
Aaron E. Carroll's Blog, page 136
May 5, 2017
Healthcare Triage News: Narrow Insurance Networks Limit Access, Especially for Kids
Narrow health insurance networks cover fewer doctors, and can be especially narrow when it comes to specialists. And, it turns out, this limited access to specialists disproportionately affects children. This is Healthcare Triage News:
This episode was adapted from a blog post I wrote for the AcademyHealth blog. Go read more there:


May 4, 2017
The AHCA and the ACA in two charts
The House passed the American Health Care Act (AHCA) this afternoon. It’s still a considerable way from becoming law, but if it does it will repeal the Affordable Care Act (ACA). Here are two charts that explain why this happened.
The first chart is from Henry Aaron of the Brookings Institution (previously discussed here). For each decile of the US income distribution, it projects the income gains and losses from the ACA, where the cash value of the health insurance benefit is treated as income. The positive bars on the left are income gains by the people in the lowest 20% of the US distribution. They are balanced by losses in the upper 80% of the income distribution.

Transfer effects of the ACA, by Henry Aaron at the Brookings Institution.
Next is a similar chart from the Urban Institute on the net transfer effects of the AHCA.

Transfer Effects of the AHCA, from the Urban Institute.
The horizontal axis on the Urban Institute graph represents income ranges, not income deciles. The four bars that are positive on the right represent people making $50,000 or more (the upper 37% of the US income distribution). The bar on the far right, with the huge positive income transfer, represents people earning $200,000 or more (the top 0.33% of the income distribution). Notice also that the vertical axis of the Brookings chart represents percentage changes in income, whereas the axis in the Urban Institute chart represents changes in dollars. If you converted the Urban Institute chart to percents, the magnitude of the bars on the left (low) side would grow and those on right (high) side would shrink. The Institute projects that the average person earning $200,000 or more will get a 1% increase in income. They project that the average person earning less than $10,000 will experience a 33% net loss of income. Think about that for a moment.
Here is why the AHCA is moving forward. The ACA used tax funds to pay for the healthcare of people in the bottom 20% of the income distribution. High earning people pay most of the taxes, so the ACA transferred money from them down to people in the bottom deciles of the US economic hierarchy. The AHCA cuts taxes in the ACA and reduces the amount that the government will spend on the health care of the poor. The net effect of the AHCA is a massive loss for the poor and a benefit for the very top of the economic scale.
I would love to be able to say that these bills represent clashing views about the best way to deliver health care. Unfortunately, I am unable to find a conservative health policy expert who thinks the AHCA is optimal. There may not be one who thinks it’s even good. The AHCA did not pass based on its merits as a health policy solution. The AHCA passed because Republicans wanted these transfer effects.
The Michigan Morsel
To corral some last-minute votes, the House leadership has endorsed the Upton amendment to the American Health Care Act. The legislative text was released late yesterday, giving members no time to understand what it does before they vote on it today. That’s a shame: the amendment works at cross-purposes with other parts of the AHCA, is arbitrarily structured, and is ambiguous on a key point. It’s another example of the perils of doing health policy on the fly.
Under the earlier MacArthur amendment to the AHCA, states can apply for waivers from some of the Affordable Care Act’s rules, including the rule that insurers can’t take health status into account when setting rates. In waiver states, insurers will be allowed to hike the premiums of people with preexisting conditions who have a lapse in coverage.
The goal is to encourage healthy people to maintain continuous coverage—a Republican-friendly substitute for the individual mandate. You want to go without insurance? Fine. But you’ll be fenced out of the insurance markets if you develop some terrible disease.
That’s a harsh policy, but it’s an explicable one. (Waivers might also undermine community rating for people without a coverage gap, as Matthew Fielder expertly explains. But let that pass for now.) What’s more, the policy responds to a genuine problem: without the individual mandate, and with savage cuts to ACA subsidies, the exchanges will have a hard time attracting healthy enrollees. The 30% continuous-coverage penalty is too small to make a difference. With a waiver, however, the states can pull out the big guns.
If you believe in the MacArthur amendment—if you believe in it so much that that’s what it took to secure your support for the AHCA—the last thing you’d want to do is dilute the penalty for going without coverage. But that’s exactly what the Upton amendment does.
The amendment appropriates $8 billion over five years and gives it to those states that allow insurers to discriminate against people based on their health status. The money must be used “for the purpose of providing assistance to reduce premiums or other out-of-pocket costs of individuals who are subject to an increase in the monthly premium rate for health insurance coverage as a result of [a] waiver.” In other words, the state will offer you some financial assistance when an insurer charges you more because of a preexisting condition.
As a policy matter, this makes no sense. If you think it’s cruel to withhold insurance from people with preexisting conditions, then you should retain the rule banning discrimination on the basis of health status. Instead, the Upton amendment tries to correct a problem that the AHCA itself creates.
And it’s an arbitrary correction. The new money can only go to waiver states, but we don’t know how many states will seek waivers. If only Wyoming gets a waiver, an extra $1.6 billion per year will be enough to fully subsidize coverage for everyone in the state. But if all the states with Republican governors opt for waivers, the $8 billion will dwindle into insignificance. (That’s why Dan Diamond dubbed the amendment “the Michigan morsel.”)
In other words, the degree to which you will be punished for having a lapse in coverage doesn’t turn on a finely calibrated judgment about incentive effects or how much responsibility you should bear for going without insurance. It turns on the number of states that sign up for waivers. In what world is that good policy?
The Upton amendment could even exacerbate the problem it aims to address. By dangling money, the amendment encourages states to sign up for waivers. But if more waivers are granted, more people will be subject to discrimination based on their health status. At the same time, every new waiver means less money for all the other waiver states—meaning less money, per capita, to support those who can’t afford a risk-rated premium. With less financial support, more people will find it impossible to afford insurance. The amendment could thus increase the overall number of people who lose coverage because of their preexisting conditions.
There’s more. Some reporting has suggested that the $8 billion could go toward state high-risk pools. But the amendment’s text is squirrelly about whether that’d be permitted. High-risk pools do offer “assistance” in the abstract. But is it “assistance to reduce premiums or other out-of-pocket costs” for people who are “subject to an increase in the monthly premium rate for health insurance coverage”? The Upton amendment seems to anticipate that states will defray the cost of exchange plans for people with preexisting conditions—not shunt them to a high-risk pool.
If that’s right, the amendment will introduce another layer of complexity to the enrollment process. If you’ve had a gap in coverage, you’ll need to submit a big packet of health information. After reviewing your information, the insurer will then give you a risk-adjusted rate. Only then will the state step in to subsidize your coverage, with the amount of any reduction depending on how many states have signed up for waivers and how many other people in your state also need financial support. Instead of quick and relatively painless on-line process, enrolling for coverage will be intrusive and protracted.
It’s crazy to adjust the basic structure of the American Health Care Act the day before House members are expected to vote for it. It’s crazier still to do so when the change is incoherent, arbitrary, and technically complex.
May 3, 2017
Some further thoughts on SMT and hypocrisy
When I have a sore throat, I like to drink hot tea. I don’t for a minute believe that the tea is “curing” my sore throat. But it provides me with symptomatic relief, so I like it. I don’t have an RCT to prove to me it’s reducing pain, so it might even be a placebo effect. I don’t care. Tea is cheap, it’s non-invasive, it has relatively few adverse effects (although I’m sure you can find me an anecdote or two showing someone who burned themselves terribly or something), and I’m not asking insurance to pay for it.
When some people have back pain, they go for spinal manipulation therapy. They shouldn’t for a minute believe that SMT is “curing” their bad back. It may provide them with symptomatic relief, though. There are RCTs to show that SMT works as well as other therapies we prescribe. It’s cheaper than many traditional therapies, it’s non-invasive, it has relatively few adverse effects (although you can find anecdotes of harm, especially if people have their neck manipulated), and it’s pretty much all out-of-pocket spending.
What’s the difference between the first and the second paragraph? The cost? Where you get the intervention? The fact that there’s more evidence for the SMT than for tea?
I’ve gotten a lot of anger from this last column, mostly from physicians. Osteopaths are angry I didn’t single them out as already knowing about the benefits of SMT and naming them good deliverers of it. MDs are angry at me for saying that anyone should think about SMT in the first place.
The latter argue that the evidence is weak. I agree, the data could be better. The data are crappy on almost every single back pain intervention, though. They argue that I’m giving SMT an easier bar to hurdle because it’s an alternative therapy. That’s not why. I’m giving it a lower hurdle to pass because it’s non-invasive, has few adverse effects if done right, it’s OOP and entirely up to individuals to buy, and it appears to work as well as the many other things we recommend for back pain all the time.
It’s like tea. I could take a pain med for my sore throat (which doesn’t work that well), or I could drink the tea. I choose the latter.
If you don’t want the SMT, that’s fine. Really. You could try heat. Or accupuncture, massage, yoga, etc. They’re all pretty safe, cheap, non-invasive, and it’s your money. Or, you could try some short term NSAIDS. Feel free. Guess what? It really doesn’t matter. The back pain is likely to resolve on its own, no matter what you do, and these things all seem to help equally along the way.
That’s what I said. That’s what I stand by. If you disagree, and think traditional medicine is better here, then I encourage you to find the evidence saying that’s so. Otherwise, shrug like me, and admit that maybe you don’t know.
For Bad Backs, It May Be Time to Rethink Biases About Chiropractors
The following originally appeared on The Upshot (copyright 2017, The New York Times Company).
About two of every three people will probably experience significant low back pain at some point. A physician like me might suggest any number of potential treatments and therapies. But one I never considered was a referral for spinal manipulation.
It appears I may have been mistaken.
For initial treatment of lower back pain, it may be time for me (and other physicians) to rethink our biases. Spinal manipulation (applying pressure on bones and joints) — along with other less traditional therapies like heat, meditation and acupuncture — seems to be as effective as many other more medical therapies we prescribe, and as safe, if not safer.
Most back pain resolves over time, so interventions that focus on relief of symptoms and allow the body to heal are ideal. Many of these can be nonpharmacological in nature, like the work done by chiropractors or physical therapists.
Physicians are traditionally wary of spinal manipulation, in part because the practitioners are often not doctors and also because a few chiropractors have claimed they can address conditions that have little to do with the spine. Patients with back pain haven’t seemed as skeptical. A large survey of them from 2002 through 2008 found that more than 30 percent sought chiropractic care, significantly more than those who sought massage, acupuncture or homeopathy.
Researchers have been looking at the evidence supporting spinal manipulation for some time. Almost 35 years ago, a systematic review evaluated the available research, most of which was judged to be low in quality, and found that there might be some short-term benefits from the procedure. Two reviews from 2003 agreed for the most part, finding that spinal manipulation worked better than a “sham procedure”, or placebo, but no better or worse than other options.
Almost a decade later, a Cochrane review assessed the literature once more, and found 12 new trials had been conducted. This review was more damning. It found that spinal manipulation was no better than sham interventions.
But since then, data have accumulated, as more higher-quality studies have been performed. Recently, in The Journal of the American Medical Association, researchers looked for new studies since 2011, as well as those that had been performed before.
The evidence from 15 randomized controlled trials, which included more than 1,700 patients, showed that spinal manipulation caused an improvement in pain of about 10 points on a 100-point scale. The evidence from 12 randomized controlled trials — which overlapped, but not completely with the other trials — of almost 1,400 patients showed that spinal manipulation also resulted in improvements in function.
In February, in Annals of Internal Medicine, another systematic review of nonpharmacologic therapies generally agreed with the other recent trials. Based upon this review, and other evidence, the American College of Physicians released new clinical practice guidelines for the noninvasive treatment of subacute back pain. They recommended that patients should try heat, massage, acupuncture or spinal manipulation as first-line therapies.
The only things that might detract from the use of spinal manipulation in this situation would be its cost and potential harms.
Because they fear those potential harms, some physicians are hesitant to refer patients to chiropractors or physical therapists for care. But in all the studies summarized above, there were really no serious adverse events reported. It’s possible to find anecdotes of harm to the spinal cord from improper manipulations, but these are rare, and almost never involve the lower spine.
Some physicians are concerned about the cost of spinal manipulation, especially since most insurance carriers don’t cover it. Visiting a chiropractor costs more than taking many non-narcotic pain medications. But more invasive interventions can cost a lot of money. In addition, studies have shown that, in general, users of complementary and alternative medicine spend less over all for back pain than users of only traditional medicine.
Medication and surgery can also lead to harms. We shouldn’t forget that prescription pain medications, like opioids, can lead to huge costs, especially when they’re misused.
Some physicians are uncomfortable that we don’t have a clear picture of how spinal manipulation actually works to reduce pain. It’s also possible that some chiropractors do it “better” than others, and we can’t tell. This concern should be tempered by the fact that we don’t have a great understanding of why many other therapies work either. Some of the more traditional things we recommend don’t even work consistently.
Still, there is no merit to many other claims about spinal manipulation — that it has been proved to work for things like infantile colic, painful periods, asthma, gastrointestinal problems, and more. For most conditions, the therapy lacks a good evidence base.
But given the natural course of back pain — that most of it goes away no matter what you do — the ideal approach is to treat the symptoms and let the body heal. Noninvasive therapies seem to do that well enough.
May 2, 2017
Healthcare Triage: Orphan Drugs part 4 – Fixing the System
Drug companies love the Orphan Drug Act. They say it encourages research into breakthrough therapies for people with rare disease. And sometimes that’s true. Lots of the time, though, the companies would’ve pursued the research anyhow. And those same companies have learned to game the Orphan Drug Act in a bunch of different ways, allowing them to jack up their prices for no good reason.
How could we fix the Orphan Drug Act? That’s the topic of this week’s Healthcare Triage.
Sources can be found in the posts Nick has written on the subject! Special thanks to him!
I have a pre-existing condition. I do things “the right way”.
When I was a medical student, I started to notice blood in the toilet. I was a medical student, so I panicked. I called my father, who at the time was still a practicing surgeon, and he told me it was likely hemorrhoids. Given the alternatives, I breathed a sigh of relief.
The blood didn’t go away, though. Soon, I started to have diarrhea, cramps, and the urge to go to the bathroom all the time. That summer, I worked at Children’s Hospital of Philadelphia on a research project, and I had to go to the bathroom so many times, I thought they were going to fire me. It got so bad, my Dad (who is a minimalist), finally sent me to the gastroenterologist. The short version of the story is they determined I had ulcerative colitis.
I’ve written about this before, so I’m not going to get into the details of the disease. The only reason I bring any of this up is so you understand that I was diagnosed when I was 22 years old and a full-time student.
None of it was my fault.
Today, I eat a healthy diet. My weight is good. I exercise 5 times or so a week. I don’t smoke or do drugs. I don’t drink more than socially. I do everything I’m supposed to do. I still have ulcerative colitis, and I will until I die, likely. I’m doing the things I need to do to keep my body healthy. I lead a good life.
__________________________________________
I try very hard to see the good in others. When I write, when I debate others, I do my best to assume that the intentions of those with whom I disagree are righteous. Even when we see the world differently, I make every effort not to think that others are “bad” or want to see people suffer. I’m not one who writes that people who want to reform the insurance system want “to kill them”. I don’t think that people who want to reform welfare “hate the poor”. I’m not perfect, so sometimes I screw up. When I do, I apologize.
Yesterday, a Congressman went on TV and said (emphasis mine):
“My understanding is that it will allow insurance companies to require people who have higher health care costs to contribute more to the insurance pool. That helps offset all these costs, thereby reducing the cost to those people who lead good lives, they’re healthy, they’ve done the things to keep their bodies healthy. And right now those are the people—who’ve done things the right way—that are seeing their costs skyrocketing.”
I cannot adequately describe how much this enraged me. This is one of those things that you hear people say “the other side believes”, but discount. I don’t want to believe that people think this. I don’t want to believe that people think that some others deserve to be sick. I don’t want to believe that people equate being ill with a moral failing.
I didn’t do anything to get ulcerative colitis. I did nothing wrong. I lead a good life. I didn’t fail.
___________________________________________
My brother, amazingly enough, has Crohn’s disease; the Carroll GI protoplasm ain’t the best. When I was a resident, and he was a law student, we would talk often about how we would both have to work for very large companies or organizations in order to get health care. It was a fact of life. We both knew that on the individual market, no insurance company would touch us. Ever. Because of our pre-existing conditions, we’d be screwed for the rest of our lives.
He didn’t do anything wrong either, by the way. He was diagnosed in high school, and he was a really good boy, too.
I could start quoting statistics here, but what’s the point? A huge number of Americans have pre-existing conditions. They couldn’t get insurance on the individual market before the ACA because it was in insurance companies’ best interest not to issue them policies. It made good business sense. That didn’t mean it was right.
There is certainly a case to be made that people have some responsibility for their health. But the lines aren’t clear at all. It’s easy to point at smokers and say they’re doing something harmful and are raising costs for all of us. That’s why we can charge smokers more under the ACA. After that… it gets dicey.
Do you start regulating what people eat? What they drink? If you eat dessert, and I don’t, why should I have to pay for your healthcare? Should we charge people more if they drive cars (number one killer of children!)? I like to ski. That has risks. So does rock climbing. Or playing contact sports. Should we make them stop, or charge them more? What about people who scuba dive?
Should we start penalizing people who have different organs in their body than we do?
____________________________________________
I expect that this Congressman will soon be issuing a statement saying he was “taken out of context”. Something along the lines of “he misspoke”. But maybe not. Maybe he does believe what he said, that people who did things the right way are the ones who are healthy. If that’s the case, then I have just one question for him.
What did the baby born prematurely, the one with congenital heart disease, or the toddler with sickle cell disease, or the child with autism, or the girl with leukemia, or the boy with asthma, or the adolescent with juvenile arthritis, or the young woman with lupus, or the young man with testicular cancer, or the new mother with breast cancer, or the new father with inflammatory bowel disease, or the woman with familial heart disease, or the man with early onset Parkinson’s disease, or the retiring woman with Alzheimer’s disease, or the elderly man with lymphoma – what did they do wrong?
Did they lead bad lives?
I guess I had two questions. Take your time answering. I’ll wait.
Adjusting for inflation is tricky
Abe Dunn, Scott Grosse, and Samuel Zuvekas are right: In many health care analyses, it is important to adjust for inflation, but there are numerous price indexes to choose from for the job. Which one should you use?
Helpfully, the authors surveyed various measures of health care price inflation and provided guidance on which to use in various circumstances. Their paper also explains why price indexes differ.
One important way they differ is the extent to which they incorporate changes in consumption patters. Laspeyres and Paasche type indexes hold fixed the quantities of goods and services consumed. The former fixes them in a base period and the latter fixes them in the current period. The only things that change in such indexes are prices. As such, they could misrepresent the actual impact of prices because people and institutions respond by changing how much of various goods and services they consume.
Put it this way, if the price of a service in the index went from $1 per unit in the base period to $1 billion per unit in the current period, consumption would fall to zero. People would substitute something else that’s cheaper. Lasperyes and Paasche indexes would miss that trend, though in different ways. The former would show massive inflationary effects because the good is in the basket in the base period, while the latter would show no inflationary effects because the good is not in the basket in the current period.
A Fisher index is the geometric mean of a Laspereys and a Paasche index. That makes it responsive to changes in consumption patterns, though not necessarily reflective of how they change period-by-period. A chained index, on the other hand, continuously updates consumption patterns.
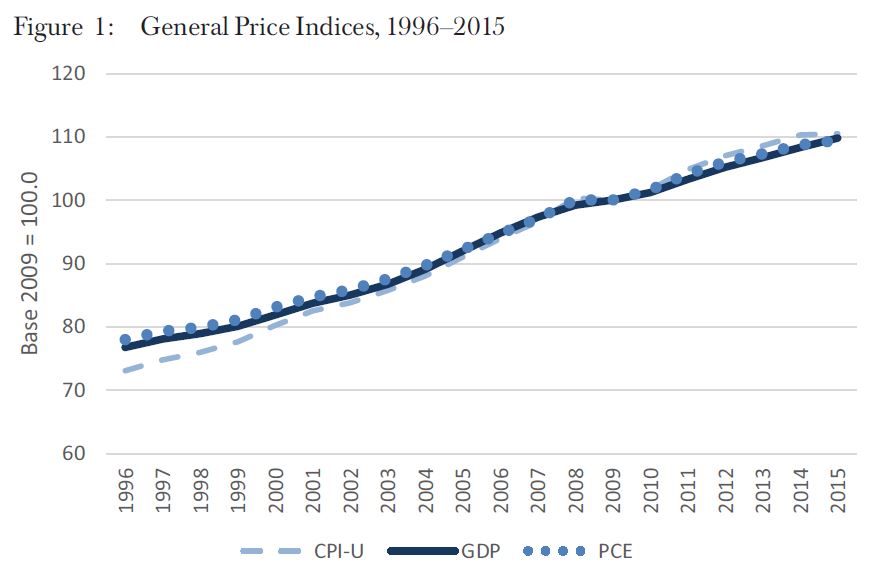
Another way price indexes differ is scope. Some indexes measure general price inflation, encompassing economic sectors beyond health care. Commonly used ones include the Gross Domestic Product (GDP), the Consumer Price Index—all urban consumers (CPI-U), and the Personal Consumption Expenditures (PCE) index. Some details:
GDP: A Fisher index that includes all sectors of economic activity (i.e., not just consumer spending). It is appropriate for adjusting for societal-level purchasing power changes.
CPI-U: A Laspeyres index that captures spending by urban consumers (i.e., excluding business and government spending, as well as consumption paid for on behalf of consumers by third parties). It is appropriate for adjusting for purchasing power changes in out-of-pocket spending.
PCE: A chained index that captures consumer spending, as well as that paid for by business, government and third parties on behalf of consumers. It is appropriate in the same circumstances as the CPI-U.
Despite the differences in how they address consumption changes and scope, these three indexes of general price inflation track one another relatively closely, as shown in Figure 1.
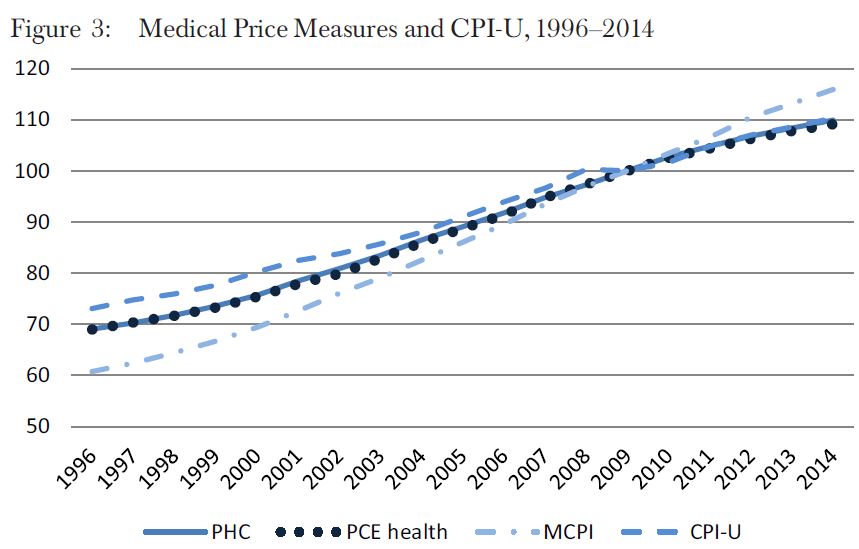
 Other indexes measure only health care price inflation. These include the Personal Health Care (PHC) deflator, Personal Consumption Expenditures-health (PCE health), and the Medical Care CPI (MCPI).
Other indexes measure only health care price inflation. These include the Personal Health Care (PHC) deflator, Personal Consumption Expenditures-health (PCE health), and the Medical Care CPI (MCPI).
PHC: A Fisher index that captures out-of-pocket and third-party health expenditures, excluding administration, research, and capital investment. It is appropriate for adjusting for general medical price changes. (Note, the National Health Expenditures (NHE) price index is an alternative that includes administration, research, and capital investment.)
PCE health: A chained index that is otherwise nearly identical to the PHC but has a longer history.
MCPI: A Laspeyres index designed to capture out-of-pocket health care spending, including that paid by individuals with private or Medicare Part B coverage. It is most appropriate for adjusting for out-of-pocket medical price changes.
The chart below (the authors’ Figure 3) shows the historical trends for these three indexes, alongside the CPI-U. All start below the CPI-U and then fall into line with it by the late 2000s, with the exception of the MCPI, which rises above the CPI-U. That the MCPI has a different trend than the other medical price indexes is not surprising, since it is the only one of the three focused exclusively on out-of-pocket spending.
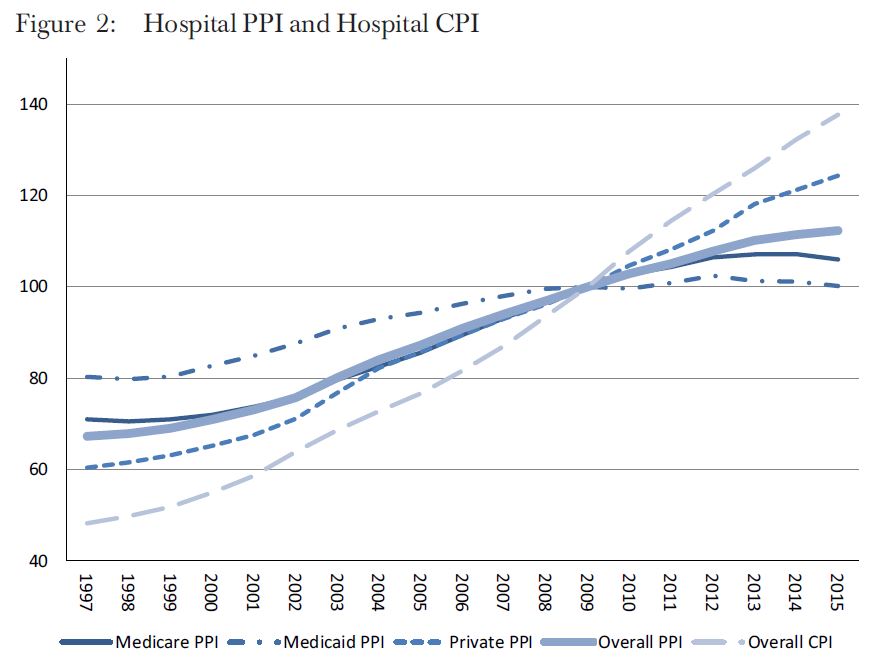
 Others indexes are even more narrow, measuring, for example, hospital price inflation overall or for different payers — the Medicare Hospital Producer Price Index (PPI), Medicaid Hospital PPI, Private Hospital PPI, Overall Hospital PPI, and Overall Hospital CPI. All five of these are shown in the author’s Figure 2, reproduced below. They exist for other services as well, not just hospital care.
Others indexes are even more narrow, measuring, for example, hospital price inflation overall or for different payers — the Medicare Hospital Producer Price Index (PPI), Medicaid Hospital PPI, Private Hospital PPI, Overall Hospital PPI, and Overall Hospital CPI. All five of these are shown in the author’s Figure 2, reproduced below. They exist for other services as well, not just hospital care.
PPI (overall and specific payers, disaggregated by service): A Laspeyres index of third-party payments appropriate for adjusting medical prices from specific payers for specific services.
CPI (overall and disaggregated by service): The same as the MCPI discussed above, but including components for different services. These are appropriate for adjusting for out-of-pocket spending.
There are large differences in these indexes, as shown in Figure 2, reflecting differences in price growth in hospital care versus overall medical care and/or differences in growth from different payers or out-of-pocket spending. If you’re analyzing hospital payments, it’s very important to match the index to the type of analysis you’re doing and questions you’re addressing.
The authors discuss many other nuances and issues, which are beyond the scope this post. They conclude with this advice:
To adjust health expenditures in terms of purchasing power, use the GDP implicit price deflator or overall PCE measure. The PCE measure is suitable for personal consumption. The GDP deflator is more appropriate for the societal perspective.
To adjust overall consumer out-of-pocket spending in terms of consumer purchasing power or out-of-pocket burden relative to income, the CPI-U can be used.
To convert average expenditures to care for a specific disease for price changes from 1 year to a different year, either the PHC deflator or the PCE health index can be used. Because of exclusions of some payers in its weights, the MCPI may not be appropriate to adjust all-payer expenditures or payments by employers, Medicaid, and Medicare Part A for medical inflation.
To convert average consumer out-of-pocket health care expenditures from 1 year to a different year, the MCPI can be used.
To adjust estimates of costs of inpatient services from different years, the PPI for inpatient services appears currently to be the best option.
I’m certain many published analyses do not follow this guidance, including my own. In some cases, it may matter. In offering clear guidance on how to use health care price indexes, Dunn, Grosse, and Zuvekas have provided a valuable service.
May 1, 2017
Healthcare Triage News: Data and Studies on Malpractice
Congressional Republicans have recently revived efforts to overhaul malpractice laws, including capping certain kinds of suits at $250,000. A perennial argument of supporters of such measures is that many claims are frivolous, clogging the court system and driving up health care costs for everyone. But does the evidence support this?
This episode was adapted from a column I wrote for the Upshot. Links to references and further reading can be found there.
Help me learn new skills in 2017 – Knitting!
This post is part of a series in which I’m dedicating two months to learning six new skills this year. The full schedule can be found here. This is month three/four. (tl;dr at the bottom of this post)
There were three lessons outside the skill I learned this month. First, it appears that very few men knit in public. I learned this because many women felt compelled to tell me this, in public. Second, I am apparently very comfortable in my own skin, because when people stared at me (they did) or took pictures of me (they did), I didn’t care at all. Neither did my wife, who apparently also likes that I don’t care. Third, knitters – while underground – are very, very friendly people and must talk to you about your knitting, their knitting, and anything else to do with knitting.
I started this month, as I almost always do, with a book. I tried Knitting Without Tears by Elizabeth Zimmerman. Huge mistake. This book, while pitched as a helpful starting place, was clearly written for Jedi Masters of knitting. I couldn’t do anything with it. The few diagrams were impossible to decipher, and I didn’t even get much of the text. I know a lot of knitters swear by it, but I was lost.
This was a problem, because I now had piles of cheap yarn, knitting needles of all sizes, and other various accouterments. And no knowledge at all. It was then I turned to YouTube.
I should have started there. YouTube is where it’s at for knitting. After watching various videos, I finally stumbled upon this one, by Hobby Lobby. It was basic enough to get me started.
First, you need to cast on. This is how you put your yarn on the needle and set the groundwork for the number of stitches in each row you’ll knit. Then, you learn to knit, using the other needle. The gist is that you push your needle through the cast on circle on the left, loop the thread around your right needle tip, and then drag it back through the circle on the left. Words fail. This is why you need a video.
With this knowledge, I went to work. I made a number of swatches over the next week. Here are a few:

I needed to learn to purl, which it the other main stitch in knitting. Also, the cast on technique from the Hobby Lobby video wasn’t really good enough. That’s when I found Chandi, from ExpressionFiberArts. Her intro video has more than 4.5 million views. I’m on YouTube, people; those are real numbers. Her videos are top notch for knitting. Trust me, I watched a ton of them. How do you bind off? Change colors? Slip a stitch? Almost any question you might have – she or someone else has a video.
Her cast on technique was much more solid. She got me most of the way to knitting, purling, and binding off. Plus, she was a little more entertaining than most. But my purls weren’t coming out right. So I made a trip to the yarn store.
This was hard. Really hard. First, I had to overcome my natural inclinations not to talk to others. Plus, I had to go talk about knitting. I didn’t want to.
Our local yarn store was just as you’d expect. Full of older women sitting around and talking while knitting. There was a dog who clearly was afraid of all people, especially my daughter and middle son – who wanted to pet the dog. The one proprietor did not want to talk to me, and she seemed suspicious of my intentions or desire to knit. I did not feel welcome. But, to her credit, she did correct my purl technique. I’d been wrapping the yarn around the right needle in the wrong direction. Very helpful. She also sold me some thick soft “yarn” that my daughter picked out for a scarf.
I figured this would be a good “first” project. I went wide – at least six inches – and chose a “seed” stitch. That’s just alternating knits and purls the whole way. It’s reversible, and I thought it would look nice. Off I went. The problem was, though, that I wasn’t yet good enough to recognize which were knits and which were purls. I had to rely on counting and memory where I was. Also, I wasn’t great yet at fixing my mistakes. I had many moments of panic. But I made progress:

It was a lot of repetition, but it was pretty rewarding to see it grow!
Plus, I was knitting! It’s hard to see from the pics, but this material was ridiculously light and soft. It was clearly artificial. But it’s what Sydney wanted, and I wanted her to use the scarf, so that’s what I used. When it was done, I was much, much prouder than I would have thought. But I could see it was uneven in places, and I had gotten a few purls and knits mixed up. The proprieter at the knitting store said I should block it.
Blocking is taking your finished product and soaking it in tepid water (and I added this soapy stuff the women recommended) for a period of time. Then you rinse and gently squeeze out the excess liquid. You roll the knitted project in a towel to dry it more. Then you stretch it out, or mush it together, to be the exact shape you desire at the end. Here’s the scarf blocked out:

It’s so even and straight! The crazy part is, when the scarf dried (about a day), IT WAS THAT SHAPE. Blocking is magic. Here it is in its natural setting:

That’s when I fell in love with knitting.
I got more ambitious. I wanted to make a hat. So I went back to the yarn store, this time with the whole family in tow. The proprietor was MUCH nicer this time. I think she realized I was in it for real. It didn’t hurt that I brought the scarf with me to show her. She took a lot of time, showed me some patterns and yarn, and I left the store with a bunch of stuff. I know I could have downloaded a pattern for free, but I wanted to support the local business. This time, my oldest (Jacob) would be the recipient of the hat. Noah (my middle child) was going to knit his own scarf. He’s usually the one who joins me on these learning experiences. He got into meditating, too.
A hat requires you to knit in the round. The first reason is that you need to make a circle, not a flat row. The second reason is that a hat’s diameter is usually longer than any straight needles could hold. You use round needles, which are shorter needles connected by a wire, so that each time you transfer a stitch from left to right, it starts to travel around the circle back to the left tip. You never knit from the right needle to left. I did this is 2×2 ribbing, which means that you do 2 knits, 2 purls, repeat – all the way around. Ribbing is good for hats because it stretches nicely. I was pretty proficient at this point, and made rapid progress:

I then switched yarn to blue, which went really well!

Those little green things you see are markers to tell me when I’ve hit the end of a “row” or need to remove a stitch to close the hat. You wind up knitting two stitches into one using various techniques to make things even. Eventually, there was too little hat to use the round needles anymore, so I had to switch to double pointed needles:

And then I finished. This hat rocked. First of all, I was good enough now to know how to recognize knits and purls, so that there were no mistakes. I was also good enough not to panic, like when the metal needle detached suddenly from the wire, and things almost fell apart near completion. I knew how to fix mistakes. Plus, I had gotten pretty even with my stitches, so that things looked nice! Here is the hat, blocked out and drying on a football:

And here’s a nicer look at it:

And here it is, in its natural setting:
I am RIDICULOUSLY proud of this hat. It’s a fricking hat! It looks professional. It’s basically made from one long string. And there is not one knot in this hat. All the ends are sewn in.
With little time left in the month, I had time for one more project. I wanted to make some socks for Aimee. But I made the mistake of not going to the yarn store last Saturday (lazy) and then found out on Sunday it’s closed. So I had to settle for another project I decided to make a small bag for Sydney, since this would also focus on some sewing skills.
I found a pattern in Stitch ‘n Bitch, the only other book I bought. This book I recommend as a nice companion. I got little out of it the first time I read it, but it was very useful as an aid when I wanted to go back and check things. Nice tips on fixing mistakes and such. A bunch of useful patterns. And when you want to a quick refresher on any topic, it’s in there. Buy it if you knit.
This bag involved two large swatches for the front and back, mostly in stockinette stitch with an inch or so of garter at the top. A long gussett in garter to attach to the front and back, and two straps in garter. Then I sewed it all together:

That’s after blocking on a shoebox lid. Note the detail where I attached the straps to the body. I think the inch of garter makes a nice contrast to the stockinette, too. Well done, Stitch ‘n Bitch! Here is the bag in its natural habitat:

I literally finished it yesterday. Deadlines matter.
I can make jokes about knitting all day, but I really loved this. My mother used to be a Home Economics teacher, and I can remember doing things like needlepoint as a kid. When Sydney got into Rainbow Loom a few years ago, I enjoyed doing that with her, too. But knitting rocks. It’s really versatile, you can make all kinds of things, and once you get going, you can really move. The hat took two weeks, even with lots of other things to do, and I bet I could do it more quickly next time. The bag took a week.
Plus, there’s something satisfying about making something with one string of yarn and two needles. It’s magic. I think I’ll likely start making things for people as gifts. I’ve already had requests for hats. And it’s something to do, when I’m sitting around watching TV or on a plane. I don’t care if people stare. Knitting won. Two months very well spent.
If you’re going to try, here are the tools I recommend. It’s anecdote, but it’s what I used:
Bamboo needles. You can get a whole set pretty cheap.
Rounded needles. I invested in a set I could expand later. I boucht the 5″ set, and a 16″ wire, but you can mix and match later
Knitting markers
A set of crochet needles for fixing problems
A set of sewing needles
A set of counters, which can also be used to identify left and right needles
A set of double pointed needles if you’re ambitious
Caps for your needles
On to drawing!
tl;dr: YouTube is the way to go to learn to knit. Videos like those from ExpressionFiberArts are invaluable. A nice resource to have is Stitch ‘n Bitch.
Aaron E. Carroll's Blog

- Aaron E. Carroll's profile
- 42 followers

