https://www.tga.gov.au/sites/default/....
[28] Trougakos IP, Terpos E, Alexopoulos H, Politou M, Paraskevis D, et al. COVID-19 mRNA vaccine-induced adverse effects: unwinding the unknowns. Trends Mol Med. 2022 Oct;28(10):800-802. https://doi.org/10.1016/j.molmed.2022....
[29] Parry PI, Lefringhausen A, Turni C, Neil CJ, Cosford R, Hudson NJ, Gillespie J. ‘Spikeopathy’: COVID-19 spike protein is pathogenic, from both virus and vaccine mRNA. Biomedicines. 2023 Aug 17;11(8):2287. https://doi.org/10.3390/biomedicines1....
[30] Posa A. Spike protein-related proteinopathies: A focus on the neurological side of spikeopathies. Ann Anat. 2025 Apr 18;260:152662. https://doi.org/10.1016/j.aanat.2025.....
[31] Petrosin S, Matende N. Elimination/Neutralization of COVID-19 vaccine-produced spike protein: scoping review. Mathews J Nutr Diet. 2024;7(2):1-23. https://doi.org/10.30654/MJND.10034.
[32] Bhattacharjee B, Lu P, Monteiro VS, Tabachnikova A, Wang K, Hooper WB, et al. Immunological and antigenic signatures associated with chronic illnesses after1 COVID-19 vaccination. MedRxiv (preprint). 2025 Feb 25. https://doi.org/10.1101/2025.02.18.25....
[33] Patterson BK, Yogendra R, Francisco EB, Guevara-Coto J, Long E, Pise A, et al. Detection of S1 spike protein in CD16 monocytes up to 245 days in SARS-CoV-2-negative post-COVID-19 vaccine syndrome (PCVS) individuals. Hum Vaccin Immunother. 2025 Dec;21(1):2494934. https://doi.org/10.1080/21645515.2025....
[34] Alghamdi A, Hussain SD, Wani K, Sabico S, Alnaami AM, Amer OE, et al. Altered circulating cytokine profile among mRNA-vaccinated young adults: A year-long follow-up study. Immun Inflamm Dis. 2025 Apr;13(4):e70194. https://doi.org/10.1002/iid3.70194.
[35] Ota N, Itani M, Aoki T, Sakurai A, Fujisawa T, Okada Y, et al. Expression of SARS-CoV-2 spike protein in cerebral Arteries: Implications for hemorrhagic stroke post-mRNA vaccination. J Clin Neurosci. 2025 Jun;136:111223. https://doi.org/10.1016/j.jocn.2025.1....
[36] Valdes Angues R, Perea Bustos Y. SARS-CoV-2 Vaccination and the multi-hit hypothesis of oncogenesis Cureus. 2023 Dec 17;15(12):e50703. https://doi.org/10.7759/cureus.50703.
[37] Rubio-Casillas A, Cowley D, Raszek M, Uversky VN, Redwan EM. Review: N1-methyl-pseudouridine (m1Ψ): Friend or foe of cancer? Int J Biol Macromol. 2024 May;267(Pt 1):131427. https://doi.org/10.1016/j.ijbiomac.20....
[38] Ivanova EN, Shwetar J, Devlin JC, Buus TB, Gray-Gaillard S, Koide A, et al. mRNA COVID-19 vaccine elicits potent adaptive immune response without the acute inflammation of SARS-CoV-2 infection. iScience. 2023 Nov 24;26(12):108572. https://doi.org/10.1016/j.isci.2023.1....
[39] Seneff S, Nigh G, Kyriakopoulos AM, McCullough PA. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs. Food Chem Toxicol. 2022 Apr 15;164:113008. https://doi.org/10.1016/j.fct.2022.11....
[40] Liu J, Wang J, Xu J, Xia H, Wang Y, Zhang C, et al. Comprehensive investigations revealed consistent pathophysiological alterations after vaccination with COVID-19 vaccines. Cell Discov. 2021 Oct 26;7(1):99. https://doi.org/10.1038/s41421-021-00....
[41] Ning W, Xu W, Cong X, Fan H, Gilkeson G, Wu X, et al. COVID-19 mRNA vaccine BNT162b2 induces autoantibodies against type I interferons in a healthy woman. J Autoimmun. 2022 Oct;132:102896. https://doi.org/10.1016/j.jaut.2022.1....
[42] Qin Z, Bouteau A, Herbst C, Igyártó BZ. Pre-exposure to mRNA-LNP inhibits adaptive immune responses and alters innate immune fitness in an inheritable fashion. PLoS Pathog. 2022 Sep 2;18(9):e1010830. https://doi.org/10.1371/journal.ppat.....
[43] Föhse FK, Geckin B, Zoodsma M, Kilic G, Liu Z, Röring RJ, et al. The BNT162b2 mRNA vaccine against SARS-CoV-2 reprograms both adaptive and innate immune responses. Clin Immunol. 2023 Oct;255:109762. https://doi.org/10.1016/j.clim.2023.1....
[44] Abramczyk H, Brozek-Pluska B, Beton K. Decoding COVID-19 mRNA vaccine immunometabolism in central nervous system: human brain normal glial and glioma cells by Raman imaging. Biovrix. 2022 Mar 2. https://doi.org/10.1101/2022.03.02.48....
[45] Sahin U, Muik A, Derhovanessian E, Vogler I, Kranz LM, Vormehr M, et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature. 2020 Oct;586(7830):594-599. https://doi.org/10.1038/s41586-020-28....
[46] Mulligan MJ, Lyke KE, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature. 2020 Oct;586(7830):589-593. https://doi.org/10.1038/s41586-020-26....
[47] Raisch J, Darfeuille-Michaud A, Nguyen HT. Role of microRNAs in the immune system, inflammation and cancer. World J Gastroenterol. 2013 May 28;19(20):2985-96. https://doi.org/10.3748/wjg.v19.i20.2985.
[48] Han Z, Estephan RJ, Wu X. MicroRNA regulation of T-cell exhaustion in cutaneous T cell lymphoma. J Invest Dermatol. 2022 Mar;142(3 Pt A):603-612.e7. https://doi.org/10.1016/j.jid.2021.08....
[49] Mishra R, Banerjea AC. SARS-CoV-2 spike targets USP33-IRF9 axis via exosomal miR-148a to activate human microglia. Front Immunol. 2021 Apr 14;12:656700. https://doi.org/10.3389/fimmu.2021.65....
[50] Kyriakopoulos AM, Nigh G, McCullough PA, Seneff S. Mitogen activated protein Kinase (MAPK) activation, p53, and autophagy inhibition characterize the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike protein induced neurotoxicity. Cureus. 2022 Dec 9;14(12):e32361. https://doi.org/10.7759/cureus.32361.
[51] Barreda D, Santiago C, Rodríguez JR, Rodríguez JF, Casasnovas JM, Mérida I, et al. SARS-CoV-2 spike protein and its receptor binding domain promote a proinflammatory activation profile on human dendritic cells. Cells. 2021 Nov 23;10(12):3279. https://doi.org/10.3390/cells10123279.
[52] Chaudhary JK, Yadav R, Chaudhary PK, Maurya A, Roshan R, Azam F, et al. Host cell and SARS-CoV-2-associated molecular structures and factors as potential therapeutic targets. Cells. 2021 Sep 15;10(9):2427. https://doi.org/10.3390/cells10092427.
[53] Erdoğdu B, Kaplan O, Fidan BB, Çelebier M, Malkan ÜY, Haznedaroglu IC. Metabolomic profiling of leukemic hematopoiesis: effects of BNT162b2 mRNA COVID-19 vaccine administration. Curr Mol Med. 2025 Jun 3. http://dx.doi.org/10.2174/01156652403....
[54] Omo-Lamai S, Wang Y, Patel MN, Essien EO, Shen M, Majumdar A, et al. Lipid nanoparticle-associated inflammation is triggered by sensing of endosomal damage: Engineering endosomal escape without side effects. BioRxiv (preprint). 2024 Apr 18. https://doi.org/10.1101/2024.04.16.58....
[55] Ko M, Quiñones-Hinojosa A, Rao R. Emerging links between endosomal pH and cancer. Cancer Metastasis Rev. 2020 Jun;39(2):519-534. https://doi.org/10.1007/s10555-020-09....
[56] Eens S, Van Hecke M, Favere K, Tousseyn T, Guns PJ, Roskams T, Heidbuchel H. B-cell lymphoblastic lymphoma following intravenous BNT162b2 mRNA booster in a BALB/c mouse: A case report. Front Oncol. 2023;13:1158124. https://doi.org/10.3389/fonc.2023.115.... Voir notre article : https://lepointcritique.fr/2023/07/19....
[57] Larsson J, Hellstrand E, Hammarström P, Nyström S. SARS-CoV-2 Spike amyloid fibrils specifically and selectively accelerates amyloid fibril formation of human prion protein and the amyloid β peptide. 2023 Sept 1. bioRxiv. https://doi.org/10.1101/2023.09.01.55....
[58] Francescangeli F, De Angelis ML, Baiocchi M, Rossi R, Biffoni M, Zeuner A. COVID-19–induced modifications in the tumor microenvironment: Do they affect cancer reawakening and metastatic relapse ? Front. Onco l. 2020 Oct 26. https://doi.org/10.3389/fonc.2020.592891.
[59] Theuerkauf SA, Michels A, Riechert V, Maier TJ, Flory E, Cichutek K, et al. Quantitative assays reveal cell fusion at minimal levels of SARS-CoV-2 spike protein and fusion from without. iScience. 2021 Feb 9;24(3):102170. https://doi.org/10.1016/j.isci.2021.1....
[60] Ou X, Liu Y, Lei X, Li P, Mi D, Ren L, et al. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat Commun. 2020 Mar 27;11(1):1620. https://doi.org/10.1038/s41467-020-15....
[61] Nguyen HT, Zhang S, Wang Q, Anang S, Wang J, Ding H, et al. Spike glycoprotein and host cell determinants of SARS-CoV-2 entry and cytopathic effects. J Virol. 2021 Feb 10;95(5): e02304-20https://doi.org/10.1128/JVI.02304-20.
[62] Lazebnik Y. Cell fusion as a link between the SARS-CoV-2 spike protein, COVID-19 complications, and vaccine side effects. Oncotarget. 2021 Dec 7;12 (25):2476-2488. https://doi.org/10.18632/oncotarget.2....
[63] Tang M, Hu X, Wang Y. Ivermectin, a potential anticancer drug derived from an antiparasitic drug. Pharmacol Res. 2021 Jan;163:105207. https://doi.org/10.1016/j.phrs.2020.1....
[64] Braga L, Ali H, Secco I, Chiavacci E, Neves G, Goldhill D, et al. Drugs that inhibit TMEM16 proteins block SARS-CoV-2 spike-induced syncytia. Nature. 2021; 594:88–93. https://doi.org/10.1038/s41586-021-03....
[65] Karikó K, Buckstein M, Ni H, Weissman D. Suppression of RNA recognition by Toll-like receptors: the impact of nucleoside modification and the evolutionary origin of RNA. Immunity. 2005 Aug;23(2):165-75. https://doi.org/10.1016/j.immuni.2005....
[66] Andries O, Mc Cafferty S, De Smedt SC, Weiss R, Sanders NN, Kitada T. N(1)-methylpseudouridine-incorporated mRNA outperforms pseudouridine-incorporated mRNA by providing enhanced protein expression and reduced immunogenicity in mammalian cell lines and mice. J Control Release. 2015 Nov 10;217:337-44. https://doi.org/10.1016/j.jconrel.201....
[67] Kauffman KJ, Mir FF, Jhunjhunwala S, et al. Efficacy and immunogenicity of unmodified and pseudouridine-modified mRNA delivered systemically with lipid nanoparticles in vivo. Biomaterials. 2016 Dec;109:78-87. https://doi.org/10.1016/j.biomaterial....
[68] Kayesh MEH, Kohara M, Tsukiyama-Kohara K. An overview of recent insights into the response of TLR to SARS-CoV-2 infection and the potential of tlr agonists as SARS-CoV-2 vaccine adjuvants. Viruses. 2021 Nov 18;13(11):2302. https://doi.org/10.3390/v13112302.
[69] Mulroney TE, Pöyry T, Yam-Puc JC, Rust M, Harvey RF, Kalmar L, et al. N1-methylpseudouridylation of mRNA causes 1 ribosomal frameshifting. Nature. 2024 Jan;625(7993):189-94. https://doi.org/10.1038/s41586-023-06...
[70] Boros LG, Kyriakopoulos AM, Brogna C, Piscopo M, McCullough PA, Seneff S. Long-lasting, biochemically modified mRNA, and its frameshifted recombinant spike proteins in human tissues and circulation after COVID-19 vaccination. Pharmacol Res Perspect. 2024 Jun;12(3):e1218. https://doi.org/10.1002/prp2.1218.
[71] Benitez Fuentes JD, Mohamed Mohamed K, de Luna Aguilar A, Jiménez García C, Guevara-Hoyer K, Fernandez-Arquero M, et al. Evidence of exhausted lymphocytes after the third anti-SARS-CoV-2 vaccine dose in cancer patients. Front Oncol. 2022 Dec 20;12:975980. https://doi.org/10.3389/fonc.2022.975980.
[72] Lacout A, Lesgards JF, Lounnas V, Azalbert X, Perronne C, Zizi M. Dealing with COVID-19 vaccine related antibody-dependent enhancement: A mini review. Arch Microbiol Immunol. 2024 Jun;8(2): 233-8. https://www.doi.org/10.26502/ami.9365....
[73] Igyártó BZ, Qin Z. The mRNA-LNP vaccines – the good, the bad and the ugly? Front Immunol. 2024 Feb 8;15:1336906. https://www.doi.org/10.3389/fimmu.202....
[74] Uversky VN, Redwan EM, Makis W, et al. IgG4 Antibodies induced by repeated vaccination may generate immune tolerance to the SARS-CoV-2 Spike protein. Vaccines. 2023 May 17;11(5):991. https://doi.org/10.3390/vaccines11050991.
[75] Irrgang P, Gerling J, Kocher K, et al. Class switch toward noninflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. Sci Immunol. 2023 Jan 27;8(79):eade2798. https://doi.org/10.1126/sciimmunol.ad....
[76] Selva KJ, Ramanathan P, Haycroft ER, Reynaldi A, Cromer D, Tan CW,Preexisting immunity restricts mucosal antibody recognition of SARS-CoV-2 and Fc profiles during breakthrough infections. JCI Insight. 2023 Sep 22;8(18):e172470. https://doi.org/10.1172/jci.insight.1....
[77] Shrestha NK, Burke PC, Nowacki AS, Simon JF, Hagen A, Gordon SM. Effectiveness of the coronavirus disease 2019 bivalent vaccine. Open Forum Infect Dis. 2023 Apr 19;10(6):ofad209. https://doi.org/10.1001/10.1093/ofid/....
[78] Yamamoto K. Adverse effects of COVID-19 vaccines and measures to prevent them. Virol J. 2022 Jun 5;19(1):100. https://doi.org/10.1186/s12985-022-01....
[79] Raszek M, Cowley D , Redwan EM, Uversky VN, Rubio-Casillas A. Exploring the possible link between the spike protein immunoglobulin G4 antibodies and cancer progression. Explor Immunol. 2024;4:267-84. https://doi.org/10.37349/ei.2024.00140.
[80] Cavanna L, Grassi SO, Ruffini L, Michieletti E, Carella E, Palli D, et al. Non-Hodgkin lymphoma developed shortly after mRNA COVID-19 vaccination: report of a case and review of the literature. Medicina (Kaunas). 2023 Jan 12;59(1):157. https://doi.org/10.3390/medicina59010157.
[81] Goldman S, Bron D, Tousseyn T, Vierasu I, Dewispelaere L, Heimann P, et al. Rapid progression of angioimmunoblastic T cell lymphoma following BNT162b2 mRNA vaccine booster shot: a case report. Front Med (Lausanne). 2021 Nov 25;8:798095. https://doi.org/10.3389/fmed.2021.798095.
[82] Sekizawa A, Hashimoto K, Kobayashi S, Kozono S, Kobayashi T, Kawamura Y, et al. Rapid progression of marginal zone B-cell lymphoma after COVID-19 vaccination (BNT162b2): a case report. Front Med (Lausanne). 2022 Aug 1;9:963393. https://doi.org/10.3389/fmed.2022.963393.
[83] Gelderloos AT, Verheul MK, Middelhof I, de Zeeuw-Brouwer ML, van Binnendijk RS, Buisman AM, et al. Repeated COVID-19 mRNA vaccination results in IgG4 class switching and decreased NK cell activation by S1-specific antibodies in older adults. Immun Ageing. 2024 Sep 14;21(1):63. https://doi.org/10.1186/s12979-024-00....
[84] Eythorsson E, Runolfsdottir HL, Ingvarsson RF, Sigurdsson MI, Palsson R. Rate of SARS-CoV-2 reinfection during an omicron wave in Iceland. JAMA Netw Open. 2022 Aug 1;5(8):e2225320. https://doi.org/10.1001/jamanetworkop....
[85] Shrestha NK, Shrestha P, Burke PC, Nowacki AS, Terpeluk P, Gordon SM. Coronavirus disease 2019 vaccine boosting in previously infected or vaccinated individuals. Clin Infect Dis. 2022 Dec 19;75(12):2169-77. https://doi.org/10.1093/cid/ciac327.
[86] Chemaitelly H, Ayoub HH, Tang P, Coyle P, Yassine HM, Al Thani AA, et al. Long-term COVID-19 booster effectiveness by infection history and clinical vulnerability and immune imprinting: a retrospective population-based cohort study. Lancet Infect Dis. 2023 Jul;23(7):816-27. https://doi.org/10.1016/S1473-3099(23....
[87] Nakatani E, Morioka H, Kikuchi T, Fukushima M. Behavioral and health outcomes of mRNA COVID-19 vaccination: A case-control study in Japanese small and medium-sized enterprises. Cureus. 2024 Dec 13;16(12):e75652. https://doi.org/10.7759/cureus.75652.
[88] Feldstein LR, Ruffin J, Wiegand R, Grant L, Babu TM, Briggs-Hagen M, et al. Protection From COVID-19 vaccination and prior SARS-CoV-2 infection among children aged 6 months-4 years, United States, September 2022-April 2023. J Pediatric Infect Dis Soc. 2025 Jan 20;14(1):piae121. https://doi.org/10.1093/jpids/piae121.
[89] Ioannou GN, Berry K, Rajeevan N, Li Y, Yan L, Huang Y, et al. Effectiveness of the 2023-to-2024 XBB.1.5 COVID-19 vaccines over long-term follow-up : A target trial emulation. Ann Intern Med. 2025 Mar;178(3):348-359. https://doi.org/10.7326/ANNALS-24-01015.
[90] Martín Pérez C, Ruiz-Rius S, Ramírez-Morros A, Vidal M, Opi DH, Santamaria P, et al. Post-vaccination IgG4 and IgG2 class switch associates with increased risk of SARS-CoV-2 infections. J Infect. 2025 Apr;90(4):106473. https://doi.org/10.1016/j.jinf.2025.1....
[91] McKernan K. Pfizer and Moderna bivalent vaccines contain 20-35% expression vector and are transformation competent in E. coli. 2023. https://anandamide.substack.com/p/pfi....
[92] McKernan K (Medicinal Genomics, US), Nitta T (Tokyo Univ, Japan), Buckhaults PJ (University of South Carolina, US), König B et Kirchner JO (MMD Indep Lab, Magdeburg, Germany), Speicher DJ (University of Guelph, Canada) et McKernan K (Medicinal Genomics, US), Speicher DJ (University of Guelph, Canada), Raoult D (IHU Marseille, France), Kämmerer U (Univ. Hospital of Würzburg, Germany), Wang TJ, Kim A et Kim K, (FDA scientists, Centreville High School, US, executed at FDA White Oak Campus). Résultats dans : https://docs.google.com/spreadsheets/....
[93] Speicher DJ. Full Detailed Report. 2024 Sept 9. https://russellbroadbent.com.au/wp-co....
[94] Kämmerer U, Schulz V, Steger K. BioNTech RNA-Based COVID-19 Injections Contain Large Amounts of Residual DNA including an SV40 Promoter/Enhancer Sequence. Public Health Policy Law. 2024 Mar 12. https://publichealthpolicyjournal.com....
[95] Wang TJ, Kim A, Kim K. A rapid detection method of replication-competent plasmid DNA from COVID-19 mRNA vaccines for quality control. J High School Sc. 2024;8(4):427-39. https://jhss.scholasticahq.com/articl....
[96] Peková S. Quantitative Multiplex Real-Time PCR analysis of Moderna (Spikevax) and Pfizer (BNT162b2) vaccines. 2025 Mar 8. https://www.10letters.org/CzechResear....
[97] Dean DA, Dean BS, Muller S, Smith LC. Sequence requirements for plasmid nuclear import. Exp Cell Res. 1999 Dec 15;253(2):713-22. https://doi.org/10.1006/excr.1999.4716.
[98] Duncan CN, Bledsoe JR, Grzywacz B, Beckman A, Bonner M, Eichler FS, et al. Hematologic cancer after gene therapy for cerebral adrenoleukodystrophy. N Engl J Med. 2024 Oct 10;391(14):1287-1301. https://doi.org/10.1056/nejmoa2405541. Voir notre article : https://lepointcritique.fr/2024/10/14....
[99] Hickey TE, Mudunuri U, Hempel HA, Kemp TJ, Roche NV, Talsania K, et al. Proteomic and serologic assessments of responses to mRNA-1273 and BNT162b2 vaccines in human recipient sera. Front Immunol. 2025 Jan 27;15:1502458. https://doi.org/10.3389/fimmu.2024.15....
[100] OpenVaet, Syed KA, Guetzkow J, Cobalt J, Kunadhasan J, Jackson B. Pfizer/BioNTech C4591001 Trial – Audit Report – v1 (2024-05-31) Reanalysis of the data and anomalies inventoried. 2024 May 31. https://openvaet.substack.com/p/pfize....
[101] Fajloun Z, Sabatier JM. The unsuspected role of the renin-angiotensin system (RAS): Could its dysregulation be at the root of all non-genetic human diseases? Infect Disord Drug Targets. 2024;24(1):e140923221085. https://doi.org/10.2174/1871526524666....
[102] Hazan S, Dave S, Barrows B, Borody T. Messenger RNA SARS-CoV-2 vaccines affect the gut microbiome. Am J Gastroenterol. 2022 Oct;117(10S):e162. https://doi.org/10.14309/01.ajg.00008....
[103] Beaudoin CA, Bartas M, Volná A, Pečinka P, Blundell TL. Are There Hidden Genes in DNA/RNA Vaccines? Front Immunol. 2022 Feb 8;13:801915. https://doi.org/10.3389/fimmu.2022.80....
Les vaccins ARNm anti-COVID peuvent induire le cancer de 17 manières distinctes selon plus de 100 études Mathilde Debord | 19 juin 2025
===================================================
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Bioidentical Hormones 101 Second Edition
Menopausal Hormone Replacement, Health Benefits
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Copyright © 2025 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on August 20th, 2025 by Jeffrey Dach MD
The post Does the C0\/1D \/axxine Cause Cancer? appeared first on Jeffrey Dach MD.
August 11, 2025
Podcast Carol Petersen and Jeffrey Dach MD Bioidentical Hormones 101 Second Edition

Podcast Carol Petersen and Jeffrey Dach MD Bioidentical Hormones 101 Second Edition (2025)
Join Carol Petersen as she interviews Dr. Jeffrey Dach, a renowned expert in bioidentical hormones, about his newly updated book “Bioidentical Hormones 101” second edition (2025). In the interview, we discuss the 2022 study by Dr. Shuyuan Huang who calculated if all women in the US using oral estrogen switched to topical estrogen (transdermal), then 2,245 ischemic strokes per year could be prevented. (1)
We also discussed the Women’s Health Initiative (WHI) Study showing increased breast cancer in the first arm study using Premarin (CEE) with medroxyprogesterone (MPA) of 24 percent (nonsignificant) (hazard ratio [HR] 1.24, 95% CI 1.01–1.53) compared to placebo. (2)
Second Arm WHI shows 45% Reduction in Breast Cancer Mortality
However, for the second arm of the WHI study using Premarin (CEE) alone, the 18 year follow up showed a 45 percent reduction in breast cancer mortality (significant) (hazard ratio [HR] 0.55, 95% CI 0.33–0.92). This indicates estrogen is highly protective and does not cause breast cancer. This is a paradigm shift in our thinking about breast cancer. I would also point out that this 45 percent reduction in breast cancer mortality is larger than any mammography breast cancer screening program, which is in the range of 20-30 percent reduction for breast cancer mortality, according to Dr. Nils Bjurstam (2003). This 45 percent reduction in breast cancer mortality is also larger than any primary prevention study using antiestrogens (tamoxifen or aromatase inhibitors), none of which show any significant reduction in breast cancer mortality. (3-8)
What went wrong with the HABITS STUDY by Lars Holdmerg of Sweden?
We also discussed the HABITS study of Lars Holmberg from Sweden in which breast cancer survivors on tamoxifen were given HRT (estradiol plus norethisterone a synthetic progestin) and compared to non-users. This was the only one of 26 studies of HRT in Breast Cancer Survivors compiled by Avrum Bluming MD which showed an increased breast cancer recurrence in the hormone treated group. All breast cancer recurrence was in tamoxifen users, indicating the development of anti-estrogen resistance. Using the work of Zsuzsanna Suba, a Hungarian pathologist, who writes about the three phases of anti-estrogen resistance, I speculate that this is just another example of the final phase of estrogen resistance with breakthrough of proliferative breast cancer caused by blockade of both the estrogen and androgen receptors. The tamoxifen blocks the estrogen receptors, and the norethisterone (progestin) blocks the androgen receptors.
The HABITS (Hormonal Replacement Therapy After Breast Cancer—Is It Safe?) by Lars Holmberg in Sweden, studied hormone replacement therapy (HRT) in breast cancer survivors (women with a history of breast cancer). The randomized trial compared HRT (primarily estradiol with norethisterone) in 442 breast cancer survivors compared to non-users. After 4 years, the study found an approximate 3-fold increase in new breast cancer events (39 events in the HRT arm [17.6%] vs. 17 in the control arm [7.7%]). (9-10)
The second edition ebook is expanded into three volumes on Kindle. The paperback version contains all three volumes in one comprehensive print edition.
Here is the cover for the paperback version:
Click Here for link to books on Amazon:
ebook Bioidentical Hormones 101 Second Edition (2025) by Jeffrey Dach MD. This is a Three Volume Series e-book
Paperback Version of Bioidentical Hormones 101 second edition (2025). The p aperback contains all three volumes.
Free Video Introduction to Book:
Introduction Video to Bioidentical Hormones 101 Second Edition (2025)
Bioidentical Hormones for Breast Cancer Survivors Video Presentation
Articles with Related Interest:
Hormone Replacement for Breast Cancer Survivors Part One
Hormone Replacement for Breast Cancer Survivors Part Two
Estrogen Metabolism, Iodine, 2MEO Part Three
Testosterone for Breast Cancer Prevention and Treatment
All Bioidentical Hormone Articles
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Links and References:
1) Huang, Shuyuan, et al. “Research Progress on The Role of Hormones in Ischemic Stroke.” Frontiers In Immunology 13 (2022): 1062977.
2) Rossouw, Jacques E., et al. “Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial.” Jama 288.3 (2002): 321-333.
3) Chlebowski, Rowan T., et al. “Association of menopausal hormone therapy with breast cancer incidence and mortality during long-term follow-up of the women’s health initiative randomized clinical trials.” Jama 324.4 (2020): 369-380.
4) Manson, JoAnn E., et al. “Menopausal hormone therapy and long-term all-cause and cause-specific mortality: the Women’s Health Initiative randomized trials.” Jama 318.10 (2017): 927-938.
5) Hodis, Howard N., and P. M. Sarrel. “Menopausal hormone therapy and breast cancer: what is the evidence from randomized trials?.” Climacteric 21.6 (2018): 521-528.
6) Bjurstam, Nils, et al. “The Gothenburg Breast Screening Trial.” Cancer: Interdisciplinary International Journal of the American Cancer Society 97.10 (2003): 2387-2396
7) Cuzick, Jack, et al. “Selective oestrogen receptor modulators in prevention of breast cancer: an updated meta-analysis of individual participant data.” The Lancet 381.9880 (2013): 1827-1834.
8) Cuzick, Jack, et al. “Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled trial.” The Lancet 383.9922 (2014): 1041-1048.
9) Holmberg, Lars, et al. “Increased risk of recurrence after hormone replacement therapy in breast cancer survivors.” Journal of the National Cancer Institute 100.7 (2008): 475-482.
10) Suba, Zsuzsanna. “The pitfall of the transient, inconsistent anticancer capacity of antiestrogens and the mechanism of apparent antiestrogen resistance.” Drug design, development and therapy (2015): 4341-4353.
============================================================
More Links:
Get the book: [Bioidentical Medical Hormones 101 on Amazon] (https://amzn.to/41kSvcs) (Kindle Volumes 1-3 or Print Edition)
‘Dr. Dach’s Website: [JeffreyDachMD.com](https://jeffreydachmd.com/) (Check out Carol’s original testimonial here!)
Related Books Mentioned:
Cracking Cancer Toolkit by Dr. Jeffrey Dach: [Amazon Link](https://amzn.to/4ouxxlx) Hormone Deception by Lindsey Berkson: [Amazon Link](https://amzn.to/45zrAMu) Iodine: Why You Need It by Dr. David Brownstein: [Amazon Link](https://amzn.to/4froair)Other Resources:
Women’s Health Initiative Study (2017 Follow-Up): [JAMA Article](https://jamanetwork.com/journals/jama…) Carol Petersen’s Website: [TheWellnessByDesignProject.com](https://thewellnessbydesignproject.com/) (For more on hormones and wellness)Bioidentical Hormones 101: A Comprehensive Guide: Unraveling the Confusion [Carol’s Review of Jeffrey Dach’s Books] (https://thewellnessbydesignproject.co…)
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
my blog: www.jeffreydachmd.com
Bioidentical Hormones 101 Second Edition
Menopausal Hormone Replacement, Health Benefits
Natural Thyroid Toolkit by Jeffrey Dach MD
Cracking Cancer Toolkit by Jeffrey Dach MD
Heart Book by Jeffrey Dach MD
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
www.drdach.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Copyright © 2025 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on August 11th, 2025 by Jeffrey Dach MD
The post Podcast Carol Petersen and Jeffrey Dach MD Bioidentical Hormones 101 Second Edition appeared first on Jeffrey Dach MD.
Jeffrey Dach's Blog

- Jeffrey Dach's profile
- 3 followers


.jpg){kind=link}
{kind=link}