
Aaron E. Carroll's Blog, page 27
March 2, 2022
HSR Author Instructions Part 2: Manuscript Formatting and Submission Requirements
This post is part of a series explaining aspects of the author instructions (see also the checklist) for Health Services Research (HSR) as they existed circa March 2022. Each post quotes portions of the instructions and explains their import. Neither these posts nor the checklist are a substitute for reading and following the full set of instructions, which is expected of all authors for all submissions.
This post focuses on portions of Section 2 of the author instructions, which is about manuscript formatting and submission requirements. This is probably the section of greatest interest to authors submitting manuscripts, yet some recommendations and requirements are frequently overlooked. I’ll focus on those in this post.
Section 2.2: “HSR publishes the following types of papers in its regular issues: Research Articles … Research Briefs … Methods Articles and Methods Briefs … Commentaries …”
Each of these article types has its own focus and the requirements and recommendations for each vary. This is all documented in the instructions, so I won’t repeat it all here. I do want to emphasize just a few points:
Research or Methods Briefs are particularly appropriate for studies that “make incremental contributions to the literature”. These include, for example, “single-setting studies (with an argument for the generalizability of findings to other sites).”Commentaries are by invitation only, though authors may submit a proposal for a commentary (see instructions for details on how to do so). Commentaries must be evidence-based and “organized into thematic sections with subheadings.”Section 2.3: This section includes a table that briefly summarizes some of the key requirements for article types, like word limits, abstract formatting, and so forth. Whether on initial or revised submission, authors may not exceed word limits without prior approval.
Section 2.4: This section has vast detail about how to prepare a manuscript, with instructions that go document-by-document and section-by-section. Some key points:
Instructions for what must be included in the cover letter are found in Subsection 2.4.1. For the most part, authors will also find the same instructions as they submit and answer the required questions online that pertain to prior disclosure or publication of findings, age of data (explanation required if >5 years old), and conflicts of interest.Subsection 2.4.2 has instructions for the main manuscript file and is probably of greatest interest to authors. A few things are commonly overlooked, however, so warrant emphasis:Throughout the manuscript, “for reporting findings about or discussing race and ethnicity, we recommend that authors follow the AHA/ASA Journals Disparities Research Guidelines and JAMA guidance on reporting of race and ethnicity.”“For quantitative analyses, we recommend authors follow the general statistical guidelines provided by the Annals of Internal Medicine.” In addition, “[r]eporting of odds ratios is discouraged (marginal effects preferred) except in case-control studies (see Norton and Dowd DOI: 10.1111/1475-6773.12712 and Norton et al. DOI: 10.1001/jama.2018.6971).“Titles should not include abbreviations or punctuation, including colons, dashes or question marks.The Acknowledgements should list funding sources, even for the anonymized version sent to reviewers.The Objective of the structured Abstract should begin with “To …”The Principle Findings of the structured Abstract should “present numerical results (absolute numbers when available and rates only if not available) with appropriate indicators of uncertainty, such as confidence intervals. Do not report the results of statistical hypothesis testing alone, such as P values, which fail to convey important quantitative information.”Each section of the callout box (What is known on this topic/What this study adds) should be up to three bullets long with each bullet no longer than 30 words. Bullets should be written for a wide audience. For each published paper, we use these as tweets in a thread, so think of them, and write them, that way.Tables and Figures should be understandable on their own, without reference to the text. This will require meaningful titles, definitions of all abbreviations. Though I haven’t done a quantitative study, it feels like the majority of manuscripts have tables and figures with abbreviations without definition. It’s not in your interest to overlook this, as editors and reviewers may not recall the definition of everything from the main text when they turn to your tables and figures. Then they become confused or frustrated, which you don’t want.Abbreviations: “[T]erms should not be abbreviated unless they are used repeatedly and the abbreviation is helpful to the reader. Initially, use the word in full, followed by the abbreviation in parentheses. Thereafter use the abbreviation only. We discourage the use of abbreviations that are not already in common use, or that may have more than one meaning. Abbreviations used in the abstract, callout box, main text, tables, and figures should be separately defined in each.”Again, there is lots more in the instructions. I’m just hitting the main points that are most frequently overlooked. Next in this series, I’ll cover several part of the Editorial Policies and Ethical Considerations section
The post HSR Author Instructions Part 2: Manuscript Formatting and Submission Requirements first appeared on The Incidental Economist.

March 1, 2022
Hospitals Often Charge Uninsured People More Money
Health insurance: the holy grail of the US hospital patient. While it isn’t perfect, it does often make a big difference in a patient’s bottom line. That’s not only because it helps pay the bills – it turns out that when you don’t have health insurance, you might get a bigger bill from the hospital in the first place. Makes perfect sense, right?
The post Hospitals Often Charge Uninsured People More Money first appeared on The Incidental Economist.
HSR Author Instructions Part 1: Aims and Scope
This post is part of a series explaining aspects of the author instructions (see also the checklist) for Health Services Research (HSR) as they existed circa March 2022. Each post quotes portions of the instructions and explains their import. Neither these posts nor the checklist are a substitute for reading and following the full set of instructions, which is expected of all authors for all submissions.
This post focuses on portions of Section 1 of the author instructions, which includes some common reasons for desk rejection, as well as indicates the kinds of papers we do consider for publication.
Section 1.: “… We focus on methods, concepts, and results related to the financing, organization, delivery, evaluation, and outcomes of health services…”
This is, perhaps, the aspect of HSR‘s focus, vision, mission, and values that accounts for the most desk rejections. If a manuscript is not within this scope, it’s not a good fit for the journal.
Section 1.1: “…Areas of interest include … Studies that report on important new data sources … Studies on biological, behavioral, social, and political factors—including structural racism—in addition to health care, as determinants of health outcomes … Articles that advance health services research by developing, demonstrating, or rigorously validating qualitative and quantitative methods…”
These are not the only areas of interest (read the full Section 1.1 of the author instructions). But these are worth pointing out to emphasize that HSR‘s scope includes papers on new data, non-health care factors that affect health outcomes, and methods articles.
Section 1.2: “HSR typically does not consider … Preliminary or scoping reviews … Case studies from a single site, in the absence of a reasonable argument for the generalizability … Simple pre-post (uncontrolled) studies … Studies whose most recent data are >5 years old unless the cover letter and manuscript provide a valid reason…”
These are all common reasons for desk rejections.
Section 1.3: “…[S]tudies of health services in countries other than the US [must include] direct, analytic comparison to US practices … The cover letter and Discussion section for any submission from outside the US should explain why the article is pertinent or salient to US health care.”
Also a common reason for desk rejection.
That’s it for Section 1, which is relatively short. Section 2 (Manuscript Formatting and Submission Requirements), on the other hand, is quite long and is covered in the next post of this series.
The post HSR Author Instructions Part 1: Aims and Scope first appeared on The Incidental Economist.February 24, 2022
Healthcare Triage Podcast: The Role of Publishing in the Reproducibility Crisis
In academia, publishing is “the coin of the realm”. How does the reproducibility of our work suffer under this “publish or perish” system? In this fourth episode of our special series on science culture and reproducibility, we talk about the pressure to publish splashy research in high-value journals, and how those pressures influence what kind of research gets funded.
The post Healthcare Triage Podcast: The Role of Publishing in the Reproducibility Crisis first appeared on The Incidental Economist.
Healthcare Triage Podcast: The Role of Funding in the Reproducibility Crisis
In academia, publishing is “the coin of the realm”. How does the reproducibility of our work suffer under this “publish or perish” system? In this fourth episode of our special series on science culture and reproducibility, we talk about the pressure to publish splashy research in high-value journals, and how those pressures influence what kind of research gets funded.
The post Healthcare Triage Podcast: The Role of Funding in the Reproducibility Crisis first appeared on The Incidental Economist.
February 23, 2022
Healthcare Triage Podcast: The role of funding in the reproducibility crisis
Now that we’ve covered what the reproducibility crisis is and why we think it’s happening, it’s time to dig into specific issues, starting with funding. The way that science is funded has changed a lot over time. What are those changes and how have they affected the way we practice science?
The post Healthcare Triage Podcast: The role of funding in the reproducibility crisis first appeared on The Incidental Economist.
Sleep Myoclonus Support
I have suffered from sleep myoclonus for over two years.* I haven’t written much about it (a little here, in the early days) and don’t know if I will write much more. I have many other things to which to devote my limited time and energy.
But, in brief, it’s an exceedingly rare sleep movement disorder with little research and no known cures. It’s extremely disruptive — life, mood, and mind altering. It’s torture.
Because there’s not much known about it, patients are largely left to find their own path with little support. It’s not easy to find doctors who get it. If you’re a sufferer, keep hunting for one. You may need someone to prescribe a variety of meds in rapid succession (including those they are wary of prescribing) as you search for one or several that may help. If you’re like me, you’ll want a wide variety of meds and supplements on hand to adjust to the changing condition and your evolving understanding of what works and when. You’ll need to become your own pharmacist.
There is some patient-to-patient support too, which I’ve finally found, after searching on and off for a year. So, to help others find the resources I have, here they are:
A Facebook patient support group (registration required): Hypnic Jerk*/Sleep Myoclonus Support — This is where I’m contributing my experience and getting ideas for help. As of this writing, the group has 1.6k members.A blog about someone who has the condition: The Man Who Cannot Sleep — If you want to understand the experience of the condition, this is where to look. Though his experience is not identical to mine, it’s close enough. He speaks for me. I won’t write my story out here (or not yet). His blog is not easy to navigate. When you land on the page linked to above, scroll to the bottom for the archives. The comments on posts are also very useful for treatment ideas.A website devoted to the condition: HypnicJerking.com* — There are posts from patients that document their experience and, sometimes, what works for them to address the condition. A few other gems are this patient registry, this podcast episode, which is part of the Carnivore for Life podcast, and this page of support resources.Feel free to contact me if you have this condition.
* Some call it “hypnic jerking” but I think that’s a mistake. That term is too widely used for the benign twitches most people experience when falling asleep and are NOT disruptive. Sleep myoclonus is highly disruptive, and I advocate using that term only.
The post Sleep Myoclonus Support first appeared on The Incidental Economist.February 22, 2022
Healthcare Triage Podcast: Why is the reproducibility crisis happening?
Now that we’ve covered the “what” of the reproducibility crisis, it’s time to talk about the “why”. Why would scientists engage in practices that compromise the integrity of science? Let’s talk about incentives.
The post Healthcare Triage Podcast: Why is the reproducibility crisis happening? first appeared on The Incidental Economist.
Vaccine Monopolies: Innovation and Inequity
This article is part of an educational video series created by BUSPH student, Tasha McAbee, and health economist, Dr. Austin Frakt, to explain the intersections of economics and health. The transcript follows the video below, which can also be found on YouTube at Health Economics Explainers.
The Covid-19 vaccines were a miraculous helping hand to a disastrous pandemic in the US. The vaccines were developed quickly and are highly effective.
But after production, comes distribution. And in an ongoing pandemic, a massive amount of the newly invented vaccine needs to be distributed as fast as humanly possible to put an end to the spread of disease.
Normally, production of a good or service could be increased by having more companies enter the market and contribute. The competition also helps keep prices affordable. But when a new pharmaceutical is invented, the United States government protects the developers from competition for a number of years by granting them patents and market exclusivity, rewarding them for their innovation with profit. The Covid-19 vaccine developers were no exception.
These governmental protections grant pharmaceutical and vaccine developers market power they would not otherwise have. In some cases they are able to act as monopolies. Although there are multiple Covid-19 vaccines, there is relatively little competition, so it’s useful to examine the effect monopolies have on production and price to understand what’s going on with the vaccines.
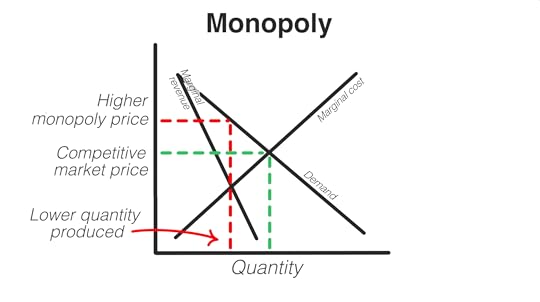
In a true monopoly, the supply curve is the additional cost to produce more of a good or service, called the marginal cost, which increases as the quantity produced increases, also causing the price to increase.
The demand curve, just as in competitive markets, is downward sloping because people will buy less of something the higher the price.
When deciding what quantity to produce, monopolists, seeking to maximize profit, look to where marginal cost meets marginal revenue, which is the additional revenue they earn from each unit they produce. Marginal revenue is also downward sloping and is steeper than the demand curve. Where these two values meet indicates the price and quantity at which the company will earn the most profit from sales, without losing money on production.
But this quantity is lower than what would be produced in a competitive market.
And the monopolist has the power to still charge a price matching the demand, while producing at the lower quantity.
While this is great for the company’s profits, low production and high prices can be a huge problem when a global population of 7.8 billion people are all in need of the same vaccine at the same time, as in a pandemic. Despite not being a true monopoly, the governmental protections granted to the few Covid-19 vaccine companies is causing this effect on production and prices of vaccines. The companies aren’t producing at a high enough rate to meet demand, and what they do produce has a high price, making vaccines both inaccessible and unaffordable to many, especially to low-income countries.
There have been calls to suspend intellectual property rights on the Covid-19 vaccines. A waiver would ensure that vaccine companies could not block others from producing vaccines, allowing more companies to join in production and help supply the world with enough vaccines, at a price more affordable to low-income countries.
The Covid-19 vaccines aren’t alone in this problem. Monopolies — or situations close to them — plague many vaccine and drug markets. The only two HPV vaccine developers, together maintaining a duopoly through similar government protections, is estimated to profit at 10 times the cost of production of the vaccine while the vaccines remain inaccessible to many in low-income countries. Keytruda, a breakthrough cancer drug, was granted 53 patents, gaining 35 years of protection from market competition. Without competition, the individual cost for a one year supply of treatment with Keytruda is over $100,000, making it inaccessible to many patients.
Governmental investment in innovation is essential and was crucial to the development of new vaccine technologies that were used in various Covid vaccines. However, the current system of creating monopolies has adverse consequences for equity. The Covid-19 pandemic is the latest example of why the US may need to find a different way of rewarding companies for innovation, one that doesn’t limit supply and risk the public’s health.
The post Vaccine Monopolies: Innovation and Inequity first appeared on The Incidental Economist.February 21, 2022
Can Text Messages Increase Vaccination Rates?
Remember last week’s episode on the exercise megastudy? Well, there’s another megastudy in existence! This time on using text message reminders to encourage people to get vaccinated for the flu. We’ve got the deets for you on today’s episode.
The post Can Text Messages Increase Vaccination Rates? first appeared on The Incidental Economist.Aaron E. Carroll's Blog

- Aaron E. Carroll's profile
- 42 followers

