
Michelle Stiles's Blog, page 5
February 9, 2015
Want to Know Which Hospitals Have Higher Than Average Knee Replacement Complication Rates?
No one wants to be in the small percentage of people who have knee replacement complications after surgery. So anything that helps protect consumers is a good thing-right?
Recently, CMS (Centers for Medicare and Medicaid Services) released data from 2009 through 2012 on readmissions within 30 days following knee replacement surgeries as well as knee replacement complication rates for all of the following adverse events by hospital:
Acute myocardial infarction
Pneumonia
Sepsis
Surgical site bleeding
Pulmonary embolism
Mechanical complication
Joint infection
Death
The raw data is available here in a very unhelpful format. Techie Alert: Any database people out there who could pull the raw data on just knee replacements?
CMS recently released a table, based on this data, of the 97 best and 95 worst hospitals as compared to the national averages for complications and readmissions.
I’ve color coded this chart and you’ll be able to download it in a PDF format for easy viewing and printing at the bottom of this blog post.
However, being mindful of the quote
“Lies, damned lies and statistics”
Let’s try to put this data in perspective by looking at real numbers for national complication rates as opposed to just relationship data.
From the AAOS website (American Academy of Orthopedic Surgeons):
“The complication rate following total knee replacement is low. Serious complications, such as a knee joint infection, occur in fewer than 2% of patients. Major medical complications such as heart attack or stroke occur even less frequently. Chronic illnesses may increase the potential for complications. Although uncommon, when these complications occur, they can prolong or limit full recovery.”
A more detailed look at complication rates complied from government and clinical sources and presented by healthline is available below.
Overall rates of complications were 6.1% during a hospital stay and 7.5% within 90 days of surgery based on 1.82 million patient records. Data breakdown into smaller categories reveals the following: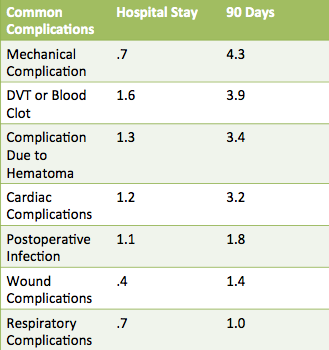
Generally speaking, 90 days post-surgery, you will have a less than 2% chance of having a knee infection, less than 4% chance of blood clots and a 4.3% chance of mechanical complications. Very good odds really.
Now that we know some of the real numbers, lets go back to the CMS story.
CMS is getting ready to launch on initiative in the fall of 2014 that will penalize hospitals 3% percent of their Medicare reimbursement rates for each patient stay for those hospitals that do not meet acceptable benchmarks.
CMS is already penalizing 2,225 hospital for unacceptable rebound rates for pneumonia, heart attacks and heart failure. Joint replacement data will be factored into the decisions to financially penalize institutions soon.
If the government is in control I can’t think of anything that will go wrong, can you?.
Of course, they wouldn’t politicize their penalties for hospitals that don’t play ball according to their dictates. Now that…. would NEVER happen. No worries there.
Beside the fact that there is definitely something creepy about a government “penalty program”, I can think of a number of ways this can go wrong.
What about unintended consequences like…
Institutions refusing to perform surgery on high risk patients to pad their stats and ensure full reimbursement.
How about the best hospitals denying replacements to diabetics, the obese and those with heart issues -groups that are most likely to have complications.
Or even refusing to do bilateral knee replacements which tend to have greater complication rates.
In fact, I already know that this type of thing is happening at the home health level. As they impose these penalties corporations are not dumb.They avoid or dump the sickest people when profits and reimbursements are at stake.
Additionally it is not always the institution’s fault that things go wrong. Human beings don’t always do what you tell them to do and penalizing institutions because patients are non-compliant is about as intelligent as penalizing teachers for students not learning.
I know, I know now I am getting into much deeper waters. The fact is you need to use your brain.
I am passing on this chart about “the best and worse” hospitals because I want you to have every available tool to assist in making quality decisions, but don’t use it blindly.
Remember the following caveats:
This data was compiled for years 2009-2012. Many of the worst hospitals have already made improvements in advance of penalties and conversely other hospitals rated superior may have had changes that caused their numbers to fall.
Some hospitals that are excellent may have been consistently treating a sicker or less compliant clientele although CMS purports to account for this with statistics
Personally, if you really trust your doctor and know what to look for in picking a top quality knee replacement surgeon, I wouldn’t let the hospital rating deter you. (I would definitely discuss it with the surgeon and he may be able to give you more insights)
Perfection is not available in medicine. What are the human costs, time costs and unintended consequences of trying to drive rates of infection down to say .5%? As laudable a goal as that first appears to be, massive government intervention and super-quantification of medicine are not benign forces.
Remember ratings are compared to national averages. Here is the coding for the chart.
—— =results met national averages
“better”= results were better than national averages
“worse”= results were worse than national averages


Want To Avoid a Knee Replacement?

Here's one way to ensure having the best chance to avoid the bludgeoning numbers of folks having to a knee replacement.
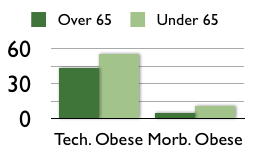
Researchers at the University of Massachusetts Medical School tracked 9,000 patients in a first-of-its-kind database for knee and hip replacements and patient reported outcomes. They concluded that the increasing rate of knee replacements currently being performed could be linked to increasing obesity rates among younger patients.
Researchers stated that "55 percent of patients under age 65 were considered technically obese compared to 43 percent age 65 and older. Even more striking was that twice as many younger patients were in the morbidly obese category (body mass index greater than 40) – 11 percent of those under age 65 versus 5 percent age 65 and older. The younger patients also had higher rates of smoking and lower mental health scores." Read more about original study...
But of course we intuitively knew this already, didn't we? Carrying around more weight will wear out your joints faster, It is very simple.
Something you might not know is that body weight forces are multiplied by different types of activity. A Journal of Bio-mechcanics study (J Biomech. 2010 Aug 10;43(11):2164-73) determined peak forces as a percent of body weight for the following activities.
Peak Forces as a Percentage of Body Weight
Stair descending (346% BW)
Stair ascending (316% BW)
Level walking (261% BW)
One legged stance (259% BW)
Knee bending (253% BW)
Standing up (246% BW)
Sitting down (225% BW)
Two legged stance (107% BW)
See how high one legged standing is? All your body weight is being carried on one leg driving up the forces that your knee is experiencing. It makes sense then that descending stairs and ascending stairs are rated high as well because lowering on one leg and raising up on one leg are just more difficult versions of a one legged stance. This is by the way, one of the reasons why stair training is more difficult to master after someone gets their knee replaced. But I digress...
Negative Effects of Obesity
It makes sense that obesity at a younger age will predispose you to greater damage because you are generally still very active. You will be using up what is suppose to be a lifelong supply of cartilage. If on the other hand, you gained some extra pounds late in life after you had slowed down, you would not be in the position to do as much damage to yourself.
One the positive side, research from 2005, (Arthritis Rheum. 2005;52:2026-2032) found that for each pound of weight lost there was a fourfold reduction in the load exerted on the knee per step during daily activities. Just one pound of weight loss will help protect your knees into old age.
The four take home points to avoid a knee replacement are:
* Some activities are more demanding on your knees and wear them out faster
* Being overweight is more taxing on your knee no matter what activities you choose.
* Being overweight at a younger age is more damaging to your knees
* Just one pound of weight loss can ensure a fourfold reduction in knee forces.
So the moral of the story is...
Get started taking the weight off now or you may just have to get in line to have your knee replaced.
A Free Knee Replacement-For Christmas?

A Free Knee Replacement- For Christmas?
That is exactly what santa brought this year for a few fortunate people across the United States who were in need. Well not santa exactly.and maybe they won't exactly be dancing around the Christmas tree this year but they received a big present from a great organization of cool people.
Operation Walk USA is a non-profit organization that donates total knee and total hip surgeries to candidates that do not qualify for government assistance programs and cannot afford to pay for them on their own. They perform the surgeries once a year in early December.
As you can see from the story below, they just completed the 2013 event which occurs in various locations around the country. A list of the locations used this year can be found at the bottom of this blog. Remember that next year, more sites could be added or an existing site could discontinue participation but at least it is a start. Most of the time you must live in the surrounding area to qualify. Bookmark the following page and start looking into it if you or someone you know may be in need of the generosity provided by these surgeons and hospitals. http://www.opwalkusa.com/
On the other hand, maybe you are in a position to benefit others by donating to this group for next years project, especially if you have experienced the transforming effect of having had a knee replacement yourself.
Check out the story in Kansas City and see for yourself...
Donated hip and knee replacements give patients 'back their life' - Kansas City Star
http://news.google.com Sat, 07 Dec 2013 21:27:00 GMT
Donated hip and knee replacements give patients 'back their life' Kansas City Star Surgeons from the Kansas City Bone & Joint Clinic and Carondolet Orthopedic Surgeons, in partnership with the hospital, did six no-cost knee- and hip-replacement surgeries ...
Anchorage, AK
Little Rock, AR
Prescott AZ
Tucson AZ
Colton, CA
Los Angeles, CA
Newport Beach, CA
Orange, CA
Pasadena,CA
San Diego, CA
San Ramon,CA
Denver, CO
Grand Junction,CO
Parker,CO
Newark, DE
Jacksonville FL
Mainland,FL
Stockbridge,GA
Chicago, IL
Skokie, IL
Springfield, IL
Winfield, IL
Overland Park KS
Danville, KY
Boston MA
Bethesda, MD
Hagerstown, MD
Petoskey, MI
Saginaw, MI
Traverse City, MI
Minneapolis, MN
Flowood, MS
Billings, MT
Fayetteville, NC
Morehead City, NJ
Mount Airy, NC
Omaha, NE
Basking Ridge, NJ
Hackensack, NJ
Long Branch, NJ
Albuquerque, NM
SAnte Fe NM
Buffalo, NY
NY, NY
Cincinnati, OH
New Albany, OH
Upper Arlington, OH
Tulsa, OK
Butler,PA
Philadelphia, PA
Pittsburgh, PA
Wakefield, RI
North Charleston, SC
Dallas TX
Flower Mound, TX
San Antonio, TX
Alexandria, VA
Arlington, VA
South Burlington, VT
Seattle, WA
Spokane, WA
Tacoma, WA
Franklin, WI
Huntington, WV
Morgantown, WV
Steering Clear of Marketing Hype for Knee Replacement Implants
Think you should be making the decision about the best knee replacement implants? Think again!
Potential knee replacement patients are being bombarded with tons of marketing messages regarding the desirability of various implants. The biggest problem with targeting a group with marketing messages is that it gives that group the impression that they should be able to make a decision regarding the value of the product.
What is the effect of marketing cereal to younger children? They naturally believe because the messages are targeted toward them that they should be able to make the decision about the brand of cereal Mom buys. In reality, they have no real knowledge upon which to base that decision. Such is the pernicious effect of targeting groups of uninformed people with marketing messages.
In using the term uninformed, I mean no disrespect to potential patients. In fact they could be very well read on the pros and cons according to the available material at hand. But we all know that marketing information may or may not be valid and that FDA clearance is no absolute surety of safety, just ask the people that were harmed as a result of using one of the many medical products and drugs recalled in the last 10 years. You’ve seen all those lawyer ads.
The purpose of this post is to permanently disabuse you of the notion that you can decide which implant type you want your surgeon to use. The means to accomplish this is twofold. I am embedding a video which shows two surgeons using two different types of knee replacement implants; the rotating hinge and the MRI-assisted.
It is a bit dated but valuable none the less to hear the discussion about rationale going on among surgeons for various things they do or do not do.
Because the video is 1 hour and 20 minutes long, and because I understand that watching a knee replacement surgery live on video is just not what some potential patients should be doing prior to the undergoing the operation-I’ve provided the transcript of the video for you to download and read instead.
 Knee Replacement Surgery-Two Techniques
Knee Replacement Surgery-Two TechniquesTwo surgeons demonstrate different techniques for knee replacement surgery and field questions on topics of interest for those considering a knee replacement in the future
The questions that they answer during the surgery are wide ranging and valuable. I have bolded and highlighted those questions so that you can get good information quickly. Consider it my gift to you in the new year.
Remember when all is said and done… The bottom line is… find a surgeon who is highly skilled at his craft, who you trust and let him make the decisions about the implant type.
The Mental Aspect of Total Knee Replacement Recovery
Common sense says, “Of course it does!” Here is an update on the research in this area.
In the past, studies have shown that anxiety and depression preoperatively influence the outcomes of knee replacement recovery. A recent study looked at ‘catastrophizing,’ perceived injustice, fear of movement, and recovery expectancies and total knee replacement outcomes.
Dr. Victoria Brander, a physical medicine and rehabilitation specialist at Northwestern Orthopaedic Institute in Chicago, summarized the results of the recent study as follows:
All of these psychological factors point to the fact that patients who perceive themselves as helpless, those who are afraid, those who feel loss of control, have a more difficult time. The contrary is also true – patients who exhibit high levels of ‘self-efficacy’ (that is, patients who have a high degree of confidence in their own ability to achieve a goal) appear to do best after knee replacement.
See the original study here: The role of perceived injustice in the prediction of pain and function after total knee arthroplasty
See Reuters Report Here
After years of treating patients in the field, I stumbled upon the fact that patients did better when they had control of the outcomes. I started teaching them a system where they could track daily progress by converting degrees to inches. I started leaving tools in the home. These tools allowed the patient to leverage their stretch without a physical therapist being present. This tool, called a FLEX Bar is now available on Amazon. In short I was created a system where the patient was central and only needed me as a coach. It gave my patients an overwhelming sense of confidence and control.
It might take someone a few visits to grasp the concepts but once they did, I could see the change in confidence instantly. Instead of being stowaways on a ship headed into the unknown, they become captains of the ship. It was no longer about me the therapist and what I could or could not do for them.
If you want to have a plan going into surgery instead of hoping and trusting an increasingly corrupt corporate medical establishment …grab my book. You will get all the insider knowledge you need and a proven system to help you confidently achieve a speedy and successful knee replacement recovery .
Remember, start with a great surgeon. If you don’t no amount of total knee replacement recovery will fix poor alignment. But on the other hand a patient can have a great surgeon and still have a very hard time with recovery because they are doing things all wrong.
It is not brain surgery, if you know the basic principles. Anyone can succeed.
The post The Mental Aspect of Total Knee Replacement Recovery appeared first on .
Find the Best Hospitals for Knee Replacement Surgery In Less Than 1 Minute
Simply knowing that high volume hospitals have lower complication rates is a critical piece of information, if you are thinking about getting a knee replacement. No one wants complications. They jeopardize safety, cost money and waste a ton of time.
Finding out the actual volumes of knee replacement surgeries each hospital is doing without wasting a morning on the phone, listening to phone trees and risking profound aggravation, is another thing.
The wait is over. Now you can easily look up the hospitals located around your area code and get the results in under 1 minute. Fantastic.
The nerd wallet is a website that has just launched a new service called the Best Hospitals Tool.
Go directly to the knee replacement page and enter your location and click on the “go” button.
Nerdwallet pre fills this section with the following: Knee or hip replacement or reattachment surgery without major complications.
At first this was confusing. Why the part about reattachment surgery? On my first attempt I deleted the extra verbiage and just typed knee replacement. Nothing came up. Nerd wallet is most likely using medicare categories that were already defined in the database.
A neat and easy to read graph comes up and you can pull data from that. You should be seeing the graph of Patient volume compared to hospital charges.
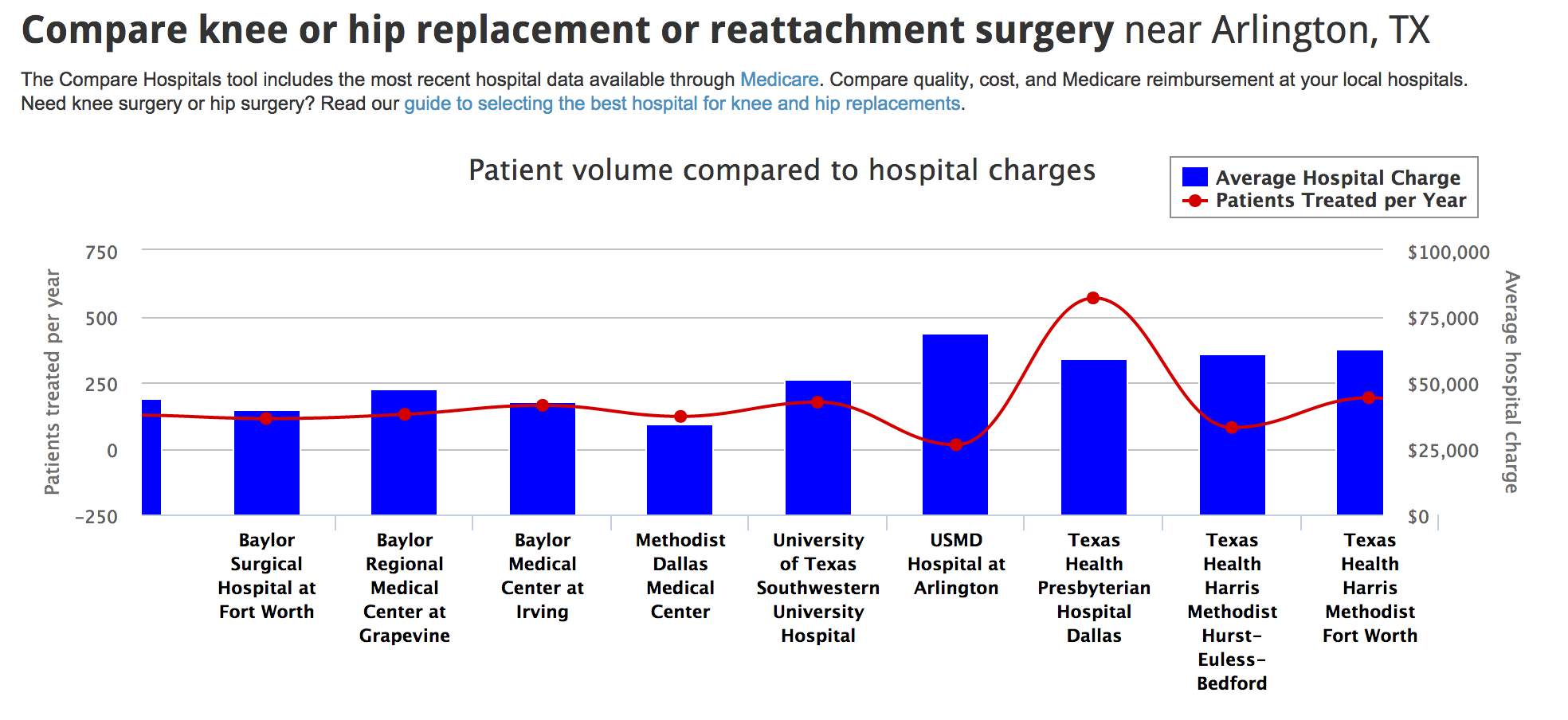
200 Quality Benchmark
Remember for bigger markets there is a sider across the bottom that allows you to scroll from right to left to find the best hospitals for knee replacement surgery in your area.
Conclusions from multiple studies have revealed that hospitals that perform over 200 surgeries annually have significantly less complications and better overall outcomes. They same principle holds true for surgeons. Find the best doctors for knee r replacement surgery and not the ones who do general orthopedics. For example, don’t make the mistake of finding a high volume hospital only to have your surgery performed by a low volume surgeon. Fit both pieces of the puzzle together and significantly increase your chances of achieving a great outcome.
If you want to make your head swim, click on the tab that says hospital charges compared to medicare reimbursement. The discrepancies in pricing and reimbursement across facilities is hard to fathom.
Summary
Hospitals with over 200 total knee replacement surgeries have lower rates of infection, heart attacks, blood clots, pneumonia and death
2,750 hospitals were evaluated
Only one in 4 hospitals meet the benchmark
2 in 5 patients will not be treated in a benchmark hospital
The Hospital for Special Surgery in NY has the highest patient volume at 3,833 treated in 2011
If you were wondering what to take to the hospital for knee replacement surgery..Read more
The post Find the Best Hospitals for Knee Replacement Surgery In Less Than 1 Minute appeared first on .
High Flexion/Gender Specific Knee Replacement Devices- Are They Better?
Additional evidence released this time from the British Journal of Medicine suggests that the high flexion knee and gender specific knee replacement implants do not improve function or patient related outcomes. After a review of 118 studies, they concluded that …
there was no clinically relevant improved benefits for these devices compared with older and established alternative implants. Furthermore, neither of these technologies was found to be safer or to have better survival than the established implants. In fact, high flexion implants in total knee replacement had inferior survival.
Assumptions About Knee Replacement Implants
The authors discussed many critical issues related to implant testing and approval that will probably shock and surprise.
Check carefully to see if you could be making one or more erroneous assumptions about the knee replacement implant industry?
Assumption 1: Present systems on the market are carefully vetted through controlled and evidence based studies. WRONG
Our goals are to highlight that the status quo regarding the introduction of new device technologies is not acceptable, that substantial efforts are needed by all stakeholders to invest in systems of careful evaluation and to promote controlled and evidence based introduction of device innovations.
Assumption 2: Benefits of new implants have been convincingly established prior to marketing. WRONG
This is particularly important when the comparative benefits of new device related technologies have not been convincingly demonstrated. Exposing large numbers of patients to new devices with uncertain safety could be considered unethical and should be avoided without controlled introduction and proper systems of evaluation. In this context, stepwise introduction of device related technologies has been proposed
Assumption 3: The risks of releasing new implants on the general population have been throughly evaluated prior to marketing. WRONG
For now, the need for new device technologies and the associated expected benefits need to be carefully balanced against the possible associated risks. We suggest adherence to the IDEAL recommendations, and when clinically relevant improvements have not been convincingly shown widespread commercial introduction should be deferred until appropriate long term safety comparable to existing technologies has been demonstrated.
No Criticism Of the Surgical Community or Orthopedic Industry Intended
The search for implants with superior functional outcome, increased longevity, and better survival is needed. Hence, this review is not intended to criticise the surgical community or orthopaedic industry.
Pathway for Implant Approval
At this time, as moderate-risk, class 2 medical devices, incremental changes to devices can be made through the 510(k) pathway, which requires manufacturers to demonstrate that the new product is “substantially equivalent” to the design that was previously approved. The authors of the study suggest that improved features should be tested in smaller groups of patients before being approved for wider use.
Others have suggested that a black box warning of sorts for knee replacement devices could help correct the misapprehension of benefits and understating of risks inherent in new devices that current marketing engenders in the public.
You might also be making one or more erroneous assumptions about total knee replacement rehab. Read more
WHAT THE FDA REQUIRES FOR CLASS 2 AND CLASS 3 DEVICES
Premarket Notification (510(k))
510(k) is required when demonstrating substantial equivalence to a legally marketed device, when making significant modifications to a marketed device, and when a person required to register with FDA introduces a device for the first time. If a device requires the submission of a 510(k), it cannot be commercially distributed until the FDA authorizes it.
Substantial Equivalence
A device is substantially equivalent (SE) if it has the same intended use and same technological characteristics as a legally marketed device, known as the predicate. A legally marketed device:
1. was legally marketed prior to May 28, 1976 (“preamendments device”), for which a PMA is not required, or
2. was reclassified from Class III to Class II or Class I, or
3. was found SE through the 510(k) process.
Applicants must compare their device to one or more similar legally marketed devices and make and support their SE claims. If the device is SE to a predicate, it is placed in the same class. If it is not SE, it becomes non-SE and is placed into Class III.
Examples of 510(k)s include x-ray machines, dialysis machines, fetal monitors, lithotripsy machines, and muscle stimulators.
Premarket Approval (PMA)
PMA refers to the scientific and regulatory review necessary to evaluate the safety and effectiveness of Class III devices or devices that were found not substantially equivalent to a Class I or II predicate through the 510(k) process.
PMA is the most involved process. To reasonably assure that a device is safe and effective, PMA requires valid scientific evidence that the probable benefits to health from the intended use of a device outweigh the probable risks, and that the device will significantly help a large portion of the target population. Sources of valid scientific evidence may include well controlled investigations, partially controlled studies, historical controls, well documented case histories by qualified experts, and robust human experience.
Independence is an important concept for PMAs, meaning that each PMA should establish the safety and effectiveness of the device under review, and that data about one device cannot be used to support another.
Examples of PMAs include digital mammography, minimally invasive and non-invasive glucose testing devices, implanted defibrillators, and implantable middle ear devices.
The post High Flexion/Gender Specific Knee Replacement Devices- Are They Better? appeared first on .
“Pre-habilitation” Lowers The Cost of Knee Replacement Rehabilitation
According to a recent study in the Journal of Bone and Joint Surgery, patients receiving preoperative physical therapy (knee replacement pre-habilitation) showed a 29 percent reduction in post-operative care use following a total knee replacement.
A big part of a physical therapy pre-habilitation session is about setting expectations and educating patients for the post-operative experience. They general consist of 1 or 2 sessions and cost in the range of $100. The study examined historical claims data from the Centers for Medicare & Medicaid Services and found the following:
• 54.2 percent of the preoperative knee replacement physical therapy group required postoperative care services, compared to 79.7 percent of the patients who did not have preoperative therapy.
• The decline in postoperative care services resulted in an adjusted cost reduction of $1,215 per patient, due largely to lower costs for skilled nursing facility and home health agency care.
What does this mean for You?
Exercises may be prescribed to help maintain strength and promote range of motion of the knee joint itself prior to total knee replacement surgery. As a rule, the more you have (strength and range) going into the surgery, the higher your starting point when you exit surgery.
Fifteen years ago, knee replacement candidates would wait as long as possible before submitting to the surgery. In doing so they would invariably lose strength and range in their knee from disuse, making the post surgical total knee replacement rehabilitation protocol much more of an uphill climb. An understandable problem because the surgery was and is a procedure of last resort.
Additionally, the pre-habilitation sessions often do not take place far enough in advance to allow for noticeable increases in strength and range and the limits of pain naturally hinder this development as well.
So what is driving the decrease utilization of total knee replacement rehabilitation services in this study? Education is the primary focus in a pre-habilitation session.
Becoming familiar with the principles and strategies of sound knee replacement recovery before your head is filled with narcotic pain medicine is an absolute game changer. If you get educated on what works, avoid pitfalls common to knee replacement patients and get your game plan down ahead of time, you will be well ahead of the crowd.
Nothing beats getting armed with solid insider information before you find yourself in the midst of a struggle. By all means take a pre-habilitation session or better yet grab my book on Amazon, get a cup of coffee, curl up on the sofa and do your pre-habilitation session right there. For the cost of a couple caramel macchiatos at Starbucks, you can get the information that will save you time, money and frustration.
Research Study on Pre-habilitation of Longer Duration
This is a study that included 4-8weeks of pre-habilitation which is not typical but was done for research purposes.
The post “Pre-habilitation” Lowers The Cost of Knee Replacement Rehabilitation appeared first on .
Knee Replacement Recovery Time
In a fast-paced world, “How long does knee replacement recovery take?” is one of the most common questions asked about the surgery.
Other similar questions include, How long will I be “out” of my normal routine?How long before I can be active again the way that I used to be? When can I drive? Will I be able to attend my granddaughter’s graduation in 1month?Can I go on the cruise my husband and I planned for our wedding anniversary in 2 months? Can I drive over 3 hours to celebrate thanksgiving with my family weeks after surgery?
If you have asked one of these questions or a similar question, you are not alone.
A timeline created by healthline shows the recovery trajectory according to traditional industry standards.
This infographic covers the “average” recovery timeline. As noted from the graph, time frames for passing through phases II through IV are variable and can last from 1 to 3 weeks.
Why Do Recovery Times Vary So Much?
Why does it take some people 1 week to get through phase II and another person 3 weeks? This is the million dollar question. Knee replacement recovery is very simple when done right. The problems occur when patients fall into a number of booby traps that will cause them to treadmill; working and working but not making true progress. Identifying those pitfalls and showing how to avoid them is critical.
What is important to realize is that you do not want to leave a 1-3 weeks variability to chance.
After years in the industry, I can predictably tell you where people go wrong and the ways knee replacement recovery is unwittingly prolonged. My book will give you all the answers in easy to read layman’s language. It can be read in 1-3 evenings and will act like an insurance plan in case your assigned rehab professional isn’t quite as experienced.
Double Knee Replacement Recovery Time
What is different about bilateral knee replacement recovery? Of course it’s double the rehab work and usually requires a facility placement secondary to the difficulty of coming to stand from average height furniture found in a typical home. A raised hospital bed is a godsend and facilitate early mobility.
Most people are aware of the slightly higher risk associated because of the added length of the surgery itself. The risks associated with knee replacement rehab are elevated as well. Everyone has heard of people who had a “bad” single knee outcome unrelated to poor surgical technique, but a “bad” double knee outcome can be disastrous. If you are planning to do two knees at once, don’t proceed without educating yourself about the rehab process before surgery. Be able to commit ahead of time to the work involved and the level of diligence required. Read more about the mental aspect of knee replacement recovery here
Knee Replacement Recovery Time-Average Swelling
Managing swelling is one of the key points of control and is critical for success. Strive to achieve a steady and consistent reduction in swelling. If you have significant fluctuations, swelling being manageable one day and then blowing up the next, chances are that rehabilitation mistakes are being made. The two main culprits are; increased wt bearing/walking early on in recovery or too aggressive therapy. Aggressive being defined by a resulting reactionary swelling following a physical therapy treatment period.
Knee Pain Recovery Time
Ideally, pain levels should remain fairly stable, and not fluctuate wildly. To achieve this, use narcotic pain medicine for the first two weeks after knee replacement surgery at the prescribed dosage to deal with the chemical pain of trauma. This advice is similar to what I mentioned about swelling. Wild fluctuations in pain will hinder the desire to do just about anything consistently, not to mention focusing on range of motion, which is the number one goal following surgery.
Not focusing on range early in the game is one of the biggest mistakes made by total knee replacement patients. After the first couple of weeks or earlier, patients want off of the narcotic pain pills for multiple reasons. Range development without the assistance of narcotics usually results in prolonged knee replacement recovery marked by a dreadful snail’s pace.
Achieving 90 degrees range of motion by the end of your hospital stay, should be the first benchmark (Medication levels are at their highest). The second goal is 120-125 degrees range of motion in 2 weeks provided there have been no long term range restrictions prior to surgery.
Bottom line, waiting to develop range will inevitably lengthen the struggle with “pain” and discomfort.
Fast knee replacement recovery comes as a result of implementing certain proven steps, some of which have been explained above. Follow the link to find out more.
The post Knee Replacement Recovery Time appeared first on .
What Are The Best Knee Replacement Exercises?
Best Knee Replacement Exercises
There are literally 100’s of exercises to choose from following a knee replacement surgery. Selecting the best exercise(s) without any rehab experience is a bit like trying to determine which exercises you should choose to become a better golfer. You would be forced to admit that a golf-pro would likely select an “exercise progression” from simple to complex that would maximize results. So the better question to ask is which exercises should I choose and at what stage should I perform them?
Luckily, knee replacement recovery is not as difficult a task as becoming a good golfer but the principle still applies. An extremely common mistake made by patients and rehab personnel alike, is to try to do too many exercises, too soon after surgery.
Here is an example: In the two weeks after surgery the most important goal is to regain your knee range of motion. Spending a bunch of time doing standing exercises for hip flexion, extension and abduction (up in front, back and out to the side) is a waste of time for this phase in your recovery.
Could your hip use a bit of strengthening? Of course since you have probably been limiting the activity of that limb secondary to your knee pain. But this strengthening can be achieved later during the functional mobility stage where you can strengthen the hip and knee at the same time.
Attempting these exercises in the first 2 weeks will simply result in having less time and energy to focus on the real task of range of motion recovery for that period. You can learn more about a proper exercise progression here.
Home Knee Replacement Exercises
There are many knee replacement exercises that can and should be performed in the home. Why pay for access to fancy equipment and machines when you lack a basic level of strength in your knee and you are still working on range? Paying 40 dollars for a copay, to have someone stretch your knee on a mat when there are easy exercises you could do at home is a waste of money.
Home knee replacement exercises should accomplish three goals
1) Range of motion to 120-125
2) Basic strength as evidenced by ability to do basic exercise group 4x/ day with 2 1/2 lb ankle weights
3) Begin functional mobility exercises
Paying for outpatient knee replacement therapy makes much more sense after you have completed these three goals. You’ll get much more bang for the buck from your outpatient therapy treatment program.

http://www.inc.com/articles/201107/wh...
Knee Replacement Exercises To Avoid
No matter what, try to avoid using an upright stationary bike to increase your knee range of motion, especially a Schwinn Airdyne. Schwinn Airdyne’s have a large fan in front and levers for your arms that allow you to push and pull with the leg motion.
The problem with this piece of equipment is that the rotation builds up momentum that cannot be easily stopped. This can cause you to inadvertently push the knee too far into flexion causing a sharp pain that can linger for 48 hours. This will put your recovery on hold while adding to your overall pain and frustration.
A regular upright exercise bike is not much better. It lacks precision control to slowly to methodical advance knee range of motion.
Another exercise to avoid is standing squats in the first 2 weeks or so. If you can not do a straight leg raise by yourself with some light wt., there is no way I want you using your post surgical knee to lower and raise your entire body weight which is of course much more than a light ankle wt. (2 1/2lb). This is a simple case of too much too soon.
Knee Replacement Exercise Equipment
The best exercise equipment to have in the home are as follows:
Some sort of a low friction board on which to slide your leg/foot.
An adjustable ankle weight (comes in a box with 2 weight cuffs that total 2 1/2lb each but have adjustable elements like a slug or little sand bag that allows you to modulate the weight of the cuff from 1- 2 1/2lb)
A towel folded lengthwise and then rolled (Put duck tape or rubber bands around it to keep it in a roll)
A strap to assist in knee range of motion or the Recovery bar-a tool specifically designed for promoting quick knee replacement range of motion recovery.
Re-usable Cold Pack
 for reduction of swelling and pain relief
for reduction of swelling and pain reliefAccess to a stationary bike once you have gained back the proper range of motion to safely perform the exercise is a great help. Of course you can always go to a gym or rehab center if needed.
For explanation of how these can be used to accelerate your recovery from a knee replacement. Check out my book that explains the ins and outs of speedy recovery.
The post What Are The Best Knee Replacement Exercises? appeared first on .


