
Aaron E. Carroll's Blog, page 131
July 4, 2017
An Internet based weight loss program for postpartum women worked. Color me surprised.
From JAMA, “Effect of an Internet-Based Program on Weight Loss for Low-Income Postpartum Women“:
Importance Postpartum weight retention increases lifetime risk of obesity and related morbidity. Few effective interventions exist for multicultural, low-income women.
Objective To test whether an internet-based weight loss program in addition to the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC program) for low-income postpartum women could produce greater weight loss than the WIC program alone over 12 months.
Design, Setting, and Participants A 12-month, cluster randomized, assessor-blind, clinical trial enrolling 371 adult postpartum women at 12 clinics in WIC programs from the California central coast between July 2011 and May 2015 with data collection completed in May 2016.
Interventions Clinics were randomized to the WIC program (standard care group) or the WIC program plus a 12-month primarily internet-based weight loss program (intervention group), including a website with weekly lessons, web diary, instructional videos, computerized feedback, text messages, and monthly face-to-face groups at the WIC clinics.
Main Outcomes and Measures The primary outcome was weight change over 12 months, based on measurements at baseline, 6 months, and 12 months. Secondary outcomes included proportion returning to preconception weight and changes in physical activity and diet.
Pretty much all mothers gain weight during pregnancy. Keeping that extra weight after pregnancy, however, carries with it risks and issues. This study wanted to test an Internet-based program coupled with WIC for lower-income women. It was a year-long randomized controlled trial of 371 postpartum women at 12 clinics in California. Control clinics got standard WIC. Intervention clinics also got a website with weekly lessons, a diary, videos, automatic feedback, text messages, and monthly face-to-face meetings. The main outcome of interest was how much weight changed over a year.
I’d have bet money this wouldn’t work. It’s just some web based stuff and the usual outreach. Nothing significant. But the intervention group lost 3.2 kg over the year versus 0.9 kg in the control group. Almost a third of women in the intervention group returned to the preconception weight by a year versus less than 19% in the control group. There were no differences in their physical activity, calorie intake, incidence of injury, or low-milk supply.
So this pretty simple intervention worked, and it worked at a year. That’s better than a lot of diets, and this focused on women at the low end of the socio-economic spectrum. Seems like it’s at least worth more study and some consideration.



July 3, 2017
Some thoughts on health savings accounts and high deductible plans
Given the recent attacks by many Republicans on “high deductibles”, I thought that they might have abandoned their apparent love of consumer-directed health care. Perhaps not. Bret Stephens had a column in this weekend’s NYT discussing Health Savings Accounts as a panacea for the high cost of care in the US:
The only genuinely promising reform in the Republican health bills are proposals to nearly double contribution limits for heath savings accounts and allow them to be used to pay for premiums. Enrollment in tax-deductible, investable H.S.A.s has roughly doubled since Obamacare took effect, to about 20 million, because they help cover out-of-pocket costs for low-premium, high-deductible plans.
I have no problem with HSAs in theory. Truth be told, my family has an HSA plan from my employer. The difference is, my employer contributes the deductible to the HSA each year, so we’re only responsible for paying above that deductible to the maximum out-of-pocket payment.
Let’s also be clear: We can afford it. Our deductible is only $2500 for the family, the out of pocket max is only another $2500 above that, and my employer also generously contributes towards the premium cost. Oh, and I get a tax break on the remaining cost of the premiums, because employer-sponsored health insurance premiums are tax-deductible. If, by chance (and it rarely occurs cause I’m an expensive health cost guy), we manage to save money in the HSA from year to year, I get another tax break on the money made in the account.
So HSAs are great, for me, a reasonably wealthy guy who has generous employer-sponsored health insurance and a need for federal tax deductions. For most of the country – especially for the huge percentage who don’t pay federal income taxes and can’t use the deduction? Not so much.
HSAs don’t make sense for a huge part of the country, in fact. They only work if there’s money in the HSA. Where are poor people supposed to get the money to put in there? Even if you make the premiums for bronze plans free in BRCA, those plans come with $6000 deductibles. Unless the Republican bills change to fund the HSAs (which they show no intention of doing), no one just above the poverty line would be able to make use of the plans.
Of course, back when HSAs were first pushed, high deductibles meant something like $1000, not the massive ones we see today.
I understand the theory. A number of people believe (correctly) that people are less likely to spend their own money out of HSA accounts than other people’s money through first dollar insurance coverage. I also get that putting more decisions in consumers’ hands might lead to more parsimonious spending decisions. But HSAs today don’t accomplish that. They are of no use to the vast majority of people on the exchanges without significant cost-sharing reductions.
When people talk about HSAs today, especially in conjunction with the exchanges, they’re telling poorer people to put money they don’t have into accounts that don’t benefit them from a tax perspective, to pay for deductibles they can’t hope to afford.
Any serious talk of consumer-directed health care for the poorer half of America has to revolve around massively funding the HSAs, at least to the point of covering deductibles . It has to incentivize users with carrots that actually mean something to them. It also has to grapple with the fact that as long as there’s a huge gap between what they have in the HSA and what they might have to spend out-of pocket, it doesn’t matter how low you make the premium. People won’t buy plans. Don’t take my word for it. The CBO said the same.
One more thing. If you truly believe that HSAs and consumer-directed health care will slow health care spending in America, you have to grapple with this:
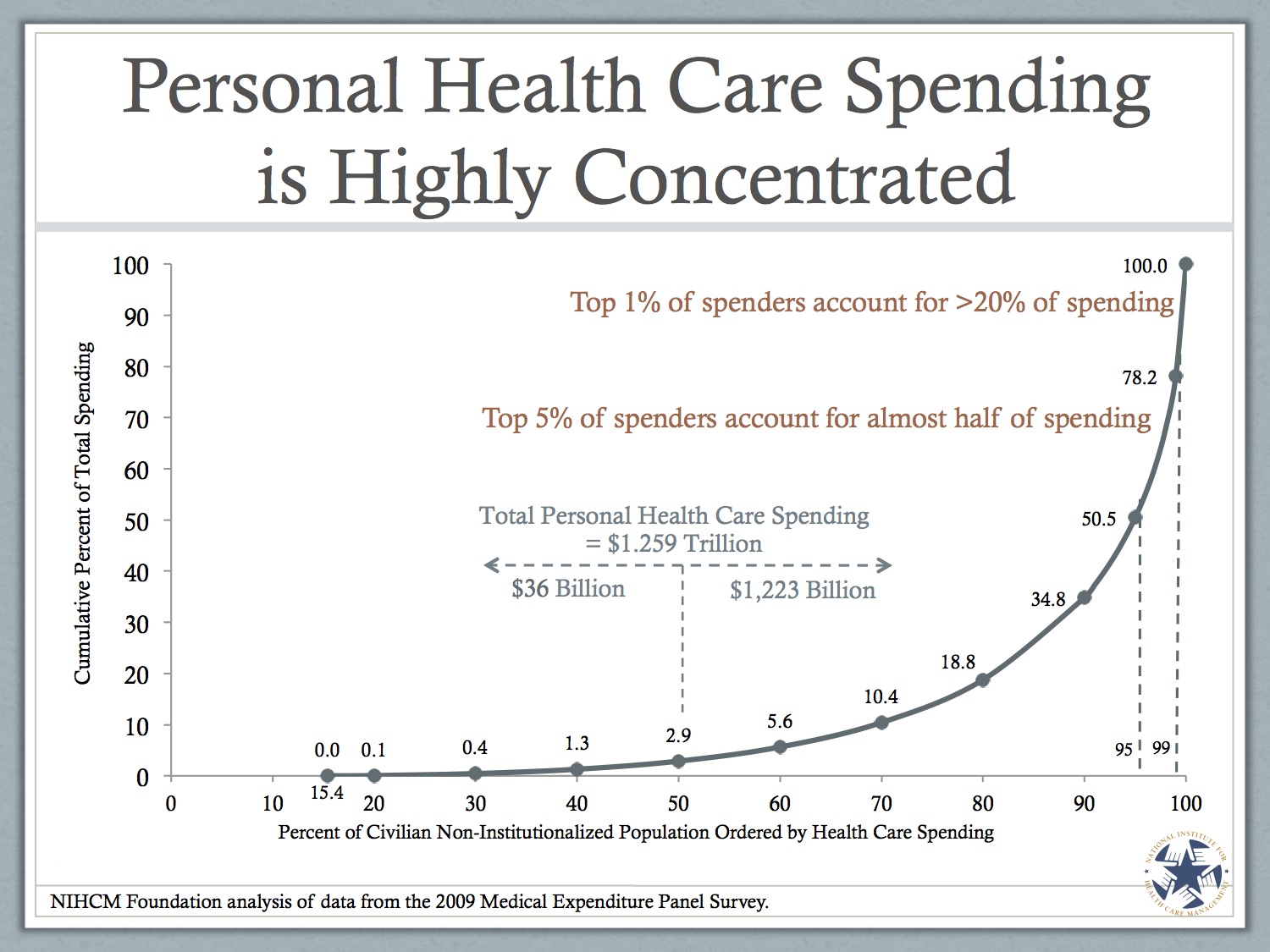
These slides are a couple of years old, so jack up the numbers in your head. In 2009, the top 10% of health care spenders in the US accounted for about 65% of all health care spending. They spent, on average, more than $26,000 each year on health care. I’m sure it’s way higher how. The point is this – health care spending in the US is concentrated among a smaller number of very expensive people. They will ALL, and I mean ALL, blow past the out-of-pocket maximum in the beginning of each year. HSAs are useless for them. Many of them are on Medicare, so the whole HSA craze doesn’t apply anyway.
HSAs and consumer-directed healthcare may help to reduce individual spending at the margins if we actually made them attractive to the poor. Even then, though, it’s hard to see how them nudge overall health care spending since the bulk of people who cost us the most won’t find any use for them at all.
More reading on this subject here and here and here and here.
July 1, 2017
You Say You Want a Single-Payer System: The Canada Health Act
Senator Warren says that
President Obama tried to move us forward with health-care coverage by using a conservative model that came from one of the conservative think tanks that had been advanced by a Republican governor in Massachusetts. Now it’s time for the next step. And the next step is single payer.
Representative Conyers has introduced a Medicare for All bill into the House. Senator Sanders is drafting one for the Senate. For Canada Day/Fête du Canada, here’s a brief introduction to the key legislation underlying Canada’s health care system, the Canada Health Act.
The first thing to know is that Canada does not have a single-payer system. There is a single-payer insurer in each province and territory. The Canadian federal government makes a block grant contribution to each province amounting to about 20% of the province’s health care spending. The Canada Health Act lays out requirements for those provincial single-payers to get that cash:
The purpose of this Act is to establish criteria and conditions in respect of insured health services and extended health care services provided under provincial law that must be met before a full cash contribution may be made… the health care insurance plan of the province must, throughout the fiscal year, satisfy the criteria… respecting the following matters:
(a) public administration;
(b) comprehensiveness;
(c) universality;
(d) portability; and
(e) accessibility.
These five points are what single-payer is supposed to accomplish. These goals are what matters, single-payer is a means to these goals, not an end in itself. Here’s what they mean:
Public administration means that the insurer must be non-profit, responsible to the provincial government, and meet requirements for transparency.
Comprehensiveness means that
the health care insurance plan of a province must insure all insured health services provided by hospitals, medical practitioners or dentists, and where the law of the province so permits, similar or additional services rendered by other health care practitioners.
Whether Canadian care is truly comprehensive depends on how “similar or additional services rendered by other health care practitioners” is understood. It hasn’t been interpreted as including outpatient services provided by psychologists or social workers, meaning that a lot of mental health care isn’t covered. Moreover, covering services does not mean covering drugs unless they are delivered in hospitals. Whether drug costs should be covered is a major health policy dispute in Canada.
Universality means that
the health care insurance plan of a province must entitle one hundred per cent of the insured persons of the province to the insured health services provided for by the plan on uniform terms and conditions.
On this one, Canada delivers.
Portability more or less means that my Ontario Health Insurance Plan card will be accepted when I’m in any other province, and vice-versa.
Accessibility means that the insurers must give reasonable compensation to hospitals and providers and
must provide for insured health services on… a basis that does not impede or preclude, either directly or indirectly whether by charges made to insured persons or otherwise, reasonable access to those services by insured persons.
You can cover everyone universally, but that doesn’t mean that everyone can access care. If you hadn’t heard, Canada is a big place. Providing care in remote areas is an enormous challenge and there are important disparities in the abilities of different ethnic and linguistic groups to access care.
These are the goals of the Canadian health care system. They are, in my opinion, the right ones. Universality is just the first step: achieiving true comprehensiveness and universality is an ongoing struggle.
So, Happy Canada Day / Joyeux Fête du Canada! The Confederation is 150 years today.
June 30, 2017
Will we ever see Medicare Advantage encounter data?
Charles Ornstein reports on the latest chapter in research access to Medicare Advantage encounter data:
The government has collected [Medicare Advantage] data on patients’ diagnoses and the services they receive since 2012 and began using it last year to help calculate payments to private insurers, which run the Medicare Advantage plans. But it has never made that data public.
Officials at the Centers for Medicare and Medicaid Services have been validating the accuracy of the data and, in recent months, were preparing to release it to researchers. Medicare already shares data on the 38 million patients in the traditional Medicare program, which the government runs. […]
The grand unveiling of the new data was scheduled to take place at the annual research meeting of AcademyHealth, a festival of health wonkery, which just concluded in New Orleans.
But at the last minute, the session was canceled.
Go read the whole thing. I am quoted.
Help me learn new skills in 2017 – Drawing!
This post is part of a series in which I’m dedicating two months to learning six new skills this year. The full schedule can be found here. This is month five/six. (tl;dr at the bottom of this post)
Let’s start with the good news: You can absolutely learn to draw. The bad news is that I’m not sure I enjoy it enough to make it a regular part of my life. That’s not to say that I didn’t find the last two months to be rewarding; I certainly did. I think that drawing, and drawing well, just take too much time and undivided attention. It will be hard to keep it up.
This post will be chock-full-of-pictures, because it was “drawing”. If that’s not your thing, feel free to skip to the tl;dr below.
Most of my efforts were focused on one source, because it was the overwhelming advice of nearly all of you who responded. I read Drawing on the Right Side of the Brain, by Betty Edwards. I also bought the workbook, which is really all you need. If I were to do this again, I’d just go with that.
Ms. Edwards breaks down drawing into five sections. These include:
The Perception of Edges
The Perception of Spaces
The Perception of Relationships
The Perception of Light and Shadows
The Perception of the Gestalt
There’s genius there. The first section starts by making you commit to some drawings, so that you can see how much you’ve improved later. I’m embarassed by mine, but I’ll post them nonetheless. Then, she gets into edges. A lot of the exercises are meant to train your brain to stop worrying about what you’re drawing and just focus on what shapes you see. One of her tricks is to get you to draw things upside down. For instance, I couldn’t draw a horse to save my life, but when I copied this Schiele drawing upside-down, I had much less trouble:

When you’re just drawing the edges without thinking about what you’re drawing, you do much better. One of the very early exercises (May 5th) was drawing a hand. I drew another on May 17th, holding a small plastic fork. In the second, I focused on small spaces, the edges between things, and not the hand. You also learn to look at things with one eye closed, to see them two dimensionally. The difference is stunning:


The second section gets into negative spaces. This is where you focus on the stuff around what you’re drawing as much as you focus on subject itself. I can’t stress how important this is. For instance, here’s a picture of a kitchen tool I drew pretty much entirely by shading in the area that wasn’t the tool:

In another exercise, I copied Vincent Van Gogh’s Man, Sitting, Reading a Book with special emphasis on the negative spaces within and without the figure. This was on June 7th. I was starting to get proud of myself:

Learning about relationships meant developing skills to sight angles and proportions. You know when you see an artist hold up their pencil or brush at arms length and close an eye? That’s sighting. It makes a difference. On May 5th, I drew the corner of a hotel room. On June 7th, with what I’d learned, I drew our dining room through our kitchen. Again – progress.


It also means learning to sight in figure drawing. Here’s a drawing I did copying Sargent’s Standing Male Nude Seen from Behind:

Here’s Sargent’s Madame X, which lets you understad the proportions of a face. For instance, the distance from the eye to the bottom of the head is also the distance from the eye to the top of the head. It’s also the distance from the back of the eye to the back of the ear. There are a bunch of proportions to learn, that are mostly the same in all people:

This section ended with a side portrait, which I did of myself. Aimee tells me it looks more like my brother than me, but I was pretty proud of it:
 The final section was about light and shading. It ended with a full on portrait. That’s where I decided to stop, because the final section (on Gestalt) didn’t seem to add much more. The full portrait was also one of the starting exercises you did, so you could see your progress. First up is my self-portrait from May 5th, followed by my same on June 29th.
The final section was about light and shading. It ended with a full on portrait. That’s where I decided to stop, because the final section (on Gestalt) didn’t seem to add much more. The full portrait was also one of the starting exercises you did, so you could see your progress. First up is my self-portrait from May 5th, followed by my same on June 29th.


A number of my co-workers, as well as my wife, were quick to tell me that I’m “thinner” than I drew myself. I would reply that this is a portrait, not a photograph, and it’s not going to be perfect. Regardless, there’s no question that the skills of the person who drew the first picture and the skills of the person who drew the second picture are not equivalent. All credit goes to Ms. Edwards.
I’m not going to try and argue that now I’m super talented at drawing. I will never say again, though, that “I can’t draw”. This exercise was a complete success in that respect. I feel like I know what I’m doing, and I don’t doubt that if I continued to work at this, I’d improve. I also learned some basic tips I’ll pass on:
The eraser is your friend. No one gets things right the first time.
Start with light lines. Darken them as you go and are closer to done.
A good drawing set is key. I got one for less than $6 on Amazon.
Shade. Use a paper towel to blur lines and help get shadows right. It matters.
There’s a reason artists do lots of practice drawings before the final project. They learn along the way, how to lighten and darken, how to color, how edges fit together. You can, too.
Unlike knitting, I found that I had to give all my attention to drawing. I can’t do it while I talk to people or watch TV. It also takes a lot of time. I’m not sure it’s something I want to keep up. Knitting, on the other hand, I have. I’m working on a pair of socks for Aimee. I’m also meditating again. I think drawing, while a useful learning experience, is something I will let go for a while.
Hebrew is next. Deep breath. I’m not a language guy.
tl;dr: You can TOTALLY learn to draw. It’s not an innate skill. The only thing you need is a drawing set and the Drawing on the Right Side of the Brain Workbook.
June 29, 2017
The Republicans’ Uncertainty Strategy
Together with Craig Garthwaite, a professor at Northwestern, I’ve got an op-ed in the New York Times on the consequences of the Republicans’ strategy to sabotage the Affordable Care Act.
The health care industry consists of a dense network of public-private partnerships. Even programs widely viewed as “government” insurance, like Medicare and Medicaid, depend on private hospitals, doctors and insurers.
Such arrangements can work only if private firms trust that the United States will be a reliable partner. Historically, this hasn’t been a problem.
That appears to be changing. A decline in trust has already caused health insurers to rethink their relationships with their increasingly erratic federal partner. They’re demanding higher premiums to account for the greater risk. Blue Cross Blue Shield in North Carolina, for example, has said that its planned rate increase of 23 percent next year would be only 9 percent if it had more certainty from the federal government.
Many other insurers have abandoned these partnerships altogether. According to Health Secretary Tom Price, 49 counties won’t have a single insurer on the exchanges in 2018.
Here’s the kicker:
Republicans appear not to have reckoned with the broader consequences of their uncertainty strategy. For example, Paul Ryan, the House speaker, wants to convert Medicare into a voucher program in which the elderly will shop for private plans. How will that work if insurers, burned by the Obamacare experience, are unwilling partners?
This is perhaps the greatest irony of the Republican actions. Republicans (including one of us) have long believed in the benefits of even greater privatization of government services. But how can any company in any sector trust the United States after seeing health insurers treated so shabbily?
June 28, 2017
Medicaid, a “broken program that harms its beneficiaries”
I asked on Twitter for policymakers’ expressions of harm caused by Medicaid.
Seen a *policymaker* justify BCRA Medicaid changes because "Medicaid causes harm"? Send me the link. cc @aaronecarroll
— Austin Frakt (@afrakt) June 28, 2017
By email, Andrew Goodman-Bacon came through in a huge way. The bullets below are a lightly edited version of what he sent me, shared with his permission. (For the record, Medicaid does not cause harm. More about that soon.)
The Sommers/Epstein paper surveyed governors and found that five of those who opposed expansion felt that Medicaid was a “broken program that harms its beneficiaries.”
Senator Ted Cruz has said that Medicaid hurts health care access
In one of Tom Price’s recent testimonies he said ,“Medicaid is a program that has, by and large, decreased people’s ability to access care.”
Speaker Paul Ryan comes close on pg 24 of “A Better Way
A Healthy Indiana report (notably produced by the Pence administration) cites Roy and LaPar, but doesn’t go all in on the “harms” claim
Here is the American Action Forum saying “harm”
See also, this brief from a policy shop in MI, this brief from a policy shop in NC, and this brief from a policy shop in PA
Here is ALEC citing that study, although not going so far as to say patients will be “harmed”
To these, I will add this quote of Representative Bill Cassidy (via Aaron) and this op-ed by Seema Verma (via Adrianna). Note: I have not looked through everything in the above list. If you find errors or have more contributions, let me know.
Can you smell the freedom?
The central theme of the Republican campaign to repeal the Affordable Care Act has been freedom: freedom from Obamacare’s onerous regulations, freedom from overpriced insurance and most of all, freedom from the tyrannical individual mandate.
The Senate has now released its long-awaited alternative to Obama-era health reform. Although the Better Care Reconciliation Act is embattled, there’s still a decent chance that the Senate will pass it. If it does, the bill is likely to become law.
So it’s reasonable to ask: How does the Senate bill stack up when it comes to freedom?
So begins an op-ed that I just published in the L.A. Times. The answer is “not well.”
Because the truth is the bill has nothing to do with freedom. It’s a vehicle for cutting Obamacare taxes, especially on the wealthy. Over the next decade, individuals who earn more than $200,000 and families that earn more than $250,000, will get a tax cut worth$230 billion. The bill also repeals taxes on health insurers, drug companies and medical device manufacturers; in total, the tax cuts amount to more than $750 billion over 10 years.
The need to pay for the tax cuts explains why the bill’s coverage numbers are so dismal. The more you reduce federal support for health insurance, the more people will lose coverage. It’s really very simple. Obamacare taxed the rich to pay for insurance for the poor; the Senate bill zeroes out those taxes and thus eliminates the coverage gains.
Now that the Senate has shown its cards, it’s become apparent just how empty the Republican rhetoric was all along. Trumpcare may liberate wealthy people’s money from the taxman, but that’s about the only freedom it delivers.
Read the whole thing here!
The ABCs and Ds of Whether to Get Prostate Cancer Screening
The following originally appeared on The Upshot (copyright 2017, The New York Times Company).
It can be hard for physicians to follow current thinking of experts on medical care. It must be exponentially harder for the public to make sense of it. Recently, the United States Preventive Services Task Force changed its recommendation on prostate cancer screening from a D (that is, don’t do it) to a C (discuss it with your doctor).
Although there seemed to be a lot of coverage of this announcement in the news media, and a fair amount of excitement, there are two things men should know. First, it’s a good thing that recommendations change over time; second, this change isn’t as big a deal as you might think.
The task force is made up of volunteers who are experts in primary care and preventive medicine. They are charged with evaluating the benefits and harms of preventive services (like prostate cancer screenings) to determine whether they should be widely performed. An from the panel can be interpreted as an endorsement that everyone get a service because there’s a high certainty of a substantial benefit. A “B” recommendation is similar, but means that there’s only a high certainty of a moderate net benefit.
A “D” recommendation advises patients not to get a service because there’s a moderate certainty of no net benefits, or because the harms from a service outweigh the benefits.
Five years ago, the task force gave prostate cancer screening a D recommendation because there are real harms from over-diagnosis of the disease. Over-diagnosis leads to unnecessary treatments, and a newly discovered cancer could lead to no symptoms or harm over the patient’s lifetime. The treatments for prostate cancer, including radiation and prostatectomy, have high levels of adverse events. About 75 percent of all the men treated will have impotence, incontinence or both.
Further, at the time of the 2012 statement, there appeared to be little evidence that screening with a prostate-specific antigen blood test (PSA) reduced prostate cancer mortality. With no clear benefit, and significant harms, a D recommendation seemed appropriate.
Many disagreed. They argued that there were benefits to screening, and that those would be shown through better research. They were, to some extent, correct. In 2014, researchers for the largest randomized controlled trial to date published an update of an earlier study, and it showed that offering men screening reduced their relative risk of dying of prostate cancer over 13 years by 21 percent. Another study published in late 2012 showed that offering screening reduced the relative risk of metastatic disease by 30 percent.
This meant that it was no longer true that there was no evidence of net benefits for screening, and a “D” no longer applied. Therefore, the task force altered its recommendation to a “C,” which means there’s moderate certainty that the overall benefit is small. That signals to patients and physicians that they should make an individual decision based on patient preferences and circumstances.
It’s important to note that these changes apply only to men 55 to 69. For men 70 and older, the harms outweigh the benefits, and the screening recommendation remains a “D.”
I’m sure the nuances of A, B, C and D recommendations can be confusing to the public. They can also make it seem like experts are constantly changing their minds. But this is how we want our experts to react: When new evidence is found, it should be added to older evidence to change our thinking when appropriate.
On the other hand, caution is still warranted when thinking about whether a man should be screened for prostate cancer. Although there is now evidence of a benefit, and its relative importance seems impressive, its absolute effects are not as persuasive.
According to these studies, a 55-year-old man has about a 0.6 percent chance of dying of prostate cancer over the next 10 to 15 years. If he is screened, that chance goes down to 0.5 percent. That’s how you get almost a 20 percent relative reduction, but an absolute reduction of only 0.1 percentage points.
Further, if a man is screened, the studies show that there’s about a 25 percent chance he will have a positive PSA test at some point. Of all men screened, about 10 percent will be found to have prostate cancer, and about 8 percent will be treated with surgery or radiation.
So out of 1,000 men screened, 80 will eventually have surgery or radiation. Three will avoid the spread of cancer to other organs. One or two will avoid death from prostate cancer. Sixty will have urinary incontinence and/or impotence. Many men will probably still think the risks outweigh the benefits.
One of the biggest concerns with screening is that too many men are treated for slow-moving prostate cancers that might never really pose a risk to their health. A new approach, known as active surveillance, offers an alternative. Instead of receiving immediate surgery or radiation, men with lower-risk cancer are watched more closely and receive more frequent PSA tests and biopsies. If the cancer progresses, they receive interventions. About 40 percent of men with lower-risk disease were treated this way from 2010 to 2013, up from 10 percent of men from 2005 to 2009.
The goal of health care, as always, should be to maximize the benefits of care while minimizing the harms. With this most recent recommendation, the preventive services task force recognizes that PSA screening now has more evidence to support its upside. There’s still a large downside, though, and the ways in which we respond to positive screens should try to minimize interventions.
June 27, 2017
Healthcare Triage: Deprescribing – Sometimes Taking Fewer Medication is Better
Prescription drugs are pretty awesome. They improve lives all the time. But it is possible to take too many. Over time, as patients are prescribed more an more ongoing medications, it’s a good idea to sometimes step back, evaluate, and think about whether people can drop some of their long-term meds. Between interactions and long term side effects, sometimes less is more when it comes to medicating patients.
This episode was adapted from a column Austin wrote for the Upshot. Links to sources and further reading can be found there.
Aaron E. Carroll's Blog

- Aaron E. Carroll's profile
- 42 followers

