
Jeffrey Dach's Blog, page 8
December 26, 2022
Iodine Treatment of Graves Disease Part Two
 Iodine Treatment of Graves’ Disease Part Two
Iodine Treatment of Graves’ Disease Part Two
Jeffrey Dach MD
This is Part Two, For Part One, Click Here. Header image thyroiditis courtesy of wikimedia commons.
One of the concerns about Iodine treatment of Graves Disease, is some patients do not respond or escape from the suppressive effects of iodine, leading to more difficult to treat thyrotoxicosis. This was decribed in a 2015 study by Dr. Ai Yoshihara switching from Methimazole to Iodine in Graves’ Disease women during pregnancy. Although 90 per cent successful, about 9-10% of patients escaped from the suppressive effects of Iodine and worsened the hyperthyroidism. This was unpredictable with no obvious parameters to predict which patients would respond well, and which patients would worsen. (1-3)
Okamura Study 504 Graves’ Patients Treated with Iodine Alone
In 2022, Dr. Ken Okamura provided us with a protocol for treating Graves Diease with Iodine as first line therapy, including the management of Iodine escape, or Iodine resistance. Proclaiming that “iodide in higher doses is an established and time-honored treatment of Graves’ Disease”, and is safer than thyroid blocking drugs such as methimazole, Dr. Ken Okamura recruited 504 untreated Graves’ Disease patients and began treatment with 100 mg of potassium iodide daily, seeking to avoid thionamide drugs, methimazole and PTU, which carry potentially severe adverse side effects. In Japan, one person dies annually from thionamide drug -induced suppression of the white blood cells (agranulocytosis). Dr. Ken Okamura writes:
iodide in higher doses is an established and time-honored treatment of GD [Graves Disease]…However, both MMI [methimazole] and PTU [propylthiouracil] were still associated with severe notorious or unfamiliar side effects. In Japan, one GD patient on average dies due to thionamide-induced agranulocytosis every year…The possibility of KI therapy was therefore suggested in general untreated GD from the beginning…many patients to have mild or even asymptomatic GD that may be sensitive to excess iodide. (4)
 Relapse of Hyperthyroidism on Iodine Therapy when Tapering
Relapse of Hyperthyroidism on Iodine Therapy when Tapering
A subset of 92 of the 504 Graves’ patients (18.3%) were too responsive to iodine. Initially, the high Free T4 level became very low, and TSH very high in response to iodine treatment. In the first half of the study, in 41 such patients with high TSH, the Iodine dosage was tapered down. However, 71% then relapsed into hyperthyroidism. In the second half of the study, for 39 “overly sensitive to iodine” patients, the iodine was no longer tapered down. Instead, these 39 patients were treated Block and Replace, by addition of levothyroxine to reduce the TSH. None of these 39 patients had relapse of hyperthyroidism. This is a justifiable use of Block and Replace. Dr. Ken Okamura writes:
in the latter half of this study, the patients were treated with the combination of 100 mg KI and LT4 [levothyroxine] when the serum fT4 level became low and the TSH level became detectable (combined fixed dose KI and LT4 therapy). In this combined therapy (n = 39), compared with tapering therapy (n = 41), a relapse of hyperthyroidism was not observed (0% vs. 71%, p < 0.0001) and the degree of TSH elevation was reduced (e.g. 10.7 [6.6–23.3] μU/mL vs. 27.3 [8.6–68.3] μU/mL), although the difference was not significant (p = 0.0561). … It was very important to keep the serum iodide level above the threshold for the WC [Wolf- Chaikoff] effect, avoiding the tapering method usually performed in MMI therapy. The KI dosage could be reduced later when TBII became negative or patients had nearly achieved remission. (4)
Lesson number One: Do not taper the Iodine dosage when T4 goes too low and TSH goes too high. Instead use Block and Replace with Levothyroxine.
Iodine Escape – Strategy for KI-resistant and/or escaped patients: addition of low-dose thionamide
202 patients were considered have “escaped” or resistant to Iodine Suppression. These were treated with a combination of Potassium iodide (KI) 100 mg/per day and Methimazole 5-15 mg per day with good results. Once starting combination of methimazole with KI, it was about 7 weeks until FreeT4 normalization.
During this study, 126 (25.0%) patients were treated by ablative therapy (RAI 104 patients and surgery 22 patients), usually 2-3 years after starting medical therapy. Patients treated with RAI (Radioactive Iodine) had the 100 mg potassium iodine withheld for 4-7 days and then had 60% Iodine uptake prior to RAI treatment. This uptake is similar to untreated Graves’ Disease, so Iodine Treatment was not an issue for RAI. Dr Ken Okamura writes:
After RAI treatment in Groups B and C [iodine escaped or resistant], 86% of the patients achieved a euthyroid- or hypothyroid status with a decrease in thyroid volume. It was then concluded that KI therapy did not interfere with the efficacy of RAI.(4)
Features Predicting Escape, Goiter Size, Free T3 Levels, and TSH
Escape or Iodine Resistance was more frequent in patients with larger thyroid goiters, and with higher Free T3 levels (greater than 10 pg/ml). Dr. Ken Okamura thought this high Free T3 was a marker of strong TSH receptor stimulation (and therefore thyroid stimulation), either from Graves antibodies or Elevated TSH, with a high turnover of both thyroglobulin and Iodide. The third factor was TSH level, as there was no escape in patients who responded early to Iodine with normalization of TSH and T4 levels. Escape from Iodine was seen only in those patients with continued TSH suppression after iodine treatment. Dr. Ken Okamura writes:
T3 predominant synthesis and secretion is a good marker of the thyroid gland being strongly stimulated with high turnover of both Tg [thyroglobulin] and iodide, as found in cases of iodine deficiency.
Timing of Adding Methimazole
Dr. Ken Okamura feels that the 60-day window for achieving euthyroid status is important. If the patient fails to achieve euthyroid status (normal Free T4) or “escapes” within 60 days, methimazole 5-15 mg/day should be added to the Potassium iodide 100 mg/day. The addition of MMI to Iodine could overcome Iodine resistance or escape. In addition, Radioactive Iodine therapy was also effective to overcome iodine resistance. Note: escape means: initially achieves normal Free T4, then later relapses with high T4. Dr. Ken Okamura writes:
When treating GD with KI, the timing for adding MMI is important. If patients fail to achieve euthyroid status within 60 days or escape occurs, it may be better to begin combined KI and MMI therapy…The important conclusion from this study was that KI resistance or escape from the KI effect could be overcome either by combined KI and MMI therapy…or RAI [radioactive iodine] therapy…In conclusion, the serum fT4 levels declined in all patients with GD [Graves Diease] following KI therapy. Among GD patients treated with 100 mg KI, 34% were KI-sensitive with detectable TSH and a good prognosis, 50% were KI-sensitive with TSH suppression and 16% were KI resistant. KI was immediately excreted into urine without serious side effects. Escape was only observed in TSH suppressed patients. KI-resistant and escaped patients were able to be treated with a combination of KI and a small dosage MMI, or RI, as usual. We can minimize the use of thionamide with serious side effects by adopting the “KI or RI” strategy for the treatment of GD without impending serious symptoms. (4)
Eighty Per Cent Remission Rate for Responders
Dr. Ken Okamura found that for patients who show an early good response to iodine with normalization of TSH, these will ultimately achieve an 80% remission rate. If the patient does not achieve euthyroid status within 60 days, then additional MMI is indicated as these patients would otherwise have a high rate of escape from Iodine, (33-83%). This combined group has a 50% chance for remission. Dr. Ken Okamura writes:
Regarding the strategy for GD treatment depending on the early response to 100 mg KI, KI treatment could be continued in Group A. Nearly 80% remission or spontaneous hypothyroidism could be expected. If the serum fT4 and fT3 levels do not normalize within 60 days, the patients may belong to Group B or C (Table 3). Combined KI and MMI therapy is then recommended, as a 33%–82% chance of escape is expected later…. (4)
Escape from Iodine or Painless Thyroiditis?
A second paper in 2022 also by Dr Ken Okamura makes the bold suggestion that many patients under treatment for Graves Disease who relapse into hyperthyroidism have thyroiditis, an inflammatory process, called painless thyroiditis (PT). This may be true for both Iodine and Methimazole, and as mentioned above is usually associated with decreasing the treatment dosage.
Dr Okamura reviewed 100 patients who presented unexpected relapsing hyperthyroidism while decreasing dosage while under treatment for Graves’ disease with Potassium Iodide, methimazole or PTU. All had radionuclide iodine uptake scans. Many of these scans showed under 5 per cent uptake indicating thyroiditis was the cause of the thyrotoxicosis rather than worsening Graves’ Disease. In this regard, PT may resemble Hashitoxicosis, a type of thyrotoxicosis with very low radio-iodine uptake. Indeed, 70 per cent of Graves patients are also positive for Hashimoto’s antibodies. Dr Okamura writes:
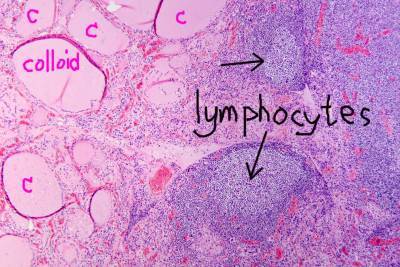
GRAVES’ DISEASE (GD) and Hashimoto thyroiditis are recognized as being pathologically interrelated, as GD may occur in patients whose thyroid glands histologically show either Hashimoto thyroiditis alone or a mixture of both parenchymatous hypertrophy of GD and extensive lymphocytic infiltration. These two conditions may represent a single disease entity with a wide range of manifestations.(5)
Mechanism of Thyroiditis
What is the mechanism causing thyroiditis upon reduction in dosage of anti-thyroid medication? Dr Okamura reminds us that excess iodine can cause a “toxic effect”, i.e. thyroiditis. Animal studies show that selenium supplementation ameliorates the toxic effects of iodine excess. I would suggest the mechanism involves increased hydrogen peroxide activity in the face of insufficient selenium-based antioxidant ability, caused by underlying selenium or magnesium deficiency. The excess hydrogen peroxide causes oxidative damage to adjacent structures which are thyroglobulin, TPO and thyrocytes, leading to inflammation and release of preformed thyroid hormone. (9-22)
Dr Okamura writes:
PT [painless thyroiditis] was frequently observed during KI treatment. In Group A [low radioiodine uptake], 19 (54.3%) patients were treated by KI alone or KI and MMI before the episode of PT. Given the effect of excess iodide on the morphological changes in the thyroid, KI treatment may precipitate the “iodide thyroiditis” reported by Edmunds in 1955. In the same year as Gluck reported convincing cases with PT, Savoie reported 10 cases of iodine-induced thyrotoxicosis in apparently normal thyroid glands, ranging from 1 to 40 months after exposure to excess iodine. They all showed a typical clinical course of PT with a low RAIU followed by hypothyroidism…From a therapeutic perspective, it is very important to keep in mind that PT [painless thyroiditis] can occur during ATD [anti-thyroid drug] treatment of GD, especially when the dosage is reduced…The diagnosis can be confirmed by the suppressed RAIU [radio iodine uptake] (<5%/5 h) in the thyrotoxic state, which remains a valuable factor for differentiating PT from relapse of GD. (5)
Returning to the 2015 Yoshihara study of pregnant Graves’ patients showing a 9-10 percent iodine escape rate when converting from MMI to Iodine, one wonders how many of these iodine escape cases are related to thyroiditis, an inflammatory process similar to Hashitoxicosis ? A radionuclide uptake study would resolve the issue. It would also be useful to know the selenium and magnesium status of these patients. One would ask the obvious question: Would the escape rate be decreased if patients had been given selenium and magnesium supplements? (9-22)
Conclusion: Dr Okamura makes a brilliant case for the first line use of Iodine for Graves’ Disease. Firstly, Iodine is safer than thyroid blocking drugs. Secondly for early responders, they enjoy an 80 per cent remission rate. For those patients who escape or are resistant to Iodine, Dr Okamura provides us with a clear and well thought out protocol adding a second drug, methimazole to the Iodine, or if that fails, radioiodine ablation. One wonders what would have been the escape rate if Lithium Carbonate had been combined with the Iodine as suggested by Dr. Jonathan Wright. (6-8)
Articles with Related Interest
Graves Disease Remission with Iodine Part One
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
header image courtesy of wikimedia : thyroiditis
References
Note on definitions: Autoantibodies to thyroglobulin (Tg) (TGHA) and thyroid microsomal antigen (MCHA).Group A: KI-sensitive patients with recovered serum TSH. Group B: KI-sensitive patients with suppressed serum TSH. Group C: KI resistant patients. Escape: Re-elevation of the serum fT4 and/or fT3 levels after temporary reduction in serum fT4 levels while taking 100 mg KI within 180 days.
Yoshihara, Ai, et al. “Substituting potassium iodide for methimazole as the treatment for Graves’ disease during the first trimester may reduce the incidence of congenital anomalies: a retrospective study at a single medical institution in Japan.” Thyroid 25.10 (2015): 1155-1161Yoshihara, Ai, et al. “Characteristics of Patients with Graves’ Disease Whose Thyroid Hormone Levels Increase After Substituting Potassium Iodide for Methimazole in the First Trimester of Pregnancy.” Thyroid: official journal of the American Thyroid Association 30.3 (2020): 451-456.Pearce, Elizabeth N. “Substituting Potassium Iodide For Methimazole In First-Trimester Pregnant Women With Graves’ Disease May Unpredictably Worsen Hyperthyroidism.” Clinical Thyroidology 32.3 (2020): 117-119.Okamura, Ken, et al. “Iodide-sensitive Graves’ hyperthyroidism and the strategy for resistant or escaped patients during potassium iodide treatment.” Endocrine Journal (2022): EJ21-0436.Okamura, Ken, et al. “Painless thyroiditis mimicking relapse of hyperthyroidism during or after potassium iodide or thionamide therapy for Graves’ disease resulting in remission.” Endocrine Journal (2022): EJ22-0207.Sharma, Pranjali P. “Use of Lithium in Hyperthyroidism Secondary to Graves’ Disease: A Case Report.” The American Journal of Case Reports 23 (2022): e935789-1.Nair, Gopalakrishnan C., et al. “Preoperative preparation of hyperthyroidism for thyroidectomy–Role of supersaturated iodine and lithium carbonate.” Indian Journal of Endocrinology and Metabolism 22.3 (2018): 392.Boehm, Timothy M., et al. “Lithium and iodine combination therapy for thyrotoxicosis.” European Journal of Endocrinology 94.2 (1980): 174-183.Vasiliu, Ioana, et al. “Protective role of selenium on thyroid morphology in iodine‑induced autoimmune thyroiditis in Wistar rats.” Experimental and therapeutic medicine 20.4 (2020): 3425-3437.Xu, Jian, et al. “Selenium supplement alleviated the toxic effects of excessive iodine in mice.” Biological Trace Element Research 111.1 (2006): 229-238.Xu, Jian, et al. “Intervention of selenium on injured thyroid hormone metabolism by excessive iodine.” Journal of Hygiene Research 38.4 (2009): 398-400.Xu, Jian, et al. “Supplemental selenium alleviates the toxic effects of excessive iodine on thyroid.” Biological trace element research 141.1 (2011): 110-118.Wang, Weiwei, et al. “Effects of selenium supplementation on spontaneous autoimmune thyroiditis in NOD. H-2h4 mice.” Thyroid 25.10 (2015): 1137-1144.Duntas, L. H. “The role of iodine and selenium in autoimmune thyroiditis.” Hormone and Metabolic Research 47.10 (2015): 721-726.Vanderpas, Jean B., et al. “Iodine and selenium deficiency associated with cretinism in northern Zaire.” The American journal of clinical nutrition 52.6 (1990): 1087-1093.Vanderpas, Jean-Baptiste, et al. “Iodine and selenium deficiency in northern Zaire.” The American journal of clinical nutrition 56.5 (1992): 957-958.Contempre, Bernard, et al. “Effects of selenium deficiency on thyroid necrosis, fibrosis and proliferation: a possible role in myxoedematous cretinism.” European Journal of Endocrinology 133.1 (1995): 99-109.Contempre, Bernard, et al. “Selenium deficiency aggravates the necrotizing effects of a high iodide dose in iodine deficient rats.” Endocrinology 132.4 (1993): 1866-1868.Davcheva, Delyana M., et al. “Serum selenium concentration in patients with autoimmune thyroid disease.” Folia Medica 64.3 (2022): 443-449.Bogusławska, Joanna, et al. “Cellular and molecular basis of thyroid autoimmunity.” European Thyroid Journal 11.1 (2022).Negro, Roberto. “Selenium and thyroid autoimmunity.” Biologics: Targets and Therapy 2.2 (2008): 265-273.Kimura, T. A. K. A. O., et al. “Thyrotropin-induced hydrogen peroxide production in FRTL-5 thyroid cells is mediated not by adenosine 3′, 5′-monophosphate, but by Ca2+ signaling followed by phospholipase-A2 activation and potentiated by an adenosine derivative.” Endocrinology 136.1 (1995): 116-123.Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
www.drdach.com
Heart Book by Jeffrey Dach
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright (c) 2018 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on December 26th, 2022 by Jeffrey Dach MD
The post Iodine Treatment of Graves Disease Part Two appeared first on Jeffrey Dach MD.


October 30, 2022
Thyroid T3/T4 Combination Therapy vs T4-Monotherapy
 Thyroid T3/T4 Combination Therapy vs T4-Monotherapy
Thyroid T3/T4 Combination Therapy vs T4-Monotherapy
by Jeffrey Dach MD
Susan is a 42-year-old Professor of Literature at the local college. About four years ago, she was treated with radioactive iodine (thyroid ablation) for Graves’ Disease. Susan now requires lifelong thyroid replacement. After seeing four different endocrinologists who prescribed various doses of thyroid medication, Susan is still unhappy with her treatment. The last endocrinologist prescribed 175 mcg of Levothyroxine, and Susan’s TSH is suppressed down to a very low 0.01. However, Susan continues to suffer from chronic fatigue, depression, weight gain, foggy thinking, and constipation, all typical symptoms of a low thyroid condition. Susan was crying in my office as she told her story of frustration. Above left image: thyroid ultrasound courtesy of wikimedia commons.
T4 Only Medication Cannot Guarantee Euthyroid State
T4 medication (Levothyroxine) is a prohormone and must be converted to its active form, T3. This is done by the D2 deiodinase enzyme system inside the cells of the peripheral tissues. The assumption made by the endocrinologist when using T4 monotherapy with Levothyroxine, generic Synthroid, is this:
It is assumed T4-only medication (Levothyroxine) is converted to T3 by the peripheral tissues at the proper rate to produce normal thyroid levels. This assumption is incorrect as shown by studies at Rush Medical Center in Dr. Antonio Bianco’s lab. The paradigm shift in thyroid endocrinology is understanding the conversion of T4 to its active form, T3, is controlled by the deiodinase enzyme system at the cellular level. This has been ignored by mainstream endocrinology, leading to a number of errors, one of which is the dogmatic perpetuation of T4-monotherapy. (2)(38-40)(43-44)
In 2011, Dr Damiano Gullo from Italy reported T4 to T3 conversion is defective in about 20% of patients treated with Levothyroxine (T4 monotherapy) after thyroid ablation (athyreotic patients). Dr. Gullo writes:
Athyreotic patients have a highly heterogeneous T3 production capacity from orally administered levothyroxine. More than 20% of these patients, despite normal TSH levels, do not maintain FT3 or FT4 values in the reference range, reflecting the inadequacy of peripheral deiodination to compensate for the absent T3 secretion. A more physiological treatment than levothyroxine monotherapy may be required in some hypothyroid patients.(21)(3)
Indeed, Susan’s labs showed a high Free T4 of 1.6 and a low Free T3 of 240 indicating poor conversion of T3 to T4, “reflecting the inadequacy of peripheral deiodination to compensate for the absent T3 secretion”. A number of animal studies have been done to answer this question of why peripheral conversion of T4 to T3 is reduced. (21)
 Left image chemical structure of levothyroxine courtesy of wikimedia commons
Left image chemical structure of levothyroxine courtesy of wikimedia commons
T4 – Monotherapy Explained
The key to understanding the failings of T4-monotherapy lies with the D2 deiodinase enzyme system which resides in our cells, and plucks an iodine molecule off of T4, converting it to T3, the active form of the hormone. In a 2013 report, Dr. Antonio Bianco says this intracellular D2 deiodinase enzyme system is the master controller for thyroid levels and creates a new paradigm in our understanding of thyroid function:
Thyroid hormone–responsive metabolic processes are turned on and off by thyroid hormone via deiodination pathways that are taking place inside the target cells, seemingly invisible from the plasma viewpoint…. deiodination supports a new paradigm in which hormones are activated or inactivated in a controlled fashion in specific thyroid hormone-target tissues. (38)
D2 in the Pituitary Acts Differently from D2 in Periphery
According to a 2015 animal study by Dr De Castro, the D2 deiodinase enzyme system in the pituitary acts differently from the D2 in the peripheral tissues. In the peripheral tissues, D2 is inactivated by T4. This is a safety mechanism to protect the cells from hyperthyroidism with dangerously high T4 levels. T4 inactivates the D2 enzyme in the peripheral tissues, thereby preventing conversion of T4 to its active form, T3.
However, the D2 in the hypothalamus and pituitary is a different type of D2 which is not inactivated by T4. In the hypothalamus and pituitary, the abundant T4 in circulation is promptly converted to intracellular T3 which will then suppress the TSH to low levels. This results in the pattern we see with Susan’s, labs, relatively higher serum T4 and relatively lower serum T3. In the periphery, cells are starved of T3 because of inactivation of the D2 enzyme by T4, which inhibits conversion of T4 to T3 in the peripheral tissues. In his mouse study, Dr De Castro found that only constant infusion of both T4 and T3 normalized thyroid levels. Dr De Castro writes:
in contrast to other D2 expressing tissues, the hypothalamus is wired to have increased sensitivity to T4… only constant delivery of L-T4 and L-T3 fully normalizes T3 -dependent metabolic markers and gene expression profiles in thyroidectomized rats. (39)
In most tissues, exposure to T4 inactivates the D2 deiodinase, which decreases conversion of T4 to T3, and decreases peripheral production of T3. Similarly, this also occurs in the brain, where the elevated serum T4/T3 ratio results in hypothyroid brain cells. However, the exception to this rule is the hypothalamus where the D2 deiodinase is less susceptible to T4 induced inactivation, causing suppression of TSH with Levothyroxine T-4 monotherapy, while in the periphery, T4 conversion to T3 via D2 is inhibited by T4, creating a hypothyroid state. This explains the findings in thyroidectomized mice in which T4 treatment normalizes TSH, yet there is reduced peripheral T3. This also explains the failings of Susan’s T4-only monotherapy with levothyroxine which suppresses her TSH, while leaving the peripheral tissues in a hypothyroid state. (38-40)
Combination Treatment with T3 andT4
If T4-monotherapy leads to cellular hypothyroidism in the periphery while centrally, a suppressed TSH, what is the solution? Combined therapy with both T3 and T4 may resolve this problem. The past dogmatic insistence on T4 monotherapy seems to be changing, as more and more endocrinologists are embracing combination T3 and T4 therapy. In 2014, Dr Wilmar Wiersinga writes:
Levothyroxine plus liothyronine [generic Cytomel] combination therapy is gaining in popularity….in some of the 14 published trials this combination was definitely preferred by patients and associated with improved metabolic profiles. (1) Note: liothyronine is T3.
Perhaps the research using thyroidectomized mice from 1995 and 1996 by Dr Escobar is convincing. In studies using thyroidectomized mice, Dr Escobar found that T3 and T4 levels could not be normalized with T4 monotherapy alone. Rather, a steady infusion of both drugs, T3 and T4, were needed to maintain a euthyroid state. In addition, a number of human studies show that patients prefer combination therapy. (1)(3,4)
Adverse Effects of Thyroid Pills
Adverse effects of thyroid excess are similar for all three types of thyroid medication, levothyroxine, NDT and combination therapy. Rapid heart rate at rest (tachycardia), is the symptom we are most concerned about, and the patient is instructed to watch for this and hold the thyroid pill if this is noted. Other symptoms of thyroid excess to watch out for include anxiety, insomnia and loose stools.
Which type of thyroid pill do you prefer?
1) Synthetic T4 andT3. Mainstream endocrinology uses Levothyroxine (T4) combined with Cytomel (T3) in a ratio of (12:1).
2) T4 plus a slow release compounded T3 to avoid supraphysiologic dosing of T3 which peaks 2 hours after ingestion.
3) NDT, Natural Desiccated Thyroid which contains T4:T3 in ratio of 4:1.
4) NDT plus T4 Levothyroxine. Some patients prefer a 12:1 ratio of T4 to T3, so adding an appropriate dose of T4 to NDT will do the trick.
Here is a sample dosing schedule:
Half Grain tablet of NDT twice a day provides 4.5 mcg of T3 twice a day (total 9 mcg), and a total T4 dosage of 76 Mcg. Add another daily 25 Mcg of (T4) Levothyroxine to obtain the desired T4:T3 ratio of (101: 9) = (11.2:1).
We have found a few patients after thyroid ablation may prefer adding T4 to obtain this combination.
Option 1) Combined T3 and T4 (Levothyroxine and Cytomel)
This option is discussed by Dr Colin Dayan in 2018 Thyroid Research. Dr. Dayan prefers a T4:T3 ration of (14:1) because this closely matches the natural secretion rate for T4 and T3 by the human thyroid gland. In 2018, Dr Dayan writes:
“The doses (for NDT) give a T4:T3 ratio of 4.2:1, significantly more T3 than the 14:1 secreted by the normal thyroid and the doses recommended above. This makes dosing difficult as displayed by several studies which have shown supraphysiological T3 doses post dose, fluctuating T3 levels during the day and more hyperthyroid symptoms in subjects taking DTE compared to LT4 monotherapy.” … “Furthermore, it has also been shown that the majority of circulating T3 comes from peripheral conversion of T4 to T3 and not secretion of T3 from the thyroid [8], hence a T4:T3 secretion ratio of approximately 14:1 appears average in humans, suggesting only a small role for secreted T3…Practicing clinicians will be able to identify a group of patients not satisfied on LT4 monotherapy which makes up a small subset of all their patients on LT4…. Both ATA and ETA suggest that in an appropriate clinical setting (see below) combination therapy may be trialed to determine if it is beneficial for the individual patient…. despite recommendations and guidelines from various specialist bodies, use of combination T4/T3 therapy appears significant in most developed countries.”(37)
Dr Colin Dayan’s routine is to give a T3 (generic Cytomel) to a patient already on “adequate LT4 monotherapy ” (usually 75-150 mcg levothyroxine), yet still having symptoms of hyopothyroidism. Dr Dayan will then remove some of the T4 dose (usually 50-75 mcg T4) and replace it with (5 – 20) mcg of T3, usually generic Cytomel (Liothyrronine) in a split dose given twice a day to avoid or reduce “supraphysiologic dosing”.
Option 2 Slow Release T3
Dr Martin Milner describes his routine using compounded slow release T3 in his article in the Townsend Letter 2005. In order to avoid supraphysiologic dosing with T3, Dr Milner suggests using slow release compounded T3.(36)
Option 3: Synthetic T3 and T4 Combination
Which T4:T3 Ratio do You Prefer 14:1 or 4:1 ? As mentioned above, a major objection to NDT, Natural Desiccated Thyroid) is the T4:T3 ratio which is 4:1, providing a much larger T3 bolus compared to the 14: 1 ration (T4:T3) ratio discussed by Dr Colin Dayan in his 2018 article .(37)
Others such as Dr Martin Milner disagree, and actually prefer to use the 4:1 (T4:T3) ratio commonly found in NDT. Perhaps Dr Milner is right, since this 4:1 (T4:T3) ratio is closer to the serum (T4:T3) ratios for the average patient which is 3.3:1. Dr. Jernej Grmek, in the 2015 Slovenian Medical Journal, studied the free thyroxine to free triiodothyronine ratios (FT4:FT3) in 225 patients, reporting this mean ratio was 2.86 ± 0.52.(41) This discrepancy between serum T4:T3 (3.3:1) ratio and secreted T4:T3 (14:1) ratio can be explained by the fact that 80% (most) of our T3 comes from peripheral conversion of T4 to T3 via the intra-cellular D2 Deiodinase Enzyme. Of the circulating Free T3, only 20 % comes from thyroid secretion, the remaining 80% from peripheral conversion of T4 to T3 via the Type 2 De-Iodinase Enzyme.(36-37)
5:1 Ratio Combination T3 and T4 Wins the Contest
in 2005, Dr. Bente Appelhof studied two different T4:T3 synthetic combination ratios, 5:1 and 10:1 ratios and compared them to T4 monotherapy in a randomized double blind study in 141 patients with Hashimoto’s hypothyroidism. About 47 patients were randomized to each treatment group, T4 monotherapy, 4:1 combination or 10:1 T4:T3 synthetic combination therapy. The 5:1 ratio was most preferred by the patients. Please note, this T4:T3 (5:1) ratio synthetic combination most closely approximates the 4:1 ratio found in NDT Natural Desiccated Thyroid. (16)
Which Thyroid Pill is Best, Synthetic Combination or NDT?
In 2018 by Dr. Anam Tariq from Johns Hopkins examined this question. Dr Tariq performed a retrospective observational study of 100 patients from an endocrinology clinic in Pennsylvania over six years comparing T4 monotherapy to both synthetic T3, T4 combination therapy and NDT, natural Desiccated Thyroid. Patients on T4 monotherapy for a year who continued to complained of hypothyroid symptoms were candidates for combination therapy. Starting dose for T3 was “5 μg in conjunction with an appropriate decrease of 12.5 μg in LT4 to achieve the standard physiological circulating FT4:FT3 ratio of nearly 14:1.“ The maximum dose of T3 was 12.5 mcg. Starting dose for NDT was 15mg (quarter grain) and the titrated up. T4:T3 ratio was of course 4:1 for NDT. The authors also checked and optimized B12 and Vitamin D levels in all patients.
The average dose of DTE (NDT) was 30 mg. The average LT4/LT3 dose was 75 μg/5 μg to obtain physiologic thyroid levels. Fifty-two percent had Hashimoto disease, 22% had surgical hypothyroidism, 10% had ablation for either Graves’ disease or thyroid cancer, and 16% had miscellaneous etiologies. (30)
I found it remarkable that the mean TSH for all treated patients was in the 1.8 to 1.9 range, regardless of the particular combination of thyroid medication. Likewise, the Free T3 and Free T4 levels were remarkably similar across all treatment modalities. Adverse effects of synthetic combination therapy were:
6.7% of the 100 patients complained of palpitations and anxiety and had confirmed TSH <0.35 μIU/mL but without atrial arrhythmias. (30)
Many of the patients reported feeling better on combination therapy (either NDT or Synthetic T3,T4) compared to Levothyroxine monotherapy. Both combination therapies seemed equally safe and effective. The authors conclude:
Combination therapy of LT4 and LT3 has remained an experimental treatment that can be used at the physician’s discretion. Our observational study concludes that for a subset of patients who feels suboptimal on LT4 monotherapy, synthetic therapy is beneficial and safe in controlling hypothyroid symptoms and improving quality of life. (30)
Genetic Mutations in the D2 Deioidinase
As mentioned above, the D2 Deiodinase enzyme is the master control mechanism for tissue level conversion of T4 to T3. What if the patient harbors a polymorphism (mutation) in the D2 deiodinase gene? Will this affect the T4 to T3 peripheral conversion ability? And, if so, would these patients prefer combination therapy? Dr Allan Carle says yes, of course. In 2017, Dr Carle studied 45 autoimmune hypothyroid patients on Levothyroxine using genetic analysis of the D2 gene. 60 per cent of patients harboring D2 gene polymorphisms preferred combination therapy with both T3 and T4. If two SNPs (single nucleotide polymorphisms) were present, all of these (100%) patients preferred combination therapy. (42-46)
Major Objection to NDT – High peak T3 levels
Mainstream Endocrinology’s major objection and reason for rejecting NDT is the high T3 peak for a few hours after ingestion of the pill. (5) However, this argument also applies to combination therapy with levothyroxine and generic Cytomel which has recently become acceptable for mainstream endocrinologists. In 2012, Dr Wiersinga writes about combination T4 and T3 therapy:
It is suggested to start combination therapy in an L-T4/L-T3 dose ratio between 13:1 and 20:1 by weight (L-T4 once daily, and the daily L-T3 dose in two doses). Currently available combined preparations all have an L-T4/L-T3 dose ratio of less than 13:1, and are not recommended. (5-6)
This argument seems rather vacuous, since many patients do well with NDT which contains a T4:T3 ratio of 4:1. In addition, many patients do well on synthetic combination T3 and T4 with the 5:1 ratio as described above by Dr. Bente Appelhof in 2005. This is very similar and essentially the same ratio as found in NDT, Natural Desiccated Thyroid, which is 4:1. If one objects to the T3 in NDT, then one must object equally to T3 in synthetic combinations used by conventional endocrinologists. The reality is that many patients do well on both. (16)
Back to the Patient
Susan was switched to NDT, Natural Desiccated Thyroid, starting with half grain daily and gradually increasing dosage by half grain weekly increments until reaching maintenance dose of 3 grains a day. Susan’s labs at 3 grains showed a suppressed TSH of 0.25, and both the serum T3 and T4 were in normal range. The Serum T3 was 320, and serum T4 was 1.1. More importantly, Susan was now feeling back to her normal self with resolution of hypothyroid symptoms, and no adverse effects of thyroid excess.
Conclusion: Of the 7%-10% of the population suffering from hypothyroidism, most will do well on T4 only thyroid medication such as Levothyroxine with the local endocrinologist. However, a subset (10-20%) of these patients will continue to suffer from low thyroid symptoms, and will do much better on a combination of T3 and T4, either synthetic T3 and T4 at their local endocrinologist, or NDT, natural desiccated thyroid used by integrative medical practitioners. The 5:1 ratio of T4 to T3 seems to be preferred. However, a smaller subset of patients will prefer the 12:1 ratio which can be obtained by adding T4 to NDT, or a synthetic combination of T4 and T3 in the proper ratio.
Jeffrey Dach MD
7450 Griffin Road Suite 180/190
Davie, Florida 33314
956-792-4663
Articles with Related Interest
Which Thyroid is Best, Natural Synthetic or Combination?
Why Natural Thyroid is Better than Synthetic Part One
Why Natural Thyroid is Better Part Two
TSH Suppression Benefits and Adverse Effects
Errors in Modern Thyroid Endocrinology
References
1) Wiersinga, Wilmar M. “Paradigm shifts in thyroid hormone replacement therapies for hypothyroidism.” Nature Reviews Endocrinology 10.3 (2014): 164.
2) Abdalla, Sherine M., and Antonio C. Bianco. “Defending plasma T3 is a biological priority.” Clinical endocrinology 81.5 (2014): 633-641.
3) Escobar-Morreale, Hector F., et al. “Replacement therapy for hypothyroidism with thyroxine alone does not ensure euthyroidism in all tissues, as studied in thyroidectomized rats.” The Journal of clinical investigation 96.6 (1995): 2828-2838.
4) Escobar-Morreale, Héctor F., et al. “Only the combined treatment with thyroxine and triiodothyronine ensures euthyroidism in all tissues of the thyroidectomized rat.” Endocrinology 137.6 (1996): 2490-2502.
5) Surks, Martin I., Alan R. Schadlow, and Jack H. Oppenheimer. “A new radioimmunoassay for plasma L-triiodothyronine: measurements in thyroid disease and in patients maintained on hormonal replacement.” The Journal of clinical investigation 51.12 (1972): 3104-3113.
6) Wiersinga, Wilmar M., et al. “2012 ETA guidelines: the use of L-T4 L-T3 in the treatment of hypothyroidism.” European thyroid journal 1.2 (2012): 55-71.
7) Panicker, Vijay, et al. “Common variation in the DIO2 gene predicts baseline psychological well-being and response to combination thyroxine plus triiodothyronine therapy in hypothyroid patients.” The Journal of Clinical Endocrinology & Metabolism 94.5 (2009): 1623-1629.
8) Hoang, Thanh D., et al. “Desiccated thyroid extract compared with levothyroxine in the treatment of hypothyroidism: a randomized, double-blind, crossover study.” The Journal of Clinical Endocrinology & Metabolism 98.5 (2013): 1982-1990.
9) Biondi, Bernadette, and Leonard Wartofsky. “Combination treatment with T4 and T3: toward personalized replacement therapy in hypothyroidism?.” The Journal of Clinical Endocrinology & Metabolism 97.7 (2012): 2256-2271.
10) Snyder, Scott. “Bioidentical thyroid replacement therapy in practice: Delivering a physiologic T4: T3 ratio for improved patient outcomes with the Listecki-Snyder protocol.” Int J Pharm Compd 16 (2012): 376-380.
11) Escobar-Morreale, Héctor F., José I. Botella-Carretero, and Gabriella Morreale de Escobar. “Treatment of hypothyroidism with levothyroxine or a combination of levothyroxine plus L-triiodothyronine.” Best Practice & Research Clinical Endocrinology & Metabolism 29.1 (2015): 57-75.
12) Schmidt, Ulla, et al. “Peripheral markers of thyroid function: the effect of T4 monotherapy versus T4/T3 combination therapy in hypothyroid subjects in a randomized cross-over study.” Endocrine connections (2013): EC-12.
13) Benvenga, Salvatore. “When thyroid hormone replacement is ineffective?.” Current Opinion in Endocrinology, Diabetes and Obesity 20.5 (2013): 467-477.
14) Samuels, Mary H., et al. “The effects of levothyroxine replacement or suppressive therapy on health status, mood, and cognition.” The Journal of clinical endocrinology and metabolism 99.3 (2014): 843.
15) Hennemann, G., et al. “Thyroxine plus low-dose, slow-release triiodothyronine replacement in hypothyroidism: proof of principle.” Thyroid 14.4 (2004): 271-275.Thyroxine plus low-dose slow-release triiodothyronine replacement in hypothyroidism Hennemann G Thyroid 2004
16) Appelhof, Bente C., et al. “Combined therapy with levothyroxine and liothyronine in two ratios, compared with levothyroxine monotherapy in primary hypothyroidism: a double-blind, randomized, controlled clinical trial.” The Journal of Clinical Endocrinology & Metabolism 90.5 (2005): 2666-2674.
17) Escobar-Morreale, Hector F., et al. “Treatment of hypothyroidism with combinations of levothyroxine plus liothyronine.” The Journal of Clinical Endocrinology & Metabolism 90.8 (2005): 4946-4954.
18) Escobar-Morreale, Héctor F., et al. “Thyroid hormone replacement therapy in primary hypothyroidism: a randomized trial comparing L-thyroxine plus liothyronine with L-thyroxine alone.” Annals of internal medicine 142.6 (2005): 412-424.
19) Wiersinga, Wilmar M., et al. “2012 ETA guidelines: the use of L-T4 L-T3 in the treatment of hypothyroidism.” European thyroid journal 1.2 (2012): 55-71.
20) Saravanan, Ponnusamy, et al. “Partial substitution of thyroxine (T4) with tri-iodothyronine in patients on T4 replacement therapy: results of a large community-based randomized controlled trial.” The Journal of Clinical Endocrinology & Metabolism 90.2 (2005): 805-812.
21) Gullo, Damiano, et al. “Levothyroxine monotherapy cannot guarantee euthyroidism in all athyreotic patients.” PLoS One 6.8 (2011): e22552.
22) J Clin Invest. 1973 May;52(5):1010-7. Effects of replacement doses of sodium L-thyroxine on the peripheral metabolism of thyroxine and triiodothyronine in man. Braverman LE, Vagenakis A, Downs P, Foster AE, Sterling K, Ingbar SH.
23) Desouza, Lynette A., et al. “Thyroid hormone regulates hippocampal neurogenesis in the adult rat brain.” Molecular and Cellular Neuroscience 29.3 (2005): 414-426.
24) Montero-Pedrazuela, Ana, et al. “Modulation of adult hippocampal neurogenesis by thyroid hormones: implications in depressive-like behavior.” Molecular psychiatry 11.4 (2006): 361.
25) Burmeister, Lynn A., John Pachucki, and Donald L. St. Germain. “Thyroid hormones inhibit type 2 iodothyronine deiodinase in the rat cerebral cortex by both pre-and posttranslational mechanisms.” Endocrinology 138.12 (1997): 5231-5237.
26) Beard, John L., et al. “Plasma thyroid hormone kinetics are altered in iron-deficient rats.” The Journal of nutrition 128.8 (1998): 1401-1408.
27) Martínez-Iglesias, Olaia, et al. “Hypothyroidism enhances tumor invasiveness and metastasis development.” PloS one 4.7 (2009): e6428.2017
28) Jonklaas, Jacqueline. “Persistent hypothyroid symptoms in a patient with a normal thyroid stimulating hormone level.” Current opinion in endocrinology, diabetes, and obesity 24.5 (2017): 356.
29) Hennessey, James V., and Ramon Espaillat. “Current evidence for the treatment of hypothyroidism with levothyroxine/levotriiodothyronine combination therapy versus levothyroxine monotherapy.” International journal of clinical practice 72.2 (2018): e13062.
30) Tariq, Anam, et al. “Effects of Long-Term Combination LT4 and LT3 Therapy for Improving Hypothyroidism and Overall Quality of Life.” Southern medical journal 111.6 (2018): 363.
31) Peterson, S. J., et al. “An Online Survey of Hypothyroid Patients Demonstrates Prominent Dissatisfaction.” Thyroid: official journal of the American Thyroid Association (2018).
32) Wiersinga, W. M. “THERAPY OF ENDOCRINE DISEASE: T4 T3 combination therapy: is there a true effect?.” European journal of endocrinology 177.6 (2017): R287.
33) Hannoush, Zeina C., and Roy E. Weiss. “Thyroid hormone replacement in patients following thyroidectomy for thyroid cancer.” Rambam Maimonides medical journal 7.1 (2016).
34) Jonklaas, Jacqueline, et al. “Single Dose T3 Administration: Kinetics and Effects on Biochemical and Physiologic Parameters.” Therapeutic drug monitoring 37.1 (2015): 110.
35) Ling, C., et al. “Does TSH Reliably Detect Hypothyroid Patients?.” Annals of thyroid research 4.1 (2018): 122.
36) Milner, Martin. “Hypothyroidism: Optimizing medication with slow-release compounded thyroid replacement.” International journal of pharmaceutical compounding 9.4 (2005): 268.
36a) Milner, Martin. “Hypothyroidism: optimizing medication with slow-release compounded thyroid replacement.” Townsend Letter: The Examiner of Alternative Medicine 283 (2007): 80-86.
37) Dayan, Colin, and Vijay Panicker. “Management of hypothyroidism with combination thyroxine (T4) and triiodothyronine (T3) hormone replacement in clinical practice: a review of suggested guidance.” Thyroid research 11.1 (2018): 1.
38) Bianco, Antonio C. “Cracking the code for thyroid hormone signaling.” Transactions of the American Clinical and Climatological Association 124 (2013): 26.
39) De Castro, Joao Pedro Werneck, et al. “Differences in hypothalamic type 2 deiodinase ubiquitination explain localized sensitivity to thyroxine.” The Journal of clinical investigation 125.2 (2015): 769.
40) Bianco, Antonio C., and Brian W. Kim. “Deiodinases: implications of the local control of thyroid hormone action.” Journal of Clinical Investigation 116.10 (2006): 2571.
41) Grmek, Jernej, et al. “Usefulness of free thyroxine to free triiodothyronine ratio for diagnostics of various types of hyperthyroidism.” Slovenian Medical Journal 84.5 (2015).
42) Carlé, Allan, et al. “Hypothyroid patients encoding combined MCT10 and DIO2 gene polymorphisms may prefer L-T3 L-T4 combination treatment–data using a blind, randomized, clinical study.” European Thyroid Journal 6.3 (2017): 143-151.
43) Jo, Sungro, et al. “Type 2 deiodinase polymorphism causes ER stress and hypothyroidism in the brain.” The Journal of clinical investigation 129.1 (2019): 230-245.
44) Wang, Xichang, et al. “The Type 2 Deiodinase Thr92Ala Polymorphism Is Associated with Higher Body Mass Index and Fasting Glucose Levels: A Systematic Review and Meta-Analysis.” BioMed research international 2021 (2021).
45) Ahmed, Ziyan, et al. “Improvement of Treatment Resistant Depression in a Patient With Primary Hypothyroidism and Thr92Ala5’Type 2 Deiodinase Gene Polymorphism With Multiple Daily Doses of Triiodothyronine.” Journal of the Endocrine Society 5.Supplement_1 (2021): A937-A937.
46) Ahmed, Ziyan S., et al. “Improvement of depression in a patient with hypothyroidism and deiodinase polymorphism with LT3 Therapy.” Clinical case reports 10.4 (2022): e05651.
47) Kotwal, Anupam, and Donald SA McLeod. “Role of Levothyroxine/Liothyronine Combinations in Treating Hypothyroidism.” Endocrinology and metabolism clinics of North America 51.2 (2022): 243-263.
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
www.drdach.com
Heart Book by Jeffrey Dach
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright (c) 2018 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on October 30th, 2022 by Jeffrey Dach MD
The post Thyroid T3/T4 Combination Therapy vs T4-Monotherapy appeared first on Jeffrey Dach MD.
September 23, 2022
Covid 19 Vaccines a Time for Reassessment

Dr. Scot Youngbloodâs presentation to the San Diego City Council on September 16th, 2022. Covid 19 Vaccines a Time for Reassessment.
=========================
Click Here to View Presentation
=========================
Links and References
1) Presentation video Courtesy of Reopen San Diego
2) PDF of slides: C19-Vaccines-Scot Young blood
Published on September 23rd, 2022 by Jeffrey Dach MD
The post Covid 19 Vaccines a Time for Reassessment appeared first on Jeffrey Dach MD.
July 18, 2022
Hashimoto’s With Normal TSH, When to Treat
Hashimoto’s Thyroiditis with Normal TSH, When to Treat ?
A 15 year old high school student came into the office with her mother with the the diagnosis of Hashimotos thyroid disease with normal TSH. Her thyroid antibodies, anti-thyroglobulin (anti-Glob) and anti-thyroperoxidase (TPO) antibody levels were 425 IU/mL and 350 IU/mL, and the thyroid gland was moderately enlarged (Goiter). Additional laboratory testing showed low vitamin D3 and B12 levels.
Above left image: Hashimotos Thyroiditis Histology Showing Lymphocytic infiltration (black arrows) in thyroid gland courtesy of wikimedia commons
This young lady had been to a number of endocrinologists who declined to treat her with thyroid hormone medication (Levothyroxine), claiming treatment was not necessary. The doctors preferred to wait until thyroid function declines, as determined by elevated TSH which indicates hypothyroidism.
In spite of the normal TSH, the 15 year old was symptomatic with menstrual irregularities, mood disorders, weight gain, acne. In addition she consumed junk food and carbonated sodas on a regular basis.
It is quite true that endocrinologists will NOT TREAT the “Euthyroid Hashimotos patient” (normal TSH). In my opinion, this is an error. In my office, we make a point of offering treatment with thyroid hormone medication to all Euthyroid Hashimoto’s patients, those with TSH in the normal range. This is a practice supported by the medical literature.(1-6)
Over the years of treating Hashimotos patients, we have seen anti-thyroid antibody levels decline in most patients under treatment with TSH suppressive doses of thyroid hormone. We use NDT, natural desiccated thyroid, rather than the T4 only levothyroxine, commonly used by endocrinologists and primary care physicians.
In addition to TSH suppressive doses of thyroid medication, our treatment protocol also includes:
Gluten Free Diet with elimination of junk food and sodas. (25-28)Optimize Vitamin D to upper end of the range. (13-22)Selenium Supplementation if found low on blood testing. (8-10)B12 testing and supplementation when low. (22)Low Dose Iodine supplementation (225-450 mcg per day)LDN (low dose naltrexone ) in selected cases. (30-32)Conclusion: Another Error in Endocrinology is the refusal to treat Euthyroid Hashimotos patients with thyroid medication (NDT or Levothyroxine). Such treatment is supported by massive evidence in the medical literature, and is even more beneficial when combined with Selenium, D3, B12 and a Gluten Free Diet.
Articles with Related Interest
Errors in Modern Endocrinology
TSH Suppression, Benefits and Adverse Side Effects
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
Links and References
euthyroid Hashimoto’s thyroiditis
treatment needs to be started as soon as Hashimotoâs disease is diagnosed.
1) Korzeniowska, Katarzyna, et al. “L-thyroxine stabilizes autoimmune inflammatory process in euthyroid nongoitrous children with Hashimotoâs thyroiditis and type 1 diabetes mellitus.” Journal of Clinical Research in Pediatric Endocrinology 5.4 (2013): 240.
Conclusions: The data demonstrate that treatment with L-T4 in euthyroid pediatric patients with T1DM and AIT stabilizes autoimmune inflammation in the thyroid gland and is to be recommended as soon as the diagnosis is established.
To sum up, our findings also indicate that the treatment of patients with autoimmune polyglandular syndrome type 3a who are euthyroid or subclinically hypothyroid is to be recommended. This treatment needs to be started as soon as Hashimotoâs disease is diagnosed.
Animal models of spontaneous Hashimoto’s autoimmune thyroiditis (HT) show that prophylactic treatment with levothyroxine (LT4) can reduce incidence and degree of lymphocytic infiltration in HT.
2) Padberg, S., et al. “One-year prophylactic treatment of euthyroid Hashimoto’s thyroiditis patients with levothyroxine: is there a benefit?.” Thyroid: official journal of the American Thyroid Association 11.3 (2001): 249-255.
Studies in animal models of spontaneous Hashimoto’s autoimmune thyroiditis (HT) show that prophylactic treatment with levothyroxine (LT4) can reduce incidence and degree of lymphocytic infiltration in HT. The aim of the present study was to clarify whether there is a benefit of prophylactic treatment with LT4 in patients with euthyroid HT with respect to the progression of the autoimmune process.
Twenty-one patients with euthyroid HT were checked for thyroid function (thyrotropin [TSH], free triiodothyronine [FT3], free thyroxine [FT4]), thyroid volume, antibodies (thyroglobulin [Tg-Ab], thyroid peroxidase [TPO-Ab]), and lymphocyte subsets. Peripheral (PBL) and thyroid-derived lymphocytes (TL) were analyzed by triple color flow cytometry. One-half of the patients with euthyroid HT were treated with LT4 for 1 year (n = 10). The other half (n = 11) were never treated with LT4. TL were obtained by fine-needle aspiration biopsy (FNAB). Thirteen healthy subjects (C) without medical history of thyroid disease served as controls concerning PBL, and patients with nontoxic nodular goiter (NG; n = 10) served as controls concerning TL. Thyroid-derived T-helper cells were found more frequently in euthyroid patients with HT compared to patients with NG (p < 0.01).
After 1 year of therapy with LT4, TPO-Abs and B lymphocytes decreased significantly only in the treated group of euthyroid patients with HT (p < 0.05). In contrast, TPO-Abs levels did not change or even increased in untreated euthyroid patients with HT. Thyroid volume did not differ before and after therapy. Prophylactic treatment of euthyroid patients with HT reduced both serological and cellular markers of autoimmune thyroiditis. Therefore, prophylactic LT4 treatment might be useful to stop the progression or even manifestation of the disease. However, the long-term clinical benefit of prophylactic LT4 therapy in euthyroid patients with HT is yet to be established.
Antibody levels decline in most patients on Levothyroxine
3) Schmidt, Matthias, et al. “Long-term follow-up of antithyroid peroxidase antibodies in patients with chronic autoimmune thyroiditis (Hashimoto’s thyroiditis) treated with levothyroxine.” Thyroid: official journal of the American Thyroid Association 18.7 (2008): 755-760.
Background: A number of studies show that the serum levels of antithyroid peroxidase antibodies (TPO-Ab) in patients with Hashimoto’s thyroiditis decline during levothyroxine treatment, but do not provide quantitative data or report the fraction of patients in whom test for TPO-Ab became negative (“normalization percentage”). The objective of the present study was to provide this information.
Methods: This was a retrospective study of TPO-Ab concentrations in 36 women and 2 men (mean age 51 +/- 16 years; range 19-81 years) with Hashimoto’s thyroiditis as defined by the following criteria: elevated plasma TPO-Ab and typical hypoechogenicity of the thyroid in high-resolution sonography at first presentation or during follow-up and low pertechnetate uptake in thyroid scintigraphy. When first studied 17 women and 1 man were not yet taking levothyroxine. The remaining 20 patients were receiving levothyroxine. At initial examination 18 patients had serum thyroid-stimulating hormone (TSH) concentrations above normal. Results of up to eight (mean = 5.8) measurements obtained over a mean period of 50 months while patients were receiving levothyroxine were analyzed. In addition, serum TSH, free triiodothyronine (fT3), and free thyroxine (fT4) were measured, and ultrasound of the neck was performed at each follow-up examination.
Results: In terms of TPO-Ab levels, 35 of 38 patients (92%) had a decrease, 2 patients had undulating levels, and 1 patient had an inverse hyperbolic increase in her TPO-Ab levels. In the 35 patients in whom there were decreasing TPO-Ab values, the mean of the first value was 4779 IU/mL with an SD of 4099 IU/mL. The mean decrease after 3 months was 8%, and after 1 year it was 45%. Five years after the first value, TPO-Ab levels were 1456 +/- 1219 IU/mL, a decrease of 70%. TPO-Ab levels became negative, < 100 IU/mL, in only six patients, a normalization percentage of 16%. There were no correlations between changes in thyroid volume and changes in TPO-Ab.
Conclusion: Serum TPO-Ab levels decline in most patients with Hashimoto’s thyroiditis who are taking levothyroxine, but after a mean of 50 months, TPO-Ab became negative in only a minority of patients.
4) Aksoy, Duygu Yazgan, et al. “Effects of prophylactic thyroid hormone replacement in euthyroid Hashimoto’s thyroiditis.” Endocrine journal 52.3 (2005): 337-343.
Hashimoto’s thyroiditis is the most frequent autoimmune thyroid disease. L-thyroxine therapy can reduce the incidence and alleviate the symptoms of this disease. The aim of this study was to evaluate the effects of prophylactic L-thyroxine treatment on clinical and laboratory findings of patients who were euthyroid at the time of diagnosis. Thirty-three patients who had diagnosis of euthyroid Hashimoto’s thyroiditis were randomized to two groups, one group received prophylactic L-thyroxine treatment and the other was followed-up without treatment. Initial thyroid function tests, autoantibodies, ultrasonography, fine needle aspiration biopsy and peripheral blood lymphocyte subsets were similar in the two study groups. After 15 months of L-thyroxine treatment, there was a significant increase in free T4 and a significant decrease in TSH and anti-thyroglobulin antibody anti-thyroid peroxidase antibody levels. CD8+ cell counts increased in both groups, CD4/CD8 levels decreased significantly because of the increase in CD8+ cell count levels. Though there was no change in cytological findings, ultrasonography showed a decrease in thyroid volume in L-thyroxine receiving patients whereas an increase was detected in patients who were followed without treatment. In conclusion, prophylactic thyroid hormone therapy can be used in patients with Hashimoto’s thyroiditis even if they are euthyroid.
Benefits of Combination Levo and Selenium in Euthyroid Hashimotos pts
5) Krysiak, Robert, and Boguslaw Okopien. “The effect of levothyroxine and selenomethionine on lymphocyte and monocyte cytokine release in women with Hashimoto’s thyroiditis.” The Journal of Clinical Endocrinology & Metabolism 96.7 (2011): 2206-2215.
Design, setting, participants, and intervention:Â We conducted a randomized clinical trial involving a group of 170 ambulatory euthyroid women with recently diagnosed and previously untreated Hashimoto’s thyroiditis and 41 matched healthy subjects. Participants were randomized in a double-blind fashion to receive a 6-month treatment with levothyroxine, selenomethionine, levothyroxine plus selenomethionine, or placebo. One hundred sixty-five patients completed the study.
Main outcome measures:Â Monocyte and lymphocyte release of proinflammatory cytokines and plasma levels of C-reactive protein (CRP) were assessed.
Results: Compared with the control subjects, monocytes and lymphocytes of Hashimoto’s thyroiditis patients released greater amounts of all cytokines studied. Levothyroxine reduced monocyte release of TNF-α, IL-1β, IL-6, and monocyte chemoattractant protein-1, whereas selenomethionine inhibited lymphocyte release of IL-2, interferon-γ, and TNF-α, which was accompanied by a reduction in plasma CRP levels. The decrease in cytokine release and in plasma CRP levels was strongest when both drugs were given together.
Conclusions:Â Despite affecting different types of inflammatory cells, levothyroxine and selenomethionine exhibit a similar systemic antiinflammatory effect in euthyroid females with Hashimoto’s thyroiditis. This action, which correlates with a reduction in thyroid peroxidase antibody titers, may be associated with clinical benefits in the prevention and management of Hashimoto’s thyroiditis, particularly in subjects receiving both agents.
Better IVF outcome in Euthyroid Hashimotos patients when treated with combination LEVO plus anti-inflammatories (ASA and prednisone)6) Revelli, Alberto, et al. “A retrospective study on IVF outcome in euthyroid patients with anti-thyroid antibodies: effects of levothyroxine, acetyl-salicylic acid and prednisolone adjuvant treatments.” Reproductive Biology and Endocrinology 7.1 (2009): 1-6.
The prevalence of ATA among euthyroid, infertile patients was 10.5%, similar to the one reported in euthyroid women between 18 and 45 years. ATA+ patients who did not receive any adjuvant treatment showed significantly poorer ovarian responsiveness to stimulation and IVF results than controls. ATA+ patients receiving LT responded better to ovarian stimulation, but had IVF results as poor as untreated ATA+ women.
Patients receiving LT+ASA+P had significantly higher pregnancy and implantation rates than untreated ATA+ patients (PR/ET 25.6% and IR 17.7% vs. PR/ET 7.5% and IR 4.7%, respectively), and overall IVF results comparable to patients without ATA (PR/ET 32.8% and IR 19%).
Conclusion
These observations suggest that euthyroid ATA+ patients undergoing IVF could have better outcome if given LT+ASA+P as adjuvant treatment. This hypothesis must be verified in further randomized, prospective studies.
–=========================================================
7) Dörr, Helmuth G., et al. “Levothyroxine treatment of euthyroid children with autoimmune Hashimoto thyroiditis: results of a multicenter, randomized, controlled trial.” Hormone research in paediatrics 84.4 (2015): 266-274.
Background: Levothyroxine (L-T4) treatment of euthyroid children with Hashimoto thyroiditis (HT) is a controversial issue. Patients and Methods: We conducted a prospective, randomized, controlled clinical trial. Out of 79 identified euthyroid patients, 59 started the study; 25 patients (21 female, 4 male; age: 11.8 ± 2.3 years) received L-T4 at a mean dose of 1.6 µg/kg (SD, 0.8) daily, and 34 (27 female, 7 male; age: 12.6 ± 1.2 years) were not treated.
Patients developing subclinical hypothyroidism during follow-up (n = 13) were treated with L-T4 and removed from the observation group.
As the main outcome measures, thyroid gland volume (determined by ultrasound) as well as serum levels of TSH, free T4, and antibodies against thyroid peroxidase and thyroglobulin were assessed every 6 months for 36 months. Results: At the start, the mean thyroid volume (standard deviation score, SDS) was 2.5 in the treatment group and 1.6 in the observation group. There was a constant decline in mean thyroid volume (SDS) from 2.13 (month 12) to 1.12 (month 30) in the treated group, with a delta thyroid volume of -1.01 SDS. In the observation group, the mean delta thyroid volume increased to +0.27 SDS. The change of the delta thyroid volume was statistically significantly different between both groups during the 12- and 30-month time points (p < 0.05). L-T4 had no effect on thyroid function and serum thyroid antibodies. Conclusions: L-T4 treatment can decrease the thyroid volume in euthyroid children with HT, but the effect is limited to a definite time period.
Selenium Reduces Antibody Levels
8) Wichman, Johanna, et al. “Selenium supplementation significantly reduces thyroid autoantibody levels in patients with chronic autoimmune thyroiditis: a systematic review and meta-analysis.” Thyroid 26.12 (2016): 1681-1692.
9) Onal, Hasan, et al. “Effects of selenium supplementation in the early stage of autoimmune thyroiditis in childhood: an open-label pilot study.” Journal of Pediatric Endocrinology and Metabolism 25.7-8 (2012): 639-644.
Results:Â Serum TPOAb, TgAb, and thyroid echogenicity were unchanged with Se supplementation. A prominent decrease in thyroid volume was noteworthy; 35% of patients showed a thyroid volume regression rate of > or = 30%.
10) Yu, L., et al. “Levothyroxine monotherapy versus levothyroxine and selenium combination therapy in chronic lymphocytic thyroiditis.” Journal of endocrinological investigation 40.11 (2017): 1243-1250.
11) Pirola, Ilenia, et al. “Selenium supplementation could restore euthyroidism in subclinical hypothyroid patients with autoimmune thyroiditis.” Endokrynologia Polska 67.6 (2016): 567-571.
12) Fan, Yaofu, et al. “Selenium supplementation for autoimmune thyroiditis: a systematic review and meta-analysis.” International journal of endocrinology 2014 (2014).
Vitamin D3 Benefits for Hashimotos
13) Piekarska, MaÅgorzata, et al. “The correlation between vitamin D and autoimmune thyroid functionâshort review.” Journal of Education, Health and Sport 11.9 (2021): 401-408.
14) Vieira, Inês Henriques, DÃrcea Rodrigues, and Isabel Paiva. “Vitamin D and Autoimmune Thyroid DiseaseâCause, Consequence, or a Vicious Cycle?.” Nutrients 12.9 (2020): 2791.
15) Koehler, Viktoria F., Natalie Filmann, and W. Alexander Mann. “Vitamin D status and thyroid autoantibodies in autoimmune thyroiditis.” Hormone and Metabolic Research 51.12 (2019): 792-797.
16) Mazokopakis, Elias E., et al. “Is vitamin D related to pathogenesis and treatment of Hashimotoâs thyroiditis.” Hell J Nucl Med 18.3 (2015): 222-7.
Results: There was a signicant negative correlation only between serum 25(OH)D levels and anti-TPO levels among all 218 HT patients. Also, antiTPO levels were signicantly higher in 186/218 vitamin D decient HT patients compared to 32/218 HT patients with no vitamin D deciency (364±181IU/mL versus 115.8±37.1IU/mL, P<0.0001). Supplementation of CF in 186 vitamin D decient HT patients caused a signicant decrease (20.3%) in serum anti-TPO levels. Although at the end of the 4 months period of the study body mass index (BMI), serum anti-TG and TSH
levels decreased by 2.2%, 5.3% and 4% respectively, these dierences were not signicant. No changes in the sonographic ndings were observed. Conclusions: The majority (85.3%) of the Greek Caucasian patients with HT studied who lived and worked in Crete had low serum 25(OH)D levels inversely correlated
with serum anti-TPO thyroid antibodies. After 4 months of CF supplementation in the 186 HT patients with vitamin D deciency, a signicant decrease (20.3%) of serum anti-TPO levels was found. These findings suggest that vitamin D deciency may be related to pathogenesis of HT and that its supplementation could contribute to the treatment of patients with HT.
17) Chahardoli, Reza, et al. “Can supplementation with vitamin D modify thyroid autoantibodies (Anti-TPO Ab, Anti-Tg Ab) and thyroid profile (T3, T4, TSH) in Hashimotoâs thyroiditis? A double blind, Randomized clinical trial.” Hormone and Metabolic Research 51.05 (2019): 296-301.
‘
18) Krysiak, Robert, Witold Szkróbka, and BogusÅaw OkopieÅ. “The effect of vitamin D on thyroid autoimmunity in levothyroxine-treated women with Hashimotoâs thyroiditis and normal vitamin D status.” Experimental and Clinical Endocrinology & Diabetes 125.04 (2017): 229-233.
Results: There were no significant differences in baseline values between
both study groups. 25-hydroxyvitamin D levels inversely correlated
with titers of thyroid antibodies. No changes in hypothalamic-pituitary-
thyroid axis activity and thyroid antibody titers were observed
in vitamin-naïve patients. Vitamin D increased serum levels of 25-hydroxyvitamin
D, as well as reduced titers of thyroid antibodies. This
effect was more pronounced for thyroid peroxidase than for thyroglobulin
antibodies and correlated with their baseline titers.
Conclusions: Vitamin D preparations may reduce thyroid autoimmunity
in levothyroxine-treated women with Hashimotoâs thyroiditis and
normal vitamin D status.
19) Koehler, Viktoria F., Natalie Filmann, and W. Alexander Mann. “Vitamin D status and thyroid autoantibodies in autoimmune thyroiditis.” Hormone and Metabolic Research 51.12 (2019): 792-797.
20) Fang, Fang, et al. “Vitamin D deficiency is associated with thyroid autoimmunity: results from an epidemiological survey in Tianjin, China.” Endocrine 73.2 (2021): 447-454.
21) Mazokopakis, Elias E., et al. “Is vitamin D related to pathogenesis and treatment of Hashimotoâs thyroiditis.” Hell J Nucl Med 18.3 (2015): 222-7.
Conclusion: The majority (85.3%) of the Greek Caucasian patients with HT studied who lived and worked in Crete had low serum 25(OH)D levels inversely correlated with serum anti-TPO thyroid antibodies. After 4 months of CF supplementation in the 186 HT patients with vitamin D deficiency, a significant decrease (20.3%) of serum anti-TPO levels was found. These findings suggest that vitamin D deficiency may be related to pathogenesis of HT and that its supplementation could contribute to the treatment of patients with HT.
D3 and B12 deficiency in Hashimotos
22) AktaÅ, Hanife Åerife. “Vitamin B12 and vitamin D levels in patients with autoimmune hypothyroidism and their correlation with anti-thyroid peroxidase antibodies.” Medical Principles and Practice 29.4 (2020): 364-370.
Iodine, Selenium, Vitamin D3 Gluten
23) Liontiris, Michael I., and Elias E. Mazokopakis. “A concise review of Hashimoto thyroiditis (HT) and the importance of iodine, selenium, vitamin D and gluten on the autoimmunity and dietary management of HT patients. Points that need more investigation.” Hell J Nucl Med 20.1 (2017): 51-56.
24) Ihnatowicz, Paulina, et al. “The importance of nutritional factors and dietary management of Hashimotoâs thyroiditis.” Annals of agricultural and environmental medicine 27.2 (2020).
Gluten
25) PobÅocki, Jakub, et al. “Whether a Gluten-Free Diet Should Be Recommended in Chronic Autoimmune Thyroiditis or Not?âA 12-Month Follow-Up.” Journal of Clinical Medicine 10.15 (2021): 3240.
During the 12-month follow-up between the CG and the GFDG, no differences
were found in anti-TPO and anti-TG antibodies, fT3 or fT4 levels, except a significant reduction in TSH levels in the GFDG. Additionally, performed analysis between individual appointments presented no significant differences in changes in the median concentrations of anti-TPO, anti-TG or fT3, but confirmed a significant decrease in TSH and showed accessory an increase in fT4 after 12 months in GFDG. Statistical analyses performed separately for both groups indicated a constant reduction of anti-TG concentrations in the GFDG. I
26) Krysiak, Robert, Witold Szkróbka, and BogusÅaw OkopieÅ. “The effect of gluten-free diet on thyroid autoimmunity in drug-naïve women with Hashimotoâs thyroiditis: a pilot study.” Experimental and Clinical Endocrinology & Diabetes 127.07 (2019): 417-422.
27) Wojtas, Natalia, Lidia Wadolowska, and Elżbieta Bandurska-Stankiewicz. “Evaluation of qualitative dietary protocol (diet4hashi) application in dietary counseling in hashimoto thyroiditis: study protocol of a randomized controlled trial.” International journal of environmental research and public health 16.23 (2019): 4841.
28) Agardh, Daniel, et al. “Reduction of tissue transglutaminase autoantibody levels by gluten-free diet is associated with changes in subsets of peripheral blood lymphocytes in children with newly diagnosed coeliac disease.” Clinical & Experimental Immunology 144.1 (2006): 67-75.
==========================
29) Talebi, Sepide, et al. “Trace element status and hypothyroidism: a systematic review and meta-analysis.” Biological trace element research 197.1 (2020): 1-14.
LDN
30) Kim, Yoon Hang John. “Case Report: Reversing Hypothyroidism with Low Dose Naltrexone (LDN).” Multiple sclerosis 3: 4.
31) McDermott, Michael T. “Low-dose naltrexone treatment of Hashimotoâs thyroiditis.” Management of Patients with Pseudo-Endocrine Disorders. Springer, Cham, 2019. 317-326.
32) Neuman, Daniel L., and Andrea L. Chadwick. “Utilization of Low-Dose Naltrexone for Burning Mouth Syndrome: A Case Report.” A&A Practice 15.5 (2021): e01475.
33)Â Hashimotoâs Disease: Your Body Is Not Supposed to Destroy Itself Right?
BY Dana Trentini HypoThyroid MOM
Doctors refuse to treat Hashimotoâs when TSH is normal.
Another major problem is that many traditional doctors refuse to treat patients who test positive for thyroid antibodies, even when they suffer debilitating symptoms, all because their TSH level is ânormalâ. Unfortunately TSH rules above all else in mainstream medicine when it comes to hypothyroidism. You may have Hashimotoâs disease with elevated thyroid antibodies, yet all because the destruction of your thyroid gland has not YET destroyed enough of your gland yet to trigger an abnormal TSH reading, you are refused treatment and forced to cope with your symptoms. End Quote
34) Ãzen, Samim, et al. “Clinical course of Hashimoto’s thyroiditis and effects of levothyroxine therapy on the clinical course of the disease in children and adolescents.” Journal of clinical research in pediatric endocrinology 3.4 (2011): 192.
Levothyroxine therapy may have beneficial effects on the clinical course of the disease and on antibody titers.
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
www.drdach.com
Heart Book by Jeffrey Dach
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
Click Here for: Dr Dachâs Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dachâs Online Store for Natureâs Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician â patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright (c) 2018 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a âfair useâ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on July 18th, 2022 by Jeffrey Dach MD
The post Hashimoto’s With Normal TSH, When to Treat appeared first on Jeffrey Dach MD.
June 30, 2022
Robert Malone MD Texas Senate Testimony
 Robert Malone MD Texas Senate Testimony June 27, 2022, Senate Committee on Health Human Services
Robert Malone MD Texas Senate Testimony June 27, 2022, Senate Committee on Health Human Services
Exerpt:Â Historically Bad Judgement By the FDA: “There Is No Rationale for Vaccinating These Young Children”
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
www.drdach.com
Heart Book by Jeffrey Dach
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
Links and References
https://www.science.org/doi/10.1126/s...
Reynolds, Catherine J., et al. “Immune boosting by B. 1.1. 529 (Omicron) depends on previous SARS-CoV-2 exposure.” Science (2022): eabq1841.
The Omicron, or Pango lineage B.1.1.529, variant of SARS-CoV-2 carries multiple spike mutations with high transmissibility and partial neutralizing antibody (nAb) escape. Vaccinated individuals show protection from severe disease, often attributed to primed cellular immunity. We investigated T and B cell immunity against B.1.1.529 in triple mRNA vaccinated healthcare workers (HCW) with different SARS-CoV-2 infection histories. B and T cell immunity against previous variants of concern was enhanced in triple vaccinated individuals, but magnitude of T and B cell responses against B.1.1.529 spike protein was reduced. Immune imprinting by infection with the earlier B.1.1.7 (Alpha) variant resulted in less durable binding antibody against B.1.1.529. Previously infection-naïve HCW who became infected during the B.1.1.529 wave showed enhanced immunity against earlier variants, but reduced nAb potency and T cell responses against B.1.1.529 itself. Previous Wuhan Hu-1 infection abrogated T cell recognition and any enhanced cross-reactive neutralizing immunity on infection with B.1.1.529.
https://boriquagato.substack.com/p/ju...
just how much are covid cases up in the US? when you adjust for testing levels (which have been dropping rapidly) the US data look ominous el gato malo
Click Here for: Dr Dachâs Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dachâs Online Store for Natureâs Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician â patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright (c) 2018 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a âfair useâ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on June 30th, 2022 by Jeffrey Dach MD
The post Robert Malone MD Texas Senate Testimony appeared first on Jeffrey Dach MD.
June 29, 2022
Peter McCuIIough Co\/id \/accine Update Texas Senate Testimony
 Peter McCullough Covid Vaccine Update Texas Senate Testimony
Peter McCullough Covid Vaccine Update Texas Senate Testimony
by Jeffrey Dach MD
If you are regular reader of this blog, you probably noticed I have taken a break in writing about Covid-19 and the mRNA Vaccines. However, it is worth watching these video excerpts of Peter McCullough MD providing testimony to the Texas Senate June 2022. Dr McCullough is a trained epidemiologist and practicing cardiologist. This is senate testimony under oath. Everything Dr McCullough says is 100% correct and true.
1,000 Papers Published in Medical Literature on Vaccine Injuries and Deaths.Â
50% of vaccine deaths occur within 48 hrs. of the vaccine, and 80% within a week.
The Vaccines cause blood clots, heart damage, neurologic damage, immunologic and hematologic system damage,
As of June 2022, VAERS System shows 13,388 Americans Died after the Vaccine.
Vaccine Deaths satisfy Bradford Hill Criteria of Causality. It is clear and convincing the vaccines are causing deaths.
https://jeffreydachmd.com/wp-content/uploads/2022/06/Peter-McCullough-Vaccines-Causing-Death.mp4
Forty Thousand Deaths After the Vaccine, Efficacy has Waned. The Vaccines have Completely Failed .
June 2022, the World Council for Health calls for global recall of all Covid 19 Vaccines because of 40,000 deaths recorded in multiple databases across the world.
The usual standard for any new product with 50 deaths, it is pulled off the market.
Vaccine efficacy has largely waned. 79% of people with Omicron Variant were fully vaccinated. This is evidence the vaccines have completely failed.
https://jeffreydachmd.com/wp-content/uploads/2022/06/40000-Deaths-Peter-McCullough.mp4Early Treatment Provides 85-95% Risk Reduction in Deaths and Hospitalization.Â
The outcome of hospitalization and death is a product of NOT receiving early treatment.
https://jeffreydachmd.com/wp-content/uploads/2022/06/Peter-McCullough-Texas-Senate-Comm-HEalth-Hum-Sewv-June-2022.mp4
Here is a link to the entire 17 minute senate testimony:
Link to entire 17 minute testimony
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
www.drdach.com
Heart Book by Jeffrey Dach
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
Click Here for: Dr Dachâs Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dachâs Online Store for Natureâs Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician â patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this Article
Copyright (c) 2018 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a âfair useâ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on June 29th, 2022 by Jeffrey Dach MD
The post Peter McCuIIough Co\/id \/accine Update Texas Senate Testimony appeared first on Jeffrey Dach MD.
May 13, 2022
Mortality Reduction in Diabetics with PDE5 Inhibitor Statin Testosterone Combo
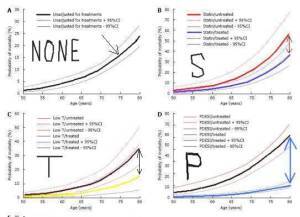 Mortality Reduction in Diabetics with PDE5 Inhibitor, Statin, and Testosterone Combination
Mortality Reduction in Diabetics with PDE5 Inhibitor, Statin, and Testosterone Combination
by Jeffrey Dach MD
While researching nitric oxide and the plant based diet, I came across this 2017 study by Geoffrey Hackett in the World Journal of Diabetes, “Statin, testosterone and phosphodiesterase 5-inhibitor treatments and age related mortality in diabetes.”
Well known complications of Diabetes are peripheral neuropathy, diabetic renal disease, accelerated coronary artery disease, and erectile dysfunction, all related to nitric oxide deficiency commonly found in diabetics.
It is also well known that both testosterone therapy and statin therapy are beneficial for diabetics, providing a reduction in all cause mortality of 20- 60%, depending on the study. This recommendation of prescribing a statin drug for diabetics is regardless of cholesterol levels. In my opinion, this benefit of a statin drug for diabetics is not due to cholesterol lowering effect of the drug. The benefit is due to pleomorphic effects, the anti-inflammatory and anti-microbial effects. See this study by Zhang:
Zhang, Quanwu, et al. “Short-term statin exposure is associated with reduced all-cause mortality in persons with diabetes.” Medical care (2007): 308-314. Conclusions: One to 2-year statin exposure is associated with a 25% to 29% risk reduction in all-cause mortality of the subsequent year in a high-risk diabetes cohort.
Benefits of Testosterone for Diabetics
was demonstrated nicely in this study by Muraleedharan, Vakkat, et al. âTestosterone deficiency is associated with increased risk of mortality and testosterone replacement improves survival in men with type 2 diabetes.â European Journal of Endocrinology 169.6 (2013): 725-733.
Even Greater Benefits For PDE5 Inhibitor Tadalafil (Cialis)
As impressive as the benefits of Testosterone and Statins are for diabetics, the benefit of a PDE5 inhibitor such as Cialis (tadalafil) 5 mg daily, is even greater. This was demonstrated nicely by Dr Geoffrey Hackett in the UK who found profound reduction in mortality in diabetics taking Cialis 5 mg daily.

Above Image Fig 3. courtesy of Hackett shows mortality in Untreated Group (A) labeled NONE (black line and arrow) . Upper Right (B) Labeled S , Red line is untreated group. Blue line is Statin treated group with reduced mortality. Lower Left (C) labeled T. Low Testosterone patients untreated (Black Line) and Treated with Testosterone (Yellow Line). Lower Right (D) Labeled P for PDE5 inhibitor Cialis. Untreated Group Black Line. Cialis Treated Group Blue Line. Note Dramatic separation (Blue Arrows) greater than other two treatment charts.
All three treatments together in Combination:
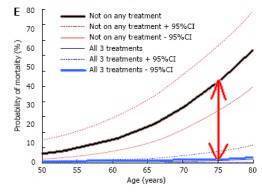
Left Chart Courtesy of Hackett (E): Black Line is Mortality of Untreated Group. Blue Line is Mortality of Treated Group using all three modalities, statin, testosterone and PDE5 inhibitor. Note dramatic reduction in mortality denoted by Red Arrows in the Blue Treated Group.
What is the connection to Nitric Oxide, Erectile Dysfunction and PDE5 inhibitors?
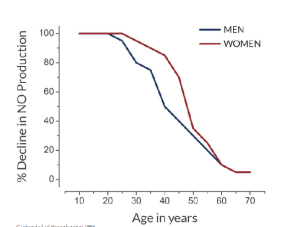 Nitric Oxide production declines with age: (see the left chart). This is directly related to erectile dysfunction, endothelial dysfunction and and vascular disease.
Nitric Oxide production declines with age: (see the left chart). This is directly related to erectile dysfunction, endothelial dysfunction and and vascular disease.
The key messenger molecule producing vasodilatation is cGMP, which is downstream to Nitric Oxide. The PDE5 inhibitors do not directly increase nitric oxide. They prevent degradation of the cyclic guanosine monophosphate (cGMP) induced by nitric oxide, thus inducing vasodilatation, and relieving erectile dysfunction.
The mechanism of action of sildenafil involves the protection of cyclic guanosine monophosphate (cGMP) from degradation by cGMP-specific phosphodiesterase type 5 (PDE5) in the corpus cavernosum. Nitric oxide (NO) in the corpus cavernosum of the penis binds to guanylate cyclase receptors, which results in increased levels of cGMP, leading to smooth muscle relaxation (vasodilation) of the intimal cushions of the helicine arteries. This smooth muscle relaxation leads to vasodilation and increased inflow of blood into the spongy tissue of the penis, causing an erection. Robert F. Furchgott, Ferid Murad and Louis Ignarro won the Nobel Prize in Physiology or Medicine in 1998 for their independent study of the metabolic pathway of nitric oxide in smooth muscle vasodilation. Endquote reference link
PDE5 inhibitors for BPH and Chronic Prostatitis
In addition to their benefit for diabetics, Cialis (tadalafil) 5 mg daily has been found beneficial for BPH Benign Prostatic Hypertrophy and Chronic Prostatitis patients.
PDE5 Inhibitors for Cognitive Function and Neuropathy
Increases in micro circulation, blood flow induced by PDE5 inhibitors provides benefit in peripheral neuropathy and cognitive function.
Conclusion: The dramatic benefit of PDE5 inhibition with tadalafil in diabetes is even greater when used in combination with testosterone and statin drugs.
Jeffrey Dach MD
Articles with Related Interest
Links and References
Testosterone Reduces Mortality in Diabetics
Muraleedharan, Vakkat, et al. âTestosterone deficiency is associated with increased risk of mortality and testosterone replacement improves survival in men with type 2 diabetes.â European Journal of Endocrinology 169.6 (2013): 725-733.
Low Testosterone Associated with Increased Mortality
Testosterone Found Beneficial for Diabetics
Testosterone Reduces Mortality
Statins Reduce Mortality in Diabetics
Maqbool, Mudasir, and Imran Gani. “Utilization of Statins in Reducing Comorbidities of Diabetes Mellitus: A Systematic Review.” Journal of Pharmacy Practice and Community Medicine 4.4 (2018). Conclusion: An overwhelming amount of data
that confirm the morbidity and mortality benefit of statin therapy in diabetes mellitus have been reported, both in primary and secondary prevention settings.
Zhang, Quanwu, et al. “Short-term statin exposure is associated with reduced all-cause mortality in persons with diabetes.” Medical care (2007): 308-314. Conclusions: One to 2-year statin exposure is associated with a 25% to 29% risk reduction in all-cause mortality of the subsequent year in a high-risk diabetes cohort.
Fung, Colman Siu Cheung, et al. “Statin use reduces cardiovascular events and all-cause mortality amongst Chinese patients with type 2 diabetes mellitus: a 5-year cohort study.” BMC cardiovascular disorders 17.1 (2017): 1-9.
Chen, Po-Hsun, et al. “Effects of statins on all-cause mortality at different low-density-lipoprotein cholesterol levels in Asian patients with type 2 diabetes.” Current medical research and opinion 34.11 (2018): 1885-1892.
PDE5 Mechanism of action
Corbin, J. D. “Mechanisms of action of PDE5 inhibition in erectile dysfunction.” International journal of impotence research 16.1 (2004): S4-S7.
Kass, David A., et al. “Phosphodiesterase regulation of nitric oxide signaling.” Cardiovascular research 75.2 (2007): 303-314.
Burnett, Arthur L. “Phosphodiesterase 5 mechanisms and therapeutic applications.” The American journal of cardiology 96.12 (2005): 29-31.
https://www.liquisearch.com/sildenafi...
The mechanism of action of sildenafil involves the protection of cyclic guanosine monophosphate (cGMP) from degradation by cGMP-specific phosphodiesterase type 5 (PDE5) in the corpus cavernosum. Nitric oxide (NO) in the corpus cavernosum of the penis binds to guanylate cyclase receptors, which results in increased levels of cGMP, leading to smooth muscle relaxation (vasodilation) of the intimal cushions of the helicine arteries. This smooth muscle relaxation leads to vasodilation and increased inflow of blood into the spongy tissue of the penis, causing an erection. Robert F. Furchgott, Ferid Murad and Louis Ignarro won the Nobel Prize in Physiology or Medicine in 1998 for their independent study of the metabolic pathway of nitric oxide in smooth muscle vasodilation.
Sildenafil is a potent and selective inhibitor of cGMP-specific phosphodiesterase type 5 (PDE5), which is responsible for degradation of cGMP in the corpus cavernosum. The molecular structure of sildenafil is similar to that of cGMP and acts as a competitive binding agent of PDE5 in the corpus cavernosum, resulting in more cGMP and better erections.
Phosphodiesterase Inhibitors and Diabetes
Santi, Daniele, et al. “Therapy of endocrine disease: effects of chronic use of phosphodiesterase inhibitors on endothelial markers in type 2 diabetes mellitus: a meta-analysis.” European journal of endocrinology 172.3 (2015): R103-R114.
Anderson, Simon G., et al. “Phosphodiesterase type-5 inhibitor use in type 2 diabetes is associated with a reduction in all-cause mortality.” Heart 102.21 (2016): 1750-1756.
Cardiac risk factors and prevention
Phosphodiesterase type-5 inhibitor use in type 2 diabetes is associated with a reduction in all-cause mortality
Simon G Anderson1,2, David C Hutchings1, Mark Woodward2,3, Kazem Rahimi2, Martin K Rutter4,5, Mike Kirby6, Geoff Hackett7, Andrew W Trafford1, Adrian H Heald8,9
Abstract
Objective Experimental evidence has shown potential cardioprotective actions of phosphodiesterase type-5 inhibitors (PDE5is). We investigated whether PDE5i use in patients with type 2 diabetes, with high-attendant cardiovascular risk, was associated with altered mortality in a retrospective cohort study.
Research design and methods Between January 2007 and May 2015, 5956 men aged 40â89â years diagnosed with type 2 diabetes before 2007 were identified from anonymised electronic health records of 42 general practices in Cheshire, UK, and were followed for 7.5â years. HRs from multivariable survival (accelerated failure time, Weibull) models were used to describe the association between on-demand PDE5i use and all-cause mortality.
https://heart.bmj.com/content/102/21/...
Anderson, Simon G., et al. “Phosphodiesterase type-5 inhibitor use in type 2 diabetes is associated with a reduction in all-cause mortality.” Heart 102.21 (2016): 1750-1756.
Of the total cohort, we identiï¬ed men who had received a pre-
scription of a PDE5i (sildenaï¬l, vardenaï¬l or tadalaï¬l) prior to
1 January 2007 and at least once, up to 30 June 2015.
A total of 5956 men with known type 2 diabetes aged 40â
89 years were identiï¬ed at cohort entry date of 1 January 2007.
Of the total, 1359 (22.8%) received a PDE5i, prescribed a
All-cause mortality
Participants were followed up for a mean of 7.5 years (range
0.4â8.5 years). From the same background population, a
random (reference) sample of 32 330 men without diabetes or
PDE5i use, followed up for a mean 8.3 years, had mortality
rates of 4.8 (4.5 to 5.0) per 100 person-years. Fewer deaths (age
adjusted) occurred among PDE5i users with type 2 diabetes:
248 (19.1%) versus non-users (1170, (23.8%); 2=12.47,
p=0.0004).
Men on treatment with a PDE5i had a 31% lower risk of all-
cause mortality compared with non-users
Among those with a prior history of MI (n=1031), there were
fewer deaths in those previously treated with a PDE5i compared
with those who were never treated (25.7% (49/191) vs 40.1%
(337/840)).
Results Compared with non-users, men who are prescribed PDE5is (n=1359) experienced lower percentage of deaths during follow-up (19.1% vs 23.8%) and lower risk of all-cause mortality (unadjusted HR=0.69 (95% CI: 0.64 to 0.79); p<0.001)). The reduction in risk of mortality (HR=0.54 (0.36 to 0.80); p=0.002) remained after adjusting for age, estimated glomerular filtration rate, smoking status, prior cerebrovascular accident (CVA) hypertension, prior myocardial infarction (MI), systolic blood pressure, use of statin, metformin, aspirin and β-blocker medication. PDE5i users had lower rates of incident MI (incidence rate ratio (0.62 (0.49 to 0.80), p<0.0001) with lower mortality (25.7% vs 40.1% deaths; age-adjusted HR=0.60 (0.54 to 0.69); p=0.001) compared with non-users within this subgroup. Conclusion In a population of men with type 2 diabetes, use of PDE5is was associated with lower risk of overall mortality and mortality in those with a history of acute MI.
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! BEST !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
Hackett, Geoffrey, et al. “Statin, testosterone and phosphodiesterase 5-inhibitor treatments and age related mortality in diabetes.” World journal of diabetes 8.3 (2017): 104. We show that statins, PDE5I and TRT reduce mortality in diabetes. PDE5I, alone and with the other treatments significantly alter age related mortality in diabetic men. METHODS We studied 857 diabetic men screened for the BLAST study, stratifying them (mean follow-up = 3.8 years) into: (1) Normal T levels/untreated (total T > 12 nmol/L and free T > 0.25 nmol/L), Low T/untreated and Low T/treated; (2) PDE5I/untreated and PDE5I/treated; and (3) statin/untreated and statin/treated groups. The relationship between age and mortality, alone and with T/TRT, statin and PDE5I treatment was studied using logistic regression. Mortality probability and 95%CI were calculated from the above models for each individual.
Four PDE5i are currently FDA approved for the
treatment of ED:
sildenafil (Viagra®),
tadalafil (Cialis®),
vardenafil (Levitra®, Staxyn®), and
avanafil (Stendra®).
Drug Time to Onset Duration of
Avanafil 15 minutes 6 hours
Vardenafil 20-30 minutes 8-12 hours
Sildenafil 30-60 minutes 2-4 hours
Tadalafil 60-120 minutes 36 hours
Activity Onset Delayed by High Fat Meal
Yes
Yes
Yes
No
Only tadalafil is indicated for daily dosing, all others are dosed as needed prior to sexual
activity. Pharmacodynamically, these medications differ in their time to onset and duration of activity5,6,7,8
PDE5 inhibitors for Diabetics with Peripheral Neuropathy
https://pubmed.ncbi.nlm.nih.gov/16939...
Hackett G. PDE5 inhibitors in diabetic peripheral neuropathy. Int J Clin Pract. 2006 Sep;60(9):1123-6. doi: 10.1111/j.1742-1241.2006.01087.x. PMID: 16939556.
Abstract
Peripheral neuropathy is the most common complication of diabetes. This paper reviews the case histories of five patients with diabetic peripheral neuropathy or severe peripheral vascular disease who reported improvement in their symptoms when treated with regular or daily dosing with phosphodiesterase type 5 inhibitors (PDE5Is). These patients had been previously treated with PDE5Is for erectile dysfunction (ED) and not responded to on-demand therapy with a PDE5I at maximal recommended dose. This improvement is likely to be due to the known benefit of these drugs on endothelial dysfunction via an improvement of blood supply to the vasa nervorum. These cases suggest that further research is indicated to evaluate the potential use of PDE5Is in the treatment and prevention of diabetic peripheral neuropathy, particularly as these drugs are already licensed to treat ED, which occurs in around 50% of male diabetics.
How I reversed my Levaquin-induced neuropathy with PDE5 Inhibitors from neuropathy
How I reversed my Levaquin-induced neuropathy with PDE5 Inhibitors
In 2015, I developed a horrible, nearly 2 year-long status of being clinically disabled due to only 2x pills of Levaquin which started a chain reaction in my body. Since that time, I developed abnormal sweating in my feet/hands, episodic pain and more, which got worse after my doctor told me my fasting blood glucose was borderline pre-diabetic; Levaquin, like other FQs, appears to cause significant dysglycemia (Friedrich and Dougherty 2004, Singh and Jacob 2008, Kelesidis and Canseco 2009) Dysglycemia is a broad term that refers to an abnormality in blood sugar stability, which is what I had, post-Levaquin. According to Telfer (2014), Fluoroquinolones seem to induce intracellular magnesium deficiency, as the 3-carboxyquinolone substructure of FQs is metal-cleating, and 6-fluoro substituent on the pharmacophore gives rise to sufficient lipophilicity that the drugs can dissolve in and penetrate cell membranes. It has also been suggested that intracellular fluoroquinolones can exist as a magnesium complex! Cellular Diffusion and/or Active Transport of such a complex would deplete Magnesium from the cells. (Lecomte et al., 1994; Bensikaddour, 2008) The effects of fluoroquinolones on intracellular magnesium levels might be considered to be almost cumulative, and slow to reverse overall. (Jahnen-Dechent and M. Ketteler, 2012) . Magnesium affects blood sugar stability, so there was the cause.
Neurological workup was initially unremarkable, but followups showed reduced Nerve Velocity in my feet, reduced nerve density and more. The pain started getting worse, with being unable to tolerate clothing or heat. The doctor wanted to prescribe me the usual cocktails of medications to ‘hide’ the pain. No thanks – I’ll use my scientific background to see about alternative treatments.
Hello ED medications! (PDE5s)
PDE5 Inhibitors, like Viagra, improve neuropathy in human studies, as well as animal studies. (Wang et al., 2017; 2016; 2015; 2011; Mostafa, 2008; Peixoto et al., 2015; Vlachopoulos et al., 2009; Hackett, 2006; Mehmet Fatih Korkmaz et al., 2016; etc) This behavior was described as early as 2002 (Sairam and McNicholas, 2002).
PN symptoms in Fluroquoinoline Patients are more or less the same in Diabetic Patients, as PN initially manifests itself as mitochondrial dysfunction.
PDE5Iâs are showing other benefits, such as increased antioxidant status in humans, cardioprotection, and more.
According to Hackett (2006), 5 patients who were prescribed different PDE5Is showed dramatic results within 90 days, with some of the patients showing a nearly complete reversal of neuropathic pain. However, their T2D was quite advanced, so keep that in mind.
The mechanisms behind PDE5I treatments are well documented; Tadalafil treatment improves motor and sensory conduction velocities in the sciatic nerve and peripheral thermal sensitivity, increased myelin thickness, enhances Nerve Growth Factor, regional blood flow in Sciatic Nerve Tissue, and more. (Wang, et al., 2016; 2017). Daily dosages of Tadalafil for a period of 90 days will likely reverse early-to-moderate stages of Neuropathy.
Going over the Pharmacodynamics of the PDE5is, Sildenafil (Viagra) has a biological half-life of 4 hours, which is likely /too/ short for effective treatment. Tadalafil has a biological half-life of 17 hours, with a great safety profile. However, Tadalafil, unlike Sildenafil, has no absorption issues when combined with food, etc. (Nichols, Muirhead and Harness, 2002), so Tadalafil is likely a better medication for treatment.
I started taking Tadalafil every 48 hours for about a month. Within the first week, my feet were feeling much better, 2 weeks later, my feet were able to sweat like normal. The pain was reduced by at least 60% on week 2. However, I had to start taking antiacids because the Tadalafil was giving me horrible acid reflux. I continued to take it for about 2 months.
A few months later, I visited my neurologist and demanded another full panel. Nerve Conduction Velocity had improved so much that is was within the ‘normal’ range for my peripheral nerves. Punch biopsy showed increased density as well. I was no longer in any pain, really, except for the occasional pins-and-needles feeling when my feet are just too cold for being outside in the winter.
If you are a male and have neuropathy from Diabetes or something else, you could ask your doctor to write you a prescription for a PDE5 and see if it helps you. I don’t know if women could take PDE5s.
Citations;
â Sairam K, McNicholas T. Sildenafil in diabetic peripheral neuropathy. Br J Diabetes Vasc Dis 2002
â Korkmaz MF, Parlakpinar H, Ceylan MF, et al. The Effect of Sildenafil on Recuperation from Sciatic Nerve Injury in Rats. Balkan Med J. 2016;33(2):204â211. doi:10.5152/balkanmedj.2016.14701
â Wang L, Chopp M, Szalad A, Lu X, Jia L, Lu M, Zhang RL, Zhang ZG. Tadalafil Promotes the Recovery of Peripheral Neuropathy in Type II Diabetic Mice. PLoS One. 2016
â Wang L, Chopp M, Szalad A, Liu Z, Bolz M, Alvarez FM, Lu M, Zhang L, Cui Y, Zhang RL, Zhang ZG. Phosphodiesterase-5 is a therapeutic target for peripheral neuropathy in diabetic mice. Neuroscience. 2011
â L. Wang, M. Chopp, A. Szalad, Z. Liu, M. Bolz, F.M. Ãlvarez, M. Lu, L. Zhang, Y. Cui, R.L. Zhang, and Z.G. Zhang, Phosphodiesterase-5 is a therapeutic target for peripheral neuropathy in diabetic mice, Neuroscience, 193, (399), (2011).
â Lei Wang, Michael Chopp, and ZhengGang Zhang, PDE5 inhibitors promote recovery of peripheral neuropathy in diabetic mice, Neural Regeneration Research, 12, 2, (218), (2017).
â Christina Alves Peixoto, Ana Karolina Santana Nunes, and Ana Garcia-Osta, Phosphodiesterase-5 Inhibitors: Action on the Signaling Pathways of Neuroinflammation, Neurodegeneration, and Cognition, Mediators of Inflammation, 10.1155/2015/940207, 2015, (1-17), (2015).
â Lei Wang, Michael Chopp, Alexandra Szalad, LongFei Jia, XueRong Lu, Mei Lu, Li Zhang, Yi Zhang, RuiLan Zhang, Zheng Gang Zhang and Julie A. Chowen, Sildenafil Ameliorates Long Term Peripheral Neuropathy in Type II Diabetic Mice, PLOS ONE, 10, 2, (e0118134), (2015).
â Taymour Mostafa, Oral Phosphodiesterase Type 5 Inhibitors: Nonerectogenic Beneficial Uses, The Journal of Sexual Medicine, 5, 11, (2502-2518), (2008).
â C. Vlachopoulos, D. Terentes-Printzios, N. Ioakeimidis, K. Rokkas, and C. Stefanadis, â PDE5 Inhibitors in Non-Urological Conditionsâ, Current Pharmaceutical Design (2009) 15: 3521. https://doi.org/10.2174/1381612097892...
â Duranti G, Ceci R, Sgrò P, Sabatini S, Di Luigi L. Influence of the PDE5 inhibitor tadalafil on redox status and antioxidant defense system in C2C12 skeletal muscle cells. Cell Stress Chaperones. 2017;22(3):389â396. doi:10.1007/s12192-017-0778-9
– The phosphodiesterase 5 inhibitor sildenafil stimulates angiogenesis through a protein kinase G/MAPK pathway. Pyriochou A, Zhou Z, Koika V, Petrou C, Cordopatis P, Sessa WC, Papapetropoulos A. J Cell Physiol. 2007 Apr;211(1):197-204.
â Pauls MM, Moynihan B, Barrick TR, Kruuse C, Madigan JB, Hainsworth AH, Isaacs JD. The effect of phosphodiesterase-5 inhibitors on cerebral blood flow in humans: A systematic review. J Cereb Blood Flow Metab. 2018 Feb;38(2):189-203.
daily tadalafil 5 mg, and L-arginine 2500.
https://www.ncbi.nlm.nih.gov/pmc/arti...
Gallo, Luigi, Stefano Pecoraro, and Pasquale Sarnacchiaro. “Adjuvant daily therapy with L-arginine 2,500 mg and tadalafil 5 mg increases efficacy and duration of benefits of low-intensity extracorporeal shock wave therapy for erectile dysfunction: A prospective, randomized, single-blinded study with 1-year follow-up.” Investigative and Clinical Urology 63.1 (2022): 83.
Purpose: To investigate a therapeutic protocol for erectile dysfunction (ED) based on the combination of low-intensity extracorporeal
shock wave therapy (Li-ESWT), tadalafil, and L-arginine.
Materials and Methods: Recruited patients completed the International Index of Erectile Function erectile function domain (IIEFEF)
and the Erection Hardness Score (EHS) questionnaires at baseline and were randomly assigned in two groups: A (treatment
group) and B (control group). Men in both groups received six weekly applications of Li-ESWT. Group A was prescribed adjuvant
oral therapy with tadalafil 5 mg and L-arginine 2,500 mg. Follow-up visits were scheduled 1, 6, and 12 months after the last Li-ESWT
application. At each follow-up visit, the IIEF-EF and EHS questionnaires were administered again. The main outcome measures
were the changes from baseline to every follow-up visit in IIEF-EF and EHS scores.
Results: The mean IIEF-EF score in group A was 16.0±4.0, 24.8±3.4, 23.3±4.6, and 21.6±5.5 at baseline, 1, 6, and 12 months of
follow-up, respectively, whereas in group B the mean IIEF-EF score was 16.5±4.1, 22.7±4.2, 21.5±4.5, and 19.5±4.9, respectively.
We reported an increase in the mean EHS score in group A from 2.07±0.72 at baseline to 3.39±0.59, 3.17±0.67, and 2.98±0.72 at 1,
6, and 12 months, respectively, and in group B from 2.12±0.80 at baseline to 3.07±0.78 and 2.95±0.76 at 1 and 6 months, respectively.
Conclusions: Adjuvant daily therapy with L-arginine 2,500 mg and tadalafil 5 mg was safe and effective in increasing the efficacy
and the duration of benefits of Li-ESWT.
https://onlinelibrary.wiley.com/doi/f...
ElâWakeel, L. M., et al. “Efficacy and tolerability of sildenafil/lâarginine combination relative to sildenafil alone in patients with organic erectile dysfunction.” Andrology 8.1 (2020): 143-147.
Randomized controlled study with two parallel groups of erectile dysfunction patients; One group received sildenafil 50 mg every other day, while the other group received a combination of sildenafil (every other day)/l-arginine on a daily base. Efficacy was assessed using International Index of Erectile Function-5 score at the baseline and after 8 weeks. Side effects were evaluated across the two groups.
Results
The mean age was 56.3 ± 5 and 56.2 ± 4.4 years in sildenafil and combination groups, respectively. International Index of Erectile Function-5 score was comparable between the two groups at the baseline (p value 0.44). International Index of Erectile Function-5 score was improved from 15.3 ± 2.5 at baseline to 19.2 ± 2.3 after treatment, and this was statistically significant with p value <0.0001. The score was slightly better in combination group in which the average International Index of Erectile Function-5 score was (19.8 ± 2.2) vs. (18.5 ± 2.3) in sildenafil group with p value 0.05. Side effects were more or less the same between the two groups except for gastritis which was more common on combination group.
Conclusion
Adding l-arginine to sildenafil demonstrated more efficacy than sildenafil alone for treatment of erectile dysfunction patients.
Mirone, Vincenzo, et al. “A new original nutraceutical formulation ameliorates the effect of Tadalafil on clinical score and cGMP accumulation.” Archivio Italiano di Urologia e Andrologia 93.2 (2021): 221-226.
https://jamanetwork.com/journals/jama...
Risk of Ocular Adverse Events Associated With Use of Phosphodiesterase 5 Inhibitors in Men in the US
Mahyar Etminan, PharmD, MSc1,2,5; Mohit Sodhi, MSc1,3; Frederick S. Mikelberg, MD1; et al
Chronic Pelvic Pain Syndrome
https://tau.amegroups.com/article/vie...
Pineault, Kevin, et al. “Phosphodiesterase type 5 inhibitor therapy provides sustained relief of symptoms among patients with chronic pelvic pain syndrome.” Translational Andrology and Urology 9.2 (2020): 391.
Contributions: (I) Conception and design: K Pineault, AS Herati; (II) Administrative support: AS Herati; (III) Provision of study materials or patients: K Pineault, AS Herati; (IV) Collection and assembly of data: All authors; (V) Data analysis and interpretation: K Pineault, S Ray; (VI) Manuscript writing: all authors; (VII) Final approval of manuscript: All authors.
Correspondence to: Amin S. Herati, MD. Department of Urology, The James Buchanan Brady Urological Institute, Johns Hopkins University School of Medicine, Park Building 217, 600 North Wolfe St., Baltimore, MD 21287, USA. Email: aherati1@jhmi.edu.
A total of 25 patients (mean age 44.4±12.9 years) met study criteria. The mean duration of PDE5i therapy was 1.3±1.6 years. Continued use of daily PDE5is was associated with significant decreases in total CPSI, pain, urinary symptom and quality of life scores [total CPSI: â12.8, standard deviation (SD) 9.5; pain: â6.1, SD 4.1; urinary symptoms: â2.4, SD 2.1; quality of life: â4.5, SD 3.9; P<0.001].
Conclusions: This prospective data suggests that PDE5i therapy is associated with durable decreases in CP/CPPS symptoms past 3 months.
Benelli, Andrea, et al. “Once-daily 5 mg tadalafil oral treatment for patients with chronic prostatitis/chronic pelvic pain syndrome.” Therapeutic Advances in Urology 10.12 (2018): 377-381.
DemirtaÅ, Abdullah, et al. “Is Tadalafil an Effective Treatment Option for Interstitial Cystitis/Painful Bladder Syndrome? A Report of a Challenging Case.” Cureus 13.7 (2021).
BPH
https://www.ncbi.nlm.nih.gov/pmc/arti...
Hatzimouratidis, Konstantinos. “A review of the use of tadalafil in the treatment of benign prostatic hyperplasia in men with and without erectile dysfunction.” Therapeutic Advances in Urology 6.4 (2014): 135-147. Tadalafil 5 mg once daily has been approved for the treatment of men with LUTS with or without comorbid ED.
Singh, Sanket Narayan, et al. “Comparing the effect of Alpha blocker (Silodosin) and Phosphodiesterase type 5 inhibitor (Tadalafil) in benign prostate hyperplasia patients with lower urinary tract symptoms: a single centre study.” International Surgery Journal 5.5 (2018): 1866-1872.
Casabé, Adolfo, et al. “Efficacy and safety of the coadministration of tadalafil once daily with finasteride for 6 months in men with lower urinary tract symptoms and prostatic enlargement secondary to benign prostatic hyperplasia.” The Journal of urology 191.3 (2014): 727-733.
https://link.springer.com/article/10....
Cai, Zhonglin, Jianzhong Zhang, and Hongjun Li. “Two birds with one stone: regular use of PDE5 inhibitors for treating male patients with erectile dysfunction and cardiovascular diseases.” Cardiovascular Drugs and Therapy 33.1 (2019): 119-128.
PDE5 for Neurologic and Cognitive Function
Peixoto, Christina Alves, Ana Karolina Santana Nunes, and Ana Garcia-Osta. “Phosphodiesterase-5 inhibitors: action on the signaling pathways of neuroinflammation, neurodegeneration, and cognition.” Mediators of Inflammation 2015 (2015).
Peixoto, Christina A., Ana KS Nunes, and Catarina Rapôso. “The role of NO/cGMP signaling on neuroinflammation: a new therapeutic opportunity.” Mechanisms of neuroinflammation (2017): 167-208.
Nabavi, Seyed Mohammad, et al. “Phosphodiesterase inhibitors say NO to Alzheimer’s disease.” Food and Chemical Toxicology 134 (2019): 110822.
Ben Aissa, Manel, et al. “Targeting NO/cGMP signaling in the CNS for neurodegeneration and Alzheimerâs disease.” Current medicinal chemistry 23.24 (2016): 2770-2788.
de Santana Nunes, Ana Karolina, et al. “Sildenafil (Viagra®) prevents and restores LPS-induced inflammation in astrocytes.” Neuroscience Letters 630 (2016): 59-65.
França, Maria Eduarda Rocha, et al. “Tadalafil restores long-term memory and synaptic plasticity in mice with hepatic encephalopathy.” Toxicology and Applied Pharmacology 379 (2019): 114673.
Wang, Lei, Michael Chopp, and Zheng Gang Zhang. “PDE5 inhibitors promote recovery of peripheral neuropathy in diabetic mice.” Neural regeneration research 12.2 (2017): 218.
da Rocha Araújo, Shyrlene Meiry, et al. “Effect of sildenafil on neuroinflammation and synaptic plasticity pathways in experimental autoimmune encephalomyelitis.” International Immunopharmacology 85 (2020): 106581.
Duarte-Silva, Eduardo, et al. “Phosphodiesterase-5 inhibitors: Shedding new light on the darkness of depression?.” Journal of Affective Disorders 264 (2020): 138-149.
El-Bakly, Wesam, et al. “The efficacy and underlying mechanism of phosphodiesterase-5 inhibitors in preventing cognitive impairment and Alzheimer pathology: A systematic review of animal studies.” Behavioural Brain Research 372 (2019): 112004.
Published on May 13th, 2022 by Jeffrey Dach MD
The post Mortality Reduction in Diabetics with PDE5 Inhibitor Statin Testosterone Combo appeared first on Jeffrey Dach MD.
February 15, 2022
More Deceptive Drug Marketing from the New York Times
 More Deceptive Drug Marketing from the New York Times
More Deceptive Drug Marketing from the New York Times
by Jeffrey Dach MD
A number of friends and family members have brought to my attention a New York Times article by David Leonhardt Feb 14, 2022 entitled, “Protecting the Vulnerable” from Covid.(1)Â This sounds a lot like the Great Barrington Declaration of Kulldorff, Bhattacharya and Gupta, three previously eminent epidemiologists from top academic centers until Collins and Fauci at the NIH blacklisted their careers:Â Here is a quote from Leonhardt:
“Good morning. We offer a guide to protecting vulnerable people â the elderly, immunocompromised and unvaccinated â from Covid…Today’s newsletter focuses on five steps that can help protect the vulnerable as society moves back toward normal…At this point in the pandemic, there is a strong argument that a targeted approach â lifting restrictions while taking specific measures to protect the vulnerable â can maximize public health.”
Next Leonhardt shows a chart based on CDC data showing 40-50 times less rate of hospitalization for the vaccinated compared to the unvaccinated. How was data obtained? What are the biases. Is this accurate data? Can we trust the CDC knowing they have falsified data for two years, inflating numbers of Covid deaths, and inflating numbers of positive PCR tests (cranking up the amplification cycle threshold)?
Can the CDC Be Trusted ?
According to Vinay Prasad February 14, 2022 Tablet Magazine in his article How the CDC Abandoned Science. Dr Prasad writes, the CDC is not impartial. They have been captured by the political system. I add here, captured by the drug industry, and can not be trusted. Here is the quote:
So why does the supposedly impartial CDC push weak or flawed studies to support the administrationâs pandemic policy goals? The cynical answer is that the agency is not in fact impartial (and thus not sufficiently scientific), but captured by the countryâs national political system. That answer has become harder to avoid. This is a precarious situation, as it undermines trust in federal agencies and naturally leads to a trust vacuum, in which Americans feel forced to cast about in a confused search for alternative sources of information. Once that trust is broken, itâs not easily regained. (27)
Contradictory Data from Other Countries
Does this CDC data reflect the same data in other countries, or is this data contradicted by other countries such as Scotland, UK, Iceland and Israel ? For example, in Scotland, January data shows the vaccinated were twice as likely get COVID infection, and twice as likely to be hospitalized with Covid compared to the UN-vaccinated. This is the opposite of the message from the CDC data.
In January, Public Health Scotland released age-adjusted figures showing a Covid case rate of 11 per 1000 in the unvaccinated, compared with 25 per 1000 in the double-jabbed. The jabbed were also twice as likely to be hospitalized. (2)
In Israel we also have contradictory data from Jacob Giris, director of Ichilov Hospitalâs coronavirus ward who says:
âRight now, most of our severe cases are vaccinated,â Giris told Channel 13 News. âThey had at least three injections. Between seventy and eighty percent of the serious cases are vaccinated. So, the vaccine has no significance regarding severe illness, which is why just twenty to twenty-five percent of our patients are unvaccinated.â (3-4) emphasis mine
The Original Pfizer Controlled Trial Data
The original Pfizer clinical trial data shows 24% increased mortality in the vaccine group compared to the placebo group. The trial was originally planned to continue 2 years. It was halted after 6 months, so we don’t have long term data. This mortality finding is disturbing and a red flag warning the vaccine is harmful. The basic rule of new drug approval is this question: Do more people die in the drug group than the placebo group? If the answer is yes, why would anybody in their right mind take this drug?(5)
Next Leonhardt quotes an expert from Harvard:
“Vaccination is the most valuable intervention we can do,” William Hanage, an infectious-disease expert at Harvard, told me.
Yes, vaccination is valuable for the drug industry while they rake in billions, all the while enjoying full protection from any liability caused by their product. If you are injured or killed by the vaccine, you have no recourse, and no one to help you. You are on your own.
Vitamin D3 for Covid
There is no mention by Leonhardt of vitamin D3 to prevent mortality from COVID 19.  Recent Vitamin D studies shows NO Mortality from Covid in people with a vitamin D level above 50 ng/ml. A new study in Nutrients by Dr. Lorenz Borsche found that low vitamin D3 level correlates with increased mortality from Covid-19. The authorsâ data shows zero mortality when Vitamin D3 level is raised to 50 ng/ml. Although Vitamin D is available over the counter without a prescription, it is recommended that one works closely with a knowledgeable physician who can monitor vitamin D levels. (19) The authors state:
Regression suggested a theoretical point of zero mortality at approximately 50 ng/mL D3â¦.Despite ongoing vaccinations, we recommend raising serum 25(OH)D levels to above 50 ng/mL to prevent or mitigate new outbreaks due to escape mutations or decreasing antibody activity. (19)
In my opinion, Vitamin D3 is the most valuable intervention. Not vaccination. You haven’t heard about vitamin D because it is cheap, and widely available at the health food store.
Early Treatment for Covid with Repurposed Antiviral Drugs
A study of outcomes with Early Treatment by Brian Procter et al shows a 85-90 % reduction in hospitalization and mortality from COVID. (24) There is no mention of this in the NYT article. Early treatment modalities include zinc, quercetin, ivermectin, hydroxychloroquine, budesonide, thymoquinone, steroids, blood thinners, anti-inflammatories, fluvoxamine, etc. (16-17)
Natural Immunity to COVID
There is no mention of protection offered by Natural immunity. By now a majority of the unvaccinated have natural immunity which is more durable and robust than immunity provided by vaccination which is of limited durability. (8-14)Â Dennis G McGonagle dicusses natural immunity in Lancet February 07, 2022:
âFirst, it is well established that for single stranded RNA viruses such as influenza, natural immunity after recovery from infection provides better protection than vaccination, which needs to be undertaken annually because of waning vaccine immunity, …The same has been shown for SARS-CoV-2; in one study, individuals exposed to natural infection were ten-times less likely to be reinfected compared with vaccinated individuals without natural infection … Individuals exposed to natural infection were also less likely to be admitted to hospital with COVID-19.â (36) emphasis mine.
Unlike the unvaccinated people who are now immune, the vaccinated person must now undergo repeated booster shots every 6 months with possible suppression of the immune system, which will render the vaccine ineffective or even rendering “negative efficacy”. The WHO advises against repeated boosters because of possible harm to the immune system. (15)
ADE (antibody dependent enhancement)
Over the last twenty years, all previous corona virus vaccine attempts have failed, leaving dead or dying test animals. (28-39)
Two years of data on this new, incompletely tested, rushed mRNA vaccine roll out shows waning efficacy after 4-6 months, after which repeated boosters are advised with horrendous adverse side effects reported in VAERS.(18)
Long term, we have no idea what the adverse effects of repeated boosters will do on the immune system, on cancer risk, on fertility impairment, on auto immune system, on neurological disease, on vascular disease, etc.  This is one giant highly risky experiment on the human population.
Previous RNA Vaccine Rollouts Did Not Fare Well
Previous human vaccines against RSV and Dengue virus resulted in failed vaccine trials because of ADE, Antibody Dependent Enhancement. In the Philippines, failure of the Dengue vaccine program led to criminal charges for researchers. 830,000 children were given the âDengvaxiaâ, Dengue virus vaccine, before the program was suspended in 2017. (11-13) Dr Wen Shi Lee writes in Nature Microbiology (2020):
Previous respiratory syncytial virus and dengue virus vaccine studies revealed human clinical safety risks related to ADE, resulting in failed vaccine trials. (6-7) Endquote Dr. Lee
The new mRNA COVID vaccines were not studied sufficiently to exclude ADE upon re-exposure to the virus in the vaccinated population. Could negative efficacy in some studies be explained by ADE?
Repeated Boosters Ad Infinitum?
Once one starts on vaccination, when does it end? Many Public Health Officials have stated that repeated boosters every 6 months will be the norm. Israel is on its fourth shot (i.e. second booster) and case rate and deaths are the highest ever with omicron variant.
Adverse Effects
There is no mention of adverse side effects from the vaccine. The VAERS reporting system reports 20,000 deaths after vaccination . The under-reporting factor could be as high as 100, which translates to 2 million deaths after the vaccine in the US. This would make the COVID vaccine the most dangerous medical product ever rolled out for mass distribution. So far, this has been ignored by the media and health agencies in the US.
Life Insurance executives are reporting 40% increased death payouts in the working ages US, not due to Covid virus. Could this be due to the vaccine?
Athletes are collapsing on the field in front of national television. Many are dying with heart attacks. Could this be due to the vaccine?
Vaccine adverse side effects from the Department of Defense Database are listed in Senator Ron Johnsonâs letter to the Secretary of Defense 2/1/22. Here is a link to the letter which contained this quote:
Based on data from the Defense Medical Epidemiology Database (DMED), Renz
reported that these whistleblowers found a significant increase in registered diagnoses on DMED for miscarriages, cancer, and many other medical conditions in 2021 compared to a five-year average from 2016-2020.2 For example, at the roundtable Renz stated that registered diagnoses for neurological issues increased 10 times from a five-year average of 82,000 to 863,000 in 2021. There were also increases in registered diagnoses in 2021 for the following medical conditions:
Hypertension â 2,181% increase
Diseases of the nervous system â 1,048% increase
Malignant neoplasms of esophagus â 894% increase
Multiple sclerosis â 680% increase
Malignant neoplasms of digestive organs â 624% increase
Guillain-Barre syndrome â 551% increase
Breast cancer â 487% increase
Demyelinating Diseaseâ 487% increase
Malignant neoplasms of thyroid and other endocrine glands â 474% increase
Female infertility â 472% increase
Pulmonary embolism â 468% increase
Migraines â 452% increase
Ovarian dysfunction â 437% increase
Testicular cancer â 369% increase
end quote Sen Ron Johnson
Spike Protein is Pathogenic, Engineered with Gain of Function
What is the mechanism of harm of the spike protein? It is now obvious the genetic sequence of the original Wuhan strain virus was genetically manipulated in a lab to produce Gain of Function, make the virus more virulent by modifying the spike protein to attach to the ACE receptor. The vaccine uses a new and dangerous mRNA technology to “program” the cells of our bodies to make the pathogenic spike protein, the same genetic sequence published from the original Wuhan virus strain.
The adverse effects of the vaccine are due to the spike protein. Uncontrolled production of spike protein causes myocarditis, pericarditis, blood clotting, heart attacks, strokes, vascular disease, autoimmune destruction of platelets with uncontrolled bleeding, neurological injury. Longer term adverse effects are unknown.
If the original Wuhan strain spike protein is a bio-engineered gain of function bio-weapon, then what would you call the mRNA vaccine which uses the same genetic sequence for the spike protein? I would call it a perfect copy of the original bio-weapon.
High Quality Masks.
All the research looking at masks for prevention of influenza prior to to COVID pandemic shows masks are ineffective for prevention of viral transmission. Viruses travel as an aerosol which can not be stopped by a cloth mask. Try this experiment: Have a friend light a cigarette, put on a mask and blow the smoke out. Where does it go? The smoke is easily visible escaping as plumes from the sides of the mask. This is the virus aerosol spreading throughout the air in the room. Studies by Dr Jung from Korea show that fully masked health care workers transmit the virus easily from one another with only a few minutes of short conversation, both wearing masks .(26)
Masks are dangerous because they give a false sense of security. Cloth Masks used by the general public are frequently dirty and contaminated with bacteria and fungus causing infections on the face and eyes of the mask wearer. Masks obscure facial expressions and muffle speech. School Children forced to wear masks show developmental delays in speech and cognition.
Repurposed Drugs for Prevention and Treatment
We have repurposed antiviral drugs which are highly effective, safer and less expensive than the new patented drugs. These old drugs such as Ivermectin and Hydroxychloroquine have been used safely for years. Yet, the media and the government agencies have vilified, and suppressed the use of these drugs for early treatment, causing untold suffering in the population as discussed by Rep. Louie Gohmert in an Op Ed in the Washington Times. Rep. Gohmert advises Pres. Biden to embrace cheap repurposed drugs for Early Treatment of Covid 19. (25)
Rapid Tests
Home tests can be useful. However, we don’t need a test to know we are symptomatic with an upper respiratory virus with fever, cough , sore throat congestion etc. Best advice is to stay home if one has symptoms, just like we all did pre-Covid.
Bottom Line:
This NYT piece is nothing more than drug marketing propaganda, painting the Covid vaccines as “safe and effective” when they are neither. Rather than submit the healthy elderly to the merry-go-round of unending dangerous and ineffective vaccines every 6 months, a far better plan would be to optimize vitamin D3, and use Ivermectin, zinc and Quercetin for prevention. If symptomatic, use Early Treatment with Ivermectin, Hydroxychloroquine, Thymoquinone, blood thinners, etc. Early treatment protocols are published in the medical literature. Here is another one: Covid Patient Home Treatment Guide AAPS Why would anyone in their right mind submit to a poorly tested experimental treatment using a new mRNA technology which programs our cells to uncontrollably manufacture the spike protein having the exact same genetic sequence as the original Gain of Function Wuhan strain virus ?
Do not forget, the vaccine makers have no product liability, and no incentive to make a safe product. And, the drug industry has paid out 35 billion dollars in civil and criminal penalties, and has only one loyalty, to make profits for its shareholders. Why would anyone trust the drug industry or their media mouthpieces to tell the truth about anything ?
Articles with Related Interest:
Failed Pandemic Public Health Policy Who is to Blame ?
Top Experts Join Senator Ron Johnson in Panel Discussion
March for Medical Freedom in Washington DC
Omicron Has Mutated Into a Milder Disease
Is This The End of Medicine in America ?
Dr Peter McCullough Interview with Joe Rogan
C0\/lD \/accine Failure and l\/ermectin Success Story
Peter McCullough on Early Treatment vs Vaccination
Inventing the Covid Virus and Vaccine
Trick or Treat from the Demon Doctor ?
Pharmacies and TeleMed Services Providing Ivermectin
Robert Malone on the Covid War Games
Covid Conversation RoundTable San Juan Global summit
More Cov-idiocy from the Clown Department
Israel Should Stop Pfizer and Start Ivermectin Distribution
Causalties of the C0\/lD War, When Wlll this End ?
Rochelle Wolensky Warns of ADE Antibody Dependent Enhancement
Covid Vaccines Are Safe and Effective ?
Are Covid Vaccines the Next Vioxx ?
Ivermectin and the Failure of American Medicine
Ivermectin Antiparasitic Anticancer Miracle Drug
Vaccinoffee, a Vaccine with Every Coffee
Useful Resources:
Covid Patient Home Treatment Guide AAPS
Telemedicine Services to Obtain Ivermectin
Unity Project Online: Working together to STOP COVID-19 Vaccine Mandates for Healthy Children K-12
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
www.drdach.com
Heart Book by Jeffrey Dach
Links and References
1) The Morning: Protecting the vulnerable Feb 14, 2022 NYTÂ By David Leonhardt
“Good morning. We offer a guide to protecting vulnerable people â the elderly, immunocompromised and unvaccinated â from Covid.
3) 80% of serious COVID cases are fully vaccinated’ says Ichilov hospital director
Vaccine has “no significance regarding severe illness,” says Prof. Jacob Giris.
Israel National News 03.02.22 15:12
Prof. Jacob Giris, director of Ichilov Hospitalâs coronavirus ward, said in a TV interview that many of the severe cases are vaccinated.
âRight now, most of our severe cases are vaccinated,â Giris told Channel 13 News. âThey had at least three injections. Between seventy and eighty percent of the serious cases are vaccinated. So, the vaccine has no significance regarding severe illness, which is why just twenty to twenty-five percent of our patients are unvaccinated.â
Giris also spoke at the cabinet meeting on Sunday and told ministers, âDefining a serious patient is problematic. For example, a patient with a chronic lung disease always had a low level of oxygen, but now he has a positive coronavirus test result which technically makes him a âserious coronavirus patient,â but thatâs not accurate. The patient is only in a difficult condition because he has a serious underlying illness.â
4) Israel’s Most Prestigious Hospital: ‘70% to 80% of Serious Covid Cases are Fully Vaccinated’ (Video) Amy Mek February 9, 2022
Despite Israel being one of the most âvaccinatedâ and âboostedâ countries in the world, the number of Covid deaths continues to break record after record.
————————– ———————————
5) 24% Increased Mortality in Vaccinated Compared to Placebo Israel National News David rosenberg 11/176/21
In addition, the original Pfizer COVID vaccine clinical trial shows 24 percent increased mortality in the vaccine group compared to placebo. FDA report finds all-cause mortality higher among vaccinated FDA report shows Pfizerâs clinical trials found 24% higher all-cause mortality rate among the vaccinated compared to placebo group. David Rosenberg
The FDA report, however, revealed a larger number of deaths by all causes in both groups, with 17 deaths among the control group and 21 in the vaccinated cohort.
6) Risk of COVIDâ19 vaccines worsening clinical disease
1.âTHE RISK OF ADE IN COVIDâ19 VACCINES IS NONâTHEORETICAL AND COMPELLING
Vaccinees at higher risk for more severe COVIDâ19 disease when they encounter circulating viruses.
7)Â Lee, Wen Shi, et al. âAntibody-dependent enhancement and SARS-CoV-2 vaccines and therapies.â Nature microbiology 5.10 (2020): 1185-1191.
Antibody-based drugs and vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are being expedited through preclinical and clinical development. Data from the study of SARS-CoV and other respiratory viruses suggest that anti-SARS-CoV-2 antibodies could exacerbate COVID-19 through antibody-dependent enhancement (ADE). Previous respiratory syncytial virus and dengue virus vaccine studies revealed human clinical safety risks related to ADE, resulting in failed vaccine trials. Here, we describe key ADE mechanisms and discuss mitigation strategies for SARS-CoV-2 vaccines and therapies in development. We also outline recently published data to evaluate the risks and opportunities for antibody-based protection against SARS-CoV-2.
8) (Cleveland Clnic Study)
Shrestha NK. 2021. Necessity of COVID-19 Vaccination in Previously Infected Individuals: A Retrospective Cohort Study. medRxiv.
study only looked at individuals over a five-month period
The study concludes, âindividuals who have laboratory-confirmed symptomatic SARS-CoV-2 infection are unlikely to benefit from COVID-19 vaccination, and vaccines can be safely prioritized to those who have not been infected before.â
Importantly, not a single incidence of SARS-CoV-2 infection was observed in previously infected participants with or without vaccination.
(LA)
9) Kojima, Noah, et al. âIncidence of Severe Acute Respiratory Syndrome Coronavirus-2 infection among previously infected or vaccinated employees.â medRxiv (2021).
Previous SARS-CoV-2 infection and vaccination for SARS-CoV-2 were
associated with decreased risk for infection or re-infection with SARS-CoV-2 in a routinely screened workforce. The was no difference in the infection incidence between vaccinated individuals and individuals with previous infection.
(Israel)
10) Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections by Sivan Gazit, MD MA1,2*; Roei Shlezinger, BA1; Galit Perez, MN MA2; Roni Lotan, PhD2; Asaf Peretz, MD1,3; Amir Ben-Tov, MD1,4; Dani Cohen, PhD4; Khitam Muhsen, PhD4; Gabriel Chodick, PhD MHA2,4; Tal Patalon, MD1,
This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. end quote
11) O Murchu, Eamon, et al. âQuantifying the risk of SARSâCoVâ2 reinfection over time.â Reviews in medical virology (2021): e2260.
Only one study estimated the populationâlevel risk of reinfection based on whole genome sequencing in a subset of patients; the estimated risk was low (0.1% [95% CI: 0.08â0.11%]) with no evidence of waning immunity for up to 7 months following primary infection. These data suggest that naturally acquired SARSâCoVâ2 immunity does not wane for at least 10 months postâinfection.
12) Goldberg, Yair, et al. âProtection of previous SARS-CoV-2 infection is similar to that of BNT162b2 vaccine protection: A three-month nationwide experience from Israel.â medRxiv (2021).
Vaccination was highly effective with overall estimated efficacy for documented infection of 92·8% (CI:[92·6, 93·0]); hospitalization 94·2% (CI:[93·6, 94·7]); severe illness 94·4% (CI:[93·6, 95·0]); and death 93·7% (CI:[92·5, 94·7]). Similarly, the overall estimated level of protection from prior SARS-CoV-2 infection for documented infection is 94·8% (CI:[94·4, 95·1]); hospitalization 94·1% (CI:[91·9, 95·7]); and severe illness 96·4% (CI:[92·5, 98·3]). Our results question the need to vaccinate previously-infected individuals.
13) Pilz, Stefan, et al. âSARSâCoVâ2 reâinfection risk in Austria.â European Journal of Clinical Investigation 51.4 (2021): e13520.
We observed a relatively low re- infection rate of SARS- CoV- 2 in Austria. Protection against SARS- CoV- 2 after natural infection is comparable with the highest available estimates on vaccine efficacies.
14) Sheehan, Megan M., Anita J. Reddy, and Michael B. Rothberg. âReinfection rates among patients who previously tested positive for COVID-19: a retrospective cohort study.â medRxiv (2021).
Conclusions Prior infection in patients with COVID-19 was highly protective against reinfection and symptomatic disease. Protective effectiveness increased over time, suggesting that viral shedding or ongoing immune response may persist beyond 90 days and may not represent true reinfection. As vaccine supply is a limited resource around the world, patients with known history of COVID-19 could delay early vaccination to allow for the most vulnerable to access the vaccine and slow transmission.
15) Frequent Boosters Spur Warning on Immune Response
By Irina Anghel January 11, 2022, Bloomberg News
European Union regulators warned that frequent Covid-19 booster shots could adversely affect the immune response and may not be feasible.
16) McCullough, Peter A., et al. âMultifaceted-highly-targeted-sequential-multidrug-treatment-of-early-ambulatory-high-risk-SARS-CoV-2-Infection (COVID-19).â Reviews in cardiovascular medicine 21.4 (2020): 517.
17) McCullough, Peter A., et al. âPathophysiological basis and rationale for early outpatient treatment of SARS-CoV-2 (COVID-19) infection.â The American journal of medicine 134.1 (2021): 16-22.
Waning Vaccine Efficacy
18) Cohn, Barbara A., et al. âBreakthrough SARS-CoV-2 infections in 620,000 US Veterans, February 1, 2021 to August 13, 2021.â medRxiv (2021). Cohn Barbara Breakthrough SARS CoV2 Veterans, Feb 2021 to Aug 2021 medRxiv..full
19) Borsche, Lorenz, Bernd Glauner, and Julian von Mendel. âCOVID-19 mortality risk correlates inversely with vitamin D3 status, and a mortality rate close to zero could theoretically be achieved at 50 ng/ml 25 (OH) D3: Results of a systematic review and meta-analysis.â Nutrients 13.10 (2021): 3596.
Regression suggested a theoretical point of zero mortality at approximately 50 ng/mL D3â¦.Despite ongoing vaccinations, we recommend raising serum 25(OH)D levels to above 50 ng/mL to prevent or mitigate new outbreaks due to escape mutations or decreasing antibody activity.
20)Â 34) Gundry, Steven R. âMrna COVID Vaccines Dramatically Increase Endothelial Inflammatory Markers and ACS Risk as Measured by the PULS Cardiac Test: a Warning.â Circulation 144.Suppl_1 (2021): A10712-A10712.
21)Â 35) Ivermectin reduces the risk of death from COVID-19 -a rapid review and meta-analysis in support of the recommendation of the Front Line COVID-19 Critical Care Alliance. (Latest version v1.2 â 6 Jan 2021) January 2021 Project: Ivermectin to prevent and treat COVID-19 Authors: Theresa A Lawrie
22) 36) Dixit, Alok, Ramakant Yadav, and Amit Vikram Singh. âIvermectin: potential role as repurposed drug for COVID-19.â The Malaysian journal of medical sciences: MJMS 27.4 (2020): 154.
23) 37) Chamie-Quintero, Juan, Jennifer A. Hibberd, and David Scheim. âIvermectin for COVID-19 in Peru: 14-fold reduction in nationwide excess deaths, p=. 002 for effect by state, then 13-fold increase after ivermectin use restricted.â (2021).
24) Procter, Brian, and McCullough âEarly Ambulatory Multidrug Therapy Reduces Hospitalization and Death in High-Risk Patients with SARS-CoV-2 (COVID-19).â Int J of Innovative Res in Med Sci (IJIRMS) 6.03 (2021).Procter_Early_ambulatory_multidrug_therapy_reduces_hospitalization_and_death_in_high-risk_patients_with_sars-cov-2__covid-19__ijirms_2021
25) Biden should embrace every weapon against COVID-19 By Rep. Louie Gohmert – – Sunday, February 13, 2022 . Cheap, safe, generic medicines can help people recover.
26) Jung, Jiwon, et al. “Frequent Occurrence of SARS-CoV-2 Transmission among Non-close Contacts Exposed to COVID-19 Patients.” Journal of Korean medical science 36.33 (2021).
27) How the CDC Abandoned Science. Mass youth hospitalizations, COVID-induced diabetes, and other myths from the brave new world of science as political propaganda
by Vinay Prasad February 14, 2022 Tablet Magazine
So why does the supposedly impartial CDC push weak or flawed studies to support the administrationâs pandemic policy goals? The cynical answer is that the agency is not in fact impartial (and thus not sufficiently scientific), but captured by the countryâs national political system. That answer has become harder to avoid. This is a precarious situation, as it undermines trust in federal agencies and naturally leads to a trust vacuum, in which Americans feel forced to cast about in a confused search for alternative sources of information. Once that trust is broken, itâs not easily regained.
28) Schindewolf, Craig, and Vineet D. Menachery. âMiddle East respiratory syndrome vaccine candidates: cautious optimism.â Viruses 11.1 (2019): 74.
Vaccine candidates against SARS-CoV were initially developed based on the full-length S protein. However, these vaccines were later demonstrated to induce non-neutralizing antibodies which did not prevent MERS-CoV infection, and the immunized animals were not protected from the viral challenge instead they experienced adverse effects like enhanced hepatitis, increased morbidity, and stronger inflammatory responses (Weingartl et al., 2004; Czub et al., 2005). Many potential vaccines against MERS-CoV were also mainly focused on the same full-length S protein, raising a safety concern on the practical application of these vaccines (Du et al., 2016b).
29) Takano, Tomomi, et al. âPathogenesis of oral type I feline infectious peritonitis virus (FIPV) infection: Antibody-dependent enhancement infection of cats with type I FIPV via the oral route.â Journal of Veterinary Medical Science (2019): 18-0702.
30) Takano, Tomomi, et al. âAntibody-dependent enhancement of serotype II feline enteric coronavirus infection in primary feline monocytes.â Archives of virology 162.11 (2017): 3339-3345.
31) Iwasaki, Akiko, and Yexin Yang. âThe potential danger of suboptimal antibody responses in COVID-19.â Nature Reviews Immunology 20.6 (2020): 339-341.
32) Tseng, Chien-Te, et al. âImmunization with SARS coronavirus vaccines leads to pulmonary immunopathology on challenge with the SARS virus.â PloS one 7.4 (2012): e35421.
33) Bolles, Meagan, et al. âA double-inactivated severe acute respiratory syndrome coronavirus vaccine provides incomplete protection in mice and induces increased eosinophilic proinflammatory pulmonary response upon challenge.â Journal of virology 85.23 (2011): 12201-12215.
34) Agrawal, Anurodh Shankar, et al. âImmunization with inactivated Middle East Respiratory Syndrome coronavirus vaccine leads to lung immunopathology on challenge with live virus.â Human vaccines & immunotherapeutics 12.9 (2016): 2351-2356.
35) Yasui, Fumihiko, et al. âPrior immunization with severe acute respiratory syndrome (SARS)-associated coronavirus (SARS-CoV) nucleocapsid protein causes severe pneumonia in mice infected with SARS-CoV.â The Journal of Immunology 181.9 (2008): 6337-6348.
36)Â Health-care workers recovered from natural SARS-CoV-2 infection should be exempt from mandatory vaccination edicts Dennis G McGonagle Lancet February 07, 2022
âFirst, it is well established that for single stranded RNA viruses such as influenza, natural immunity after recovery from infection provides better protection than vaccination, which needs to be undertaken annually because of waning vaccine immunity,â…. âThe same has been shown for SARS-CoV-2; in one study, individuals exposed to natural infection were ten-times less likely to be reinfected compared with vaccinated individuals without natural infection (adjusted hazard ratio 0·02, 95% CI 0·01â0·04 for previous infection vs 0·26, 0·24â0·28 for vaccination). Individuals exposed to natural infection were also less likely to be admitted to hospital with COVID-19.â
Published on February 15th, 2022 by Jeffrey Dach MD
The post More Deceptive Drug Marketing from the New York Times appeared first on Jeffrey Dach MD.
February 4, 2022
Failed Pandemic Public Health Policy Who is to Blame ?
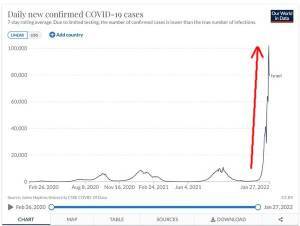 Failed Pandemic Public Health Policy Who is to Blame ?
Failed Pandemic Public Health Policy Who is to Blame ?
by Jeffrey Dach MD
Robert Malone MD feels that the hospitals and the government are to blame. The government is happy to go along with the hospital system “bilking billions of dollars” from government COVID incentives “by claiming excess disease and deaths” . This involves “playing with the numbers” What are real rates of disease and death in the USA. Nobody knows. We have to get the true numbers from other countries that actually keep real records. Here is a quote from Dr Robert Malone:
Our Hospital systems are failing in the US. THEY ARE FAILING. Our physicians are threatened and persecuted if they use life saving treatments. Hospitalists are determined to continue to push and insist on treatments that have been proven to not be safe or effective in our hospitals. Hospitals in the USA are fraudulently bilking the US Government for literally billions of dollars, by claiming excess disease and death. So much so, that it has become impossible to figure out the true rates of disease and death of Covid-19 and for all causes in the USA. It is shocking.
To actually cite reasons why this may be happening, such as the vaccines aren’t working, physicians right to treat and try has been removed, hospitals are literally killing people with their rigid and failed policies and treatments is death of one’s career. It you speak of the fraud happening at the very hospital you may be working at, it is grounds for dismissal.
And the US government not only doesn’t care, it supports the actions of such hospitalists. endquote emphasis mine . (1)
Blame Game: Authors of the Great Barrington Declaration Write in Newsweek
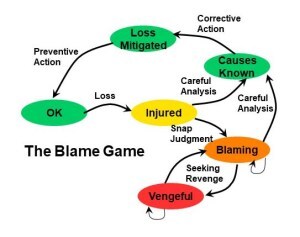 Martin Kulldorff and Jay Bhattacharya, two of the three authors of the Great Barrington Declaration, just published an Opinion piece in Newsweek entitled: Dr. Fauci and the Coronavirus Policy Blame Game. One might cite this appearance in NewsWeek, about as mainstream as you can get, by two “medical heretics” as proof the Covid narrative is shifting. The two eminent doctors should have been hailed as heros, but a sinister campaign disclosed in emails between Fauci and Collins derailed their careers. The two place the blame for failed public health policies firmly on Anthony Fauci, head of the NIAID a branch of the NIH. Here is their quote:
Martin Kulldorff and Jay Bhattacharya, two of the three authors of the Great Barrington Declaration, just published an Opinion piece in Newsweek entitled: Dr. Fauci and the Coronavirus Policy Blame Game. One might cite this appearance in NewsWeek, about as mainstream as you can get, by two “medical heretics” as proof the Covid narrative is shifting. The two eminent doctors should have been hailed as heros, but a sinister campaign disclosed in emails between Fauci and Collins derailed their careers. The two place the blame for failed public health policies firmly on Anthony Fauci, head of the NIAID a branch of the NIH. Here is their quote:
most people now realize that Washington’s pandemic policies failed. Lockdowns just postponed the inevitable while causing enormous collateral damage on cancer, cardiovascular disease, diabetes, tuberculosis, mental health, education and much else…So, the blame game is in full swing. At a recent Senate hearing, Dr. Anthony Fauci did not even attempt to defend his policies. endquote (2)
What were these failed policies which Anthony Fauci did not bother to defend?
1) Lock Down the Country to “Flatten the Curve” (5-7)
2) Blocked use of Early Treatment: Hydroxychloroquine and Ivermectin and other drugs.(11-12)
2) Denied Natural Immunity after recovery from infection.
3) Funded Gain of Function Research in Wuhan lab.
4) Pushed high vaccine efficacy rates to the public when in fact the vaccines do not stop infection or spread of disease. (13-15)
You can read my satire pieces on Anthony Fauci at these links:
More C0\/-Idiocy from the Clown Department
Trick or Treat from the Demon Doctor ?
Johns Hopkins on Failure of Lockdowns
A Literature Review and Meta-Analysis of the Effects of Lockdowns on COVID-19 Mortality by Jonas Herby, Lars Jonung, and Steve H. Hanke of Johns Hopkins Medical School reviews 24 studies on lockdowns. The authors concluded lockdowns have little or no public health effects, are ill-founded and should be rejected as a policy instrument:
While this meta-analysis concludes that lockdowns have had little to no public health effects, they have imposed enormous economic and social costs where they have been adopted. In consequence, lockdown policies are ill-founded and should be rejected as a pandemic policy instrument. (5-7)
Kerry Wakefield Australia
An excellent play by play chronology of the failure of western public health policies comes from Kerry Wakefield in Australia, pointing out a number of inconvenient truths, namely, the vaccinated are catching Omicron variant at a higher rate than the unvaccinated. This is called “negative efficacy” of the vaccines. I would venture to guess this could be explained two ways: 1) the existence of “natural immunity” after recovery from infection in the unvaccinated which reduces severity of symptoms when exposed a second time. 2) immuno-suppressive effect or ADE (Antibody dependent enhancement) effect of the vaccines which increases severity of symptoms when exposed to a viral load.(13-15)
(3) Here is his quote:
The West’s Covid-19 strategy of lockdowns, mass vaccinations and extreme curbs is losing credibility by the moment…Despite vaccination levels running at 70 per cent and above in many Western nations, Covid cases are at record levels across the UK, Europe, Australia, the US, Israel…The variants are outrunning the scientists’ vaccines, vaccine efficacy is waning, and multiple health authorities such as the WHO and the European Medicines Agency (EMA) have come out warning against repeated boosters, not only because they were designed for previous variants, but because they may have adverse health effects…
Former UK vaccine agency boss Dr Clive Dix says vaccinations have now become a ‘waste of time’… For most in the West, the pandemic seems clearly over…the global mass vaccination strategy is looking more like a foreseeable error; vaccines inevitably trail viral variants and as with the flu vaccine, being protected against last year’s variant may not be much help against this year’s strain…
New reports show the jabbed seem more likely to catch Covid than the unjabbed, possibly due to an immune-suppression effect of the vaccines.
In January, Public Health Scotland released age-adjusted figures showing a Covid case rate of 11 per 1000 in the unvaccinated, compared with 25 per 1000 in the double-jabbed. The jabbed were also twice as likely to be hospitalized. ( 3)
Dr Harvey Risch Brownstone Institute
Epidemiologist from Yale, Dr Harvey Risch has always been a voice of reason standing high above the mediocrity of seemingly brain dead public health officials pronouncements. He should have been consulted by government for his opinion. Shockingly, he was ignored. Dr Risch concludes it is time to “terminate the pandemic state of emergency”. Here is the quote:
The time has come to terminate the pandemic state of emergency. It is time to end the controls, the closures, the restrictions, the plexiglass, the stickers, the exhortations, the panic-mongering, the distancing announcements, the ubiquitous commercials, the forced masking, the vaccine mandates…
Measures like mandatory masking and distancing have had negligible or at most small effects on transmission. Large-scale population quarantines only delay the inevitable. Vaccination and boosters have not halted omicron disease spread; heavily vaccinated nations like Israel and Australia have more daily cases per capita than any place on earth at the moment. This wave will run its course despite all of the emergency measures.
Until omicron, recovery from Covid provided substantial protection against subsequent infection. While the omicron variant can reinfect patients recovered from infection by previous strains, such reinfection tends to produce mild disease. Future variants, whether evolved from omicron or not, are unlikely to evade the immunity provided by omicron infection for a long while.
Given that omicron, with its mild infection, is running its course to the end, there is no justification for maintaining emergency status. The lockdowns, personnel firings and shortages and school disruptions have done at least as much damage to the population’s health and welfare as the virus.
Americans have sacrificed enough of their human rights and of their livelihoods for two years in the service of protecting the general public health. Omicron is circulating but it is not an emergency. The emergency is over. The current emergency declaration must be canceled. It is time. emphasis mine (4)
Twelve European Countries Lift Covid Restrictions
Perhaps a number of European countries have harkened to Dr Harvey Risches words ? Or perhaps they have similar epidemiologist advisors who share the same views. 12 countries in Europe have declared the end of COVID restrictions. Israel has declared they will scrap the “Green Pass” Vaccine Passport to enter restaurants, hotels, gyms, and theaters in Israel.(8-10)
Sweden and Switzerland joined Denmark, Norway, Finland, Ireland, The Netherlands, Italy, Lithuania, France and the UK in announcing they will lift COVID restrictions and open up their countries. ending all Covid restrictions.(8)
Iowa Governor Announces Opening Up Iowa
Iowa Governor Kim Reynolds joined the approx. 25 other states who have announced the end of Covid as a Public Health Emergency. In her state, she will suspend the state of Emergency. Here is her statement:
Today I’m announcing the end of the Public Health Disaster Proc, effective 11:59 p.m., Feb. 15. …We cannot continue to suspend duly enacted laws and treat COVID-19 as a public health emergency indefinitely. After two years, it’s no longer feasible or necessary. The flu and other infectious illnesses are part of our everyday lives, and coronavirus can be managed similarly…Nearly half of U.S. states have already discontinued their public health proclamations, and several more are set to expire in February if they aren’t renewed. end quote Reference Dennis Michael Lynch.
Covid Vaccines Fail to Stop Spread of COVID
These two chart of daily cases and hospitalizations in heavily vaccinated Israel (Pfizer) shows vaccine failure to stop spread of COVID. Cases and hospitalizations exceed all previous waves. See Red Arrows. (courtesy of Worldometer):


Vaccine Adverse Effects – Life Insurance Payouts
I first brought attention to the alarming increase in adverse events reported for the COVID vaccines back in May and August of 2021 in these two newsletters:
Could the Covid Vaccine Be the Next Vioxx ? 5/25/21
The Covid Vaccine is Safe and Effective? 8/1/21
More recently, we have revelations from the Life Insurance Industry of increased 40% death payouts in working age group, age 18-64. Most of the life insurance death claims are not labeled as due to COVID. (16-17) As you might recall, the vast majority of mortality from Covid has been in the elderly, above the age of 65, and those with with underlying preconditions, so overall mortality from COVID can not explain a 40% increase in life insurance death pay outs in the 18-64 age group.
Here is the quote from Indiana Life Insurance Company One America from Mr Davison:
We are seeing, right now, the highest death rates we have seen in the history of this business. Most of the claims for deaths being filed are not classified as COVID-19 deaths, Davison said the company is seeing an “uptick” in disability claims, saying at first it was short-term disability claims, and now the increase is in long-term disability claims. (16)
What is causing this massive wave of suddenly increased mortality in this age group that is not elderly nor at the end of their life span? Many of these deaths are related to cardiovascular disease, heart attacks and strokes, as one might expect from the pathogenic spike protein which attacks the vascular system. This is the same spike protein the mRNA “vaccine” instructs our cells to manufacture in uncontrolled amounts.
I would take a wild guess and raise this question: “What mass medical intervention has taken place during this same time period?” Connect the dots, and the inescapable question is: “could it be the vaccines”? After all, our VAERS system is showing a “safety signal” of massively increased injury and death. (Note: VAERS= vaccine adverse event reporting system). In the mainstream media, this massive increase in mortality is being attributed to the virus itself, rather than the vaccine.
24% Increased Mortality in Vaccinated Compared to Placebo
In addition, the original Pfizer COVID vaccine clinical trial shows 24 percent increased mortality in the vaccine group compared to placebo. (18)
Unfortunately there is no official or formal clinical follow up in the vaccinated population, which is an experimental vaccine with EUA (emergency use authorization). The word is that vaccine adverse events and deaths are ignored or suppressed by the medical system. So, there is no way to answer this question with hard data. There has been no clinical follow up of the vaccinated population !
Correction: The FDA last week just gave full approval for the Moderna vaccine SpikeVAX and as we all know, previously gave full approval to Pfizer Cominarty vaccine. Will Spikevax be unavailable in the US, similar to the shell game with Cominarty? We will have to wait and see.
There are a few exceptions. The Department of Defense (DOD) has hard data on the military and this data is about to be explosively revealed showing the numbers and severity of various vaccine adverse events. Some of this data was revealed by Attorney Tom Renz at Senator Johnson’s “Second Opinion” Senate Hearing . You can view the entire 5 hour round table discussion in the Senate hearing room at this link: Top Experts Join Senator Ron Johnson in Panel Discussion
We await the release of this DOD information on Vaccine adverse effects in the military, and hope that it is not suppressed or censored as has been the usual case.
Increased Mortality in Countries with High Vaccination Rates
Mike Whitney at the Expose has compiled the data from a number of highly vaccinated countries showing increased mortality. His analysis is compelling and disturbing. (19)
Also from the Expose in the UK, here is data in (below chart) from the UK showing increased mortality rate per 100,000 person years in the younger age group (age 10-14) after two dose vaccination compared to the unvaccinated. See tall Red Column on left.

UK Data (See Above Chart , highest red bar at left showing increased mortality after 2 dose vaccination x 52 times for age 10-14)
Official Data shows Children are up to 52 times more likely to die following Covid-19 Vaccination than Unvaccinated Children & the ONS is trying to hide it By The Exposé on January 29, 2022
What is Happening with the Truckers in Canada ?
Leave it to CJ Hopkins to give us his insight on what is happening with the Truckers in Ottawa in his Feb 4 substack entry entitled: Attack of the Transphobic Putin-Nazi Truckers! CJ Hopkins has been following the political side of the Covid pandemic and claims: “This isn’t an abstract argument over ‘the science.’ It is a fight … a political, ideological fight. On one side is democracy, on the other is totalitarianism. Pick a side, and live with it.”
Mr. Hopkins sees the Canadian truckers as the “power of the people” to oppose the roll out of a totalitarian form of government. We should all be grateful to these truckers who are standing up for freedom, Canadian freedom and our freedom as well. Here is the quote from CJ Hopkins:
This is it. This is that fight. It is not a protest. It is a game of chicken. A high-stakes game of political chicken. In the end, politics comes down to power. The power to force your will on your adversary. GloboCap has been forcing the New Normal on people around the world for the past two years. What we are witnessing in Canada is the power of the people, the power the people have always had, and which we will always have, when we decide to use it … the power to shut down the whole GloboCap show, city after city if necessary. quoted from Attack of the Transphobic Putin-Nazi Truckers!
Here is an anonymous comment on facebook:
Eventually this protest will go down in history as a cornerstone of the freedom-movement. These people have upended their life to fight for us all. They are true modern heroes and someday society will remember and honor them as such….end quote … anonymous facebook user.
View videos of the Canadian Trucker Protest at this LINK
Conclusion: Who is to blame for the failure of public health policies? The entire medical system, our government, the pharmaceutical industry, in short, every one. When will the Covid Pandemic be over ? When you say it is over.
Articles with Related Interest:
Top Experts Join Senator Ron Johnson in Panel Discussion
March for Medical Freedom in Washington DC
Omicron Has Mutated Into a Milder Disease
Is This The End of Medicine in America ?
Dr Peter McCullough Interview with Joe Rogan
C0\/lD \/accine Failure and l\/ermectin Success Story
Peter McCullough on Early Treatment vs Vaccination
Inventing the Covid Virus and Vaccine
Trick or Treat from the Demon Doctor ?
Pharmacies and TeleMed Services Providing Ivermectin
Robert Malone on the Covid War Games
Covid Conversation RoundTable San Juan Global summit
More Cov-idiocy from the Clown Department
Israel Should Stop Pfizer and Start Ivermectin Distribution
Causalties of the C0\/lD War, When Wlll this End ?
Rochelle Wolensky Warns of ADE Antibody Dependent Enhancement
Covid Vaccines Are Safe and Effective ?
Are Covid Vaccines the Next Vioxx ?
Ivermectin and the Failure of American Medicine
Ivermectin Antiparasitic Anticancer Miracle Drug
Vaccinoffee, a Vaccine with Every Coffee
Useful Resources:
Covid Patient Home Treatment Guide AAPS
Telemedicine Services to Obtain Ivermectin
Unity Project Online: Working together to STOP COVID-19 Vaccine Mandates for Healthy Children K-12
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
www.drdach.com
Heart Book by Jeffrey Dach
Links and References
Blame Game image courtesy of wikimedia commons
Charts courtesy of Worldometer
Failure of Washington’s pandemic policies
1) The US Public Health Response has been a Colossal Failure
The US Deaths keep piling up…Robert W Malone MD, MS 2/3/22
2) Dr. Fauci and the Coronavirus Policy Blame Game Opinion Martin Kulldorff and Jay Bhattacharya On 1/31/22 Newsweek
With millions of Americans getting infected and over 800,000 reported COVID-19 deaths, most people now realize that Washington’s pandemic policies failed. Lockdowns just postponed the inevitable while causing enormous collateral damage on cancer, cardiovascular disease, diabetes, tuberculosis, mental health, education and much else.
So, the blame game is in full swing. At a recent Senate hearing, Dr. Anthony Fauci did not even attempt to defend his policies. Instead, he insisted that: “Everything that I have said has been in support of the CDC guidelines.”
3) The reckoning has begun The West’s Covid strategy is crumbling
Kerry Wakefield 22 January 2022 Spectator Australia
The West’s Covid-19 strategy of lockdowns, mass vaccinations and extreme curbs is losing credibility by the moment, even if various wannabe-despots are slow to realise it.
Despite vaccination levels running at 70 per cent and above in many Western nations, Covid cases are at record levels across the UK, Europe, Australia, the US, Israel and more, nearly two years after the virus first escaped China. The variants are outrunning the scientists’ vaccines, vaccine efficacy is waning, and multiple health authorities such as the WHO and the European Medicines Agency (EMA) have come out warning against repeated boosters, not only because they were designed for previous variants, but because they may have adverse health effects.
‘We should be careful in not overloading the immune system with repeated immunizations,’ warned Marco Cavaleri, the EMA head of vaccines strategy.
Former UK vaccine agency boss Dr Clive Dix says vaccinations have now become a ‘waste of time’. And finally, early treatments are in focus – new drugs, antivirals and more.
For most in the West, the pandemic seems clearly over, even if care must still be taken to protect the vulnerable and our hospital system. The best aspect of Australia’s response is that, geographically isolated, we kept the more dangerous original virus and variants at bay until milder Omicron arrived. No doubt this saved thousands of lives. But with the benefit of hindsight, the global mass vaccination strategy is looking more like a foreseeable error; vaccines inevitably trail viral variants and as with the flu vaccine, being protected against last year’s variant may not be much help against this year’s strain.
Australia, except for wayward sandgropers, has abandoned its policy of zero-Covid and is letting the dominant, milder Omicron variant run. The result is rocketing case numbers, pressure on hospital systems, and a two-note chant from our politicians of vax, vax, boost, vax, vax boost. Yet the ‘vaccines’ have not prevented infection or transmission among the jabbed, and are of little efficacy against Omicron, as even Pfizer boss Albert Bourla said recently. Yes, a third shot might provide a few more weeks of protection – until the next variant.
And how severe is Omicron? It poses a 91 per cent lower death threat than the Delta variant, said Centres for Disease Control (CDC) director Rochelle Walensky, citing a big new study showing only one death among 52,000 Omicron cases. Eminent Stanford epidemiologist John Ioannidis released a study recently of Covid infection fatality rates in the unvaccinated, which ranged from 0.0013 per cent in those aged 0-19 to 4.9 per cent in those aged over 70. The study concluded that fatality rates were lower than previously reported. Add in any vaccine efficacy in reducing the worst outcomes, and the real threat is even lower.
Here, Australian Bureau of Statistics figures up to October 2021 put the median age of Covid deaths at 83, (which is also our life expectancy), of whom 70 per cent had chronic pre-existing conditions, commonly heart disease. By mid-January, as cases and testing raged, Covid’s death tally had climbed to nearly 2,600 over nearly two years. In contrast, flu and pneumonia killed 4,124 Australians in 2019, around 11 people a day, and somehow, we didn’t panic, mask or lock down. Our Covid case fatality rate is one per cent, barely affecting those under 60 (0.1 per cent) but far deadlier for the elderly. Relatives who’ve had it recently say it’s just a bad cold. So, if you’re ill, old, or obese, take your shots, but normal life should return for everyone else.
This sounds remarkably like the strategy outlined in the Great Barrington Declaration (GBD), authored by eminent scientists from Oxford, Harvard, and Stanford, and signed by 60,000 physicians, which argued for focussed protection, herd immunity and early treatments – not mass vaccination, lockdowns and masking.
The US health establishment colluded to bury this push, an email recently emerging in which the National Institutes of Health boss, Francis Collins, asked National Institutes of Allergy and Infectious Diseases head honcho Anthony Fauci for ‘a quick and devastating take down’ of these ‘fringe epidemiologists’.
Early treatment options that emerged got similarly ‘cancelled’. A recent leaked report from the ne plus ultra of US top secret squirrel agencies, the Defence Advanced Research Projects Agency criticises in passing the suppression of potential curatives. Author Major Joseph Murphy said both ivermectin and hydroxychloroquine were identified as Covid curatives in April 2020 but noted that the files containing this information were unmarked and thus effectively hidden.
Moreover, the bills for this Fauci-driven strategy, especially the rushed and experimental ‘vaccines’, are coming due. New reports show the jabbed seem more likely to catch Covid than the unjabbed, possibly due to an immune-suppression effect of the vaccines.
In January, Public Health Scotland released age-adjusted figures showing a Covid case rate of 11 per 1000 in the unvaccinated, compared with 25 per 1000 in the double-jabbed. The jabbed were also twice as likely to be hospitalised.
4) The Emergency Must Be Ended, Now By Harvey Risch, Jayanta Bhattacharya, Paul Elias Alexander January 23, 2022
he time has come to terminate the pandemic state of emergency. It is time to end the controls, the closures, the restrictions, the plexiglass, the stickers, the exhortations, the panic-mongering, the distancing announcements, the ubiquitous commercials, the forced masking, the vaccine mandates.
We don’t mean that the virus is gone – omicron is still spreading wildly, and the virus may circulate forever. But with a normal focus on protecting the vulnerable, we can treat the virus as a medical rather than a social matter and manage it in ordinary ways. A declared emergency needs continuous justification, and that is now lacking.
=======================================================
5) Covid lockdown ‘prevented only 0.2pc of deaths in first wave’
Researchers say the costs of lockdowns to society far outweighed the benefits and argue that they should be ‘rejected out of hand’
6) FOX 5 DC Johns Hopkins study shows lockdowns only reduced COVID-19 death rate by .2%
Lockdowns during the first COVID-19 wave in the spring of 2020 only reduced COVID-19 mortality by .2% in the U.S. and Europe
Abstract: This systematic review and meta-analysis are designed to determine whether there is empirical evidence to support the belief that “lockdowns” reduce COVID-19 mortality. Lockdowns are defined as the imposition of at least one compulsory, non-pharmaceutical intervention (NPI). NPIs are any government mandate that directly restrict peoples’ possibilities, such as policies that limit internal movement, close schools and businesses, and ban international travel. This study employed a systematic search and screening procedure in which 18,590 studies are identified that could potentially address the belief posed. After three levels of screening, 34 studies ultimately qualified. Of those 34 eligible studies, 24 qualified for inclusion in the meta-analysis. They were separated into three groups: lockdown stringency index studies, shelter-in-place-order (SIPO) studies, and specific NPI studies. An analysis of each of these three groups support the conclusion that lockdowns have had little to no effect on COVID-19 mortality. More specifically, stringency index studies find that lockdowns in Europe and the United States only reduced COVID-19 mortality by 0.2% on average. SIPOs were also ineffective, only reducing COVID-19 mortality by 2.9% on average. Specific NPI studies also find no broad-based evidence of noticeable effects on COVID-19 mortality.
While this meta-analysis concludes that lockdowns have had little to no public health effects, they have imposed enormous economic and social costs where they have been adopted. In consequence, lockdown policies are ill-founded and should be rejected as a pandemic policy instrument.
=============================================
8) 12 Countries Roll Back COVID Restrictions, Israel Scraps ‘Green Pass’
By Megan Redshaw
Sweden and Switzerland joined Denmark, Norway, Finland, Ireland, The Netherlands, Italy, Lithuania, France and the UK in announcing they will lift COVID restrictions and open up their countries. ending all Covid restrictions.
9) Israel to Scrap COVID Green Pass for Most Entertainment Venues From Sunday Michael Hauser TovIdo Efrati Feb. 1, 2022
“Israel’s coronavirus cabinet decided to abolish its so-called green passport program for most places of entertainment, including hotels, restaurants, gyms and movie theaters, effectively removing barriers to entry for the unvaccinated.”
10) Truth Is Winning in the COVID Wars Mary Claire Kendall Jan 31, 2022
The War Against Repurposed Drugs
11) Dr. Pierre Kory: The War on Hydroxychloroquine, Ivermectin, and Other Cheap Drugs to Treat COVID-19 American Thought Leaders JAN JEKIELEK transcript from Jan 29, 2022.
12) The Global Disinformation Campaign to Suppress The Evidence of Efficacy of Ivermectin
After a week of non-stop lectures, panels, speeches, and expert testimony, my new mission has now come into focus. Pierre Kory, MD, MPA Feb 1 2022
===================
Negative Efficacy of Covid Vaccines for Omicron
13) DEVASTATING negative efficacy UK COIVD data week 4, 2022; BOOSTER data; COVID-19 vaccine surveillance report Week 4, 27 January 2022, relative to week 3 by Paul Alexander January 30, 2022
14) Data from highly vaccinated countries suggests strongly that the answer is yes; vaccinated people are at higher risk of infection from Omicron. Alex Berenson Jan 6 2022
vaccinated people are 8X more likely to develop Omicron than unvaccinated people
15) New studies show that the COVID vaccines damage your immune system, likely permanently
The vaccines are making it more likely you’ll be infected with Omicron 90 days after you are fully vaccinated. To keep vaccine effectiveness high against omicron, vaccination every 30 days is needed. Steve Kirsch Dec 24, 2021
Update Jan 7, 2022: The numbers in the Denmark study described below are now confirmed by government data from Germany showing that vaccinated people are 8X more likely to develop Omicron than unvaccinated people. This is not surprising since a paper from Germany showed the same thing: the more you vaccinate, the worse it gets.
Worried about Omicron? Guess what? After 90 days, the vaccine they gave you is going to make you MORE likely to get infected from Omicron, not less. The longer you stay on the vaccine treadmill, the harder to get off in the future and the easier you’ll make it for the virus.
=======================================================
Life Insurance Companies Report 40% Increased deaths working ages
16) Indiana life insurance CEO says deaths are up 40% among people ages 18-64 By Margaret Menge | The Center Square contributor Jan 1, 2022
Just to give you an idea of how bad that is, a three-sigma or a one-in-200-year catastrophe would be 10% increase over pre-pandemic,” he said. “So 40% is just unheard of.”
The number of hospitalizations in the state is now higher than before the COVID-19 vaccine was introduced a year ago, and in fact is higher than it’s been in the past five years, Dr. Lindsay Weaver, Indiana’s chief medical officer, said at a news conference with Gov. Eric Holcomb on Wednesday.
17) Life insurance deaths up 40% – Dr. Robert Malone’s chilling analysis
by Justus R. Hope, MD and Robert Malone, MD Jan 6, 2022
18) FDA report finds all-cause mortality higher among vaccinated
FDA report shows Pfizer’s clinical trials found 24% higher all-cause mortality rate among the vaccinated compared to placebo group. David Rosenberg
The FDA report, however, revealed a larger number of deaths by all causes in both groups, with 17 deaths among the control group and 21 in the vaccinated cohort.
20) “80% of serious COVID cases are fully vaccinated’ says Ichilov hospital director Vaccine has “no significance regarding severe illness,” says Prof. Yaakov Jerris. Israel National News Feb 3, 2022
=====================================
Masks Do Not Work
Masks don’t work.So why were “experts” hailing the Bangladesh mask study as proof that masks work? Because they were so desperate to point to something to support their belief system–even a study that was worthless. Steve Kirsch Nov 27, 2021
Are Face Masks Effective? The Evidence.
Updated: January 2022 First published: July 2020
Conclusion Face masks in the general population might be effective, at least in some circumstances, but there is currently little to no evidence supporting this proposition. If the coronavirus is primarily transmitted via indoor aerosols, face masks are unlikely to be protective. Thus, health authorities should not assume or suggest that face masks will reduce the rate or risk of infection.
================================================
JUST IN: Facebook has banned the rapidly growing “Convoy to DC 2022” group from its platform after it gained some 137,000 members.
=======================================================
———————————————
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Copyright (c) 2022 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on February 4th, 2022 by Jeffrey Dach MD
The post Failed Pandemic Public Health Policy Who is to Blame ? appeared first on Jeffrey Dach MD.
January 25, 2022
Top Experts Join Senator Ron Johnson in Panel Discussion
 Top Experts Join Senator Ron Johnson in Panel Discussion
Top Experts Join Senator Ron Johnson in Panel Discussion
COVID-19: A Second Opinion, Senator Ron Johnson
Monday January 24, 2022. This is the panel of experts that should have been governing public health policy since the beginning of the pandemic…
Peter McCullough, Robert Mallone, Pierre Kory, Paul Marik, Ryan Cole, Harvey Risch and many others,
——————————————————————————————-
View All 5 hours of testimony. Scroll forward 40 minutes to start of talks.
——————————————————————————————-
Letter to a Governing Body Margaret Anna Alice Jan 11 2022
ââââââââââââââââââ
Articles with Related Interest:
Peter McCullough on Early Treatment vs Vaccination
Inventing the Covid Virus and Vaccine
Trick or Treat from the Demon Doctor ?
Pharmacies and TeleMed Services Providing Ivermectin
Robert Malone on the Covid War Games
Covid Conversation RoundTable San Juan Global summit
More Cov-idiocy from the Clown Department
Israel Should Stop Pfizer and Start Ivermectin Distribution
Causalties of the C0\/lD War, When Wlll this End ?
Rochelle Wolensky Warns of ADE Antibody Dependent Enhancement
Covid Vaccines Are Safe and Effective ?
Are Covid Vaccines the Next Vioxx ?
Ivermectin and the Failure of American Medicine
Ivermectin Antiparasitic Anticancer Miracle Drug
Vaccinoffee, a Vaccine with Every Coffee
Useful Resources:
Covid Patient Home Treatment Guide AAPS
Telemedicine Services to Obtain Ivermectin
Unity Project Online: Working together to STOP COVID-19 Vaccine Mandates for Healthy Children K-12
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
www.drdach.com
Heart Book by Jeffrey Dach
âââââââââââââââ
Click Here for: Dr Dachâs Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dachâs Online Store for Natureâs Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician â patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Copyright (c) 2022 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a âfair useâ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on January 25th, 2022 by Jeffrey Dach MD
The post Top Experts Join Senator Ron Johnson in Panel Discussion appeared first on Jeffrey Dach MD.
Jeffrey Dach's Blog

- Jeffrey Dach's profile
- 3 followers


{kind=link}
{kind=link}
{kind=link}