
Michelle Stiles's Blog, page 4
September 13, 2015
Get Your Knee Replacement Surgery Before January 2016 If You Live in These Cities
The Center for Medicare and Medicaid Services innovation center has started something new- mandatory testing for bundled payment of knee replacement services starting in January 2016 and ending on December 31st, 2020 in 75 cities around the country. Click here for PDF of cities.
 The Comprehensive Care for Joint Replacement model (CCJR) proposes saving money by lumping all payments for an entire episode of care (hospital admission, procedure and services through a 90 period following surgery) into one payment made to the hospital. Hospitals will be responsible for partnering with other entities (MD’s skilled nursing facilities, Home Health Agencies, physical therapy clinics etc.) to bring down overall costs while improving care.
The Comprehensive Care for Joint Replacement model (CCJR) proposes saving money by lumping all payments for an entire episode of care (hospital admission, procedure and services through a 90 period following surgery) into one payment made to the hospital. Hospitals will be responsible for partnering with other entities (MD’s skilled nursing facilities, Home Health Agencies, physical therapy clinics etc.) to bring down overall costs while improving care.
According to the rule proposal, CMS expects the CCJR Model to improve patient care “by improving the coordination and transition of care, improving the coordination of items and services paid for through Medicare Fee-For-Service (FFS), encouraging more provider investment in infrastructure and redesigned care processes for higher quality and more efficient service delivery, and incentivizing higher value care across the inpatient and post-acute care spectrum spanning the episode of care, ” and simultaneously to lower costs. Has anyone seen a unicorn lately, right and I haven’t seen any government programs that lower cost and improve quality either.
Ultimately, hospitals will be rewarded with a share of the cost savings or forced to payback money to Medicare if they exceed costs.
This is euphemistically called value-based care and represents a tectonic shift in the current healthcare model. For the first time, health care entities will be incentivized for withholding care and/or cannibalizing the services of other healthcare practitioners’ or entities. Given man’s natural tendency toward greed this cannot be deemed a step forward for the future of knee replacement quality of care.
But Wait The Government Is Here To Protect You
Of course CMS would object to this statement because they have created so-called protections that would safeguard Medicare and Medicaid recipients.
The Audit
CMS proposes to use their authority, if necessary, to audit participant hospitals if claims analysis indicates an inappropriate change in delivered services.
Quality Measures
CMS proposes a complication measure, readmission measure, and a patient experience survey measure for the CCJR model. These measures will assess the priorities of safer care, transitions of care and effective communication and engagement of patients in their care, respectively.
Public Display of Quality Measures
CMS proposes the public display of measure results as an important way to educate the public on hospital performance and increase the transparency of the model.
In Reality
There are lots of ways for the quality of care to decline. The problem with these safeguards is that complications and readmissions are already very low, and secondly the patient experience survey is limited to data from the hospital only.
Risks To Patients
The monstrous 500-page proposal includes several other words of caution regarding what could go possibly go wrong for patients. You can read that proposal here if you have about 5-7 spare hours on a lazy Sunday afternoon and some aspirin tablets lying around.
Lack of Choi
 ce
ceIn the governments own words…
”We believe that existing Medicare provisions can be effective in protecting beneficiary freedom of choice and access to appropriate care under the CCJR model. However, because the CCJR model is designed to promote efficiencies in the delivery of all care associated with lower extremity joint replacement procedures, providers may seek greater control over the continuum of care and, in some cases, could attempt to direct beneficiaries into care pathways that save money at the expense of beneficiary choice or even beneficiary outcomes. As such, we acknowledge that some additional safeguards may be necessary under the CCJR model as providers are simultaneously seeking opportunities to decrease costs and utilization. We believe that it is important to consider any possibility of adverse consequences to patients and to ensure that sufficient controls are in place to protect Medicare beneficiaries receiving lower extremity joint replacement related services under the CCJR model.”
Potential Dumping of Complex Patients
In the governments own words…
“Given that participant hospitals would receive a reconciliation payment when they are able to reduce average costs per case and meet quality thresholds, they could have an incentive to avoid complex, high cost cases by referring them to nearby facilities or specialty referral centers. “
Potential for Decrease Quality of Care
In the governments own words…
“As was noted previously, in any payment system that promotes efficiencies of care delivery, there may be opportunities to direct patients say from more expensive services at the expense of outcomes and quality.”
Potential Delay of Treatment
In the governments own words…
“This model is based in part on an incentive for hospitals to create efficiencies in the delivery of care within a 90-day episode following the joint replacement surgery. Theoretically this basis could create incentives for hospitals and other CCJR collaborators involved in any CCJR Sharing Arrangements to delay services until after that window has closed.”
The Bottom Line
Is seems curious that replacement surgeries currently performed at very high levels of efficiency and effectiveness in this country would be so targeted by CMS. CMS states that this effort is about improving care and saving money.![]()
Remember the learning curve back in high school? Out on the edges of the curve, small levels of improvement are only achieved with high cost.
The cost in this case is massive government intervention and all the fallout that entails. In the form of unintended consequences. Will these small levels of improvement be worth it for patients and healthcare workers alike?
Secondly, if you read through to the end of the proposal, CMS projects that costs of replacements over 5 years for the 75 cities will be 12, 321,000,000. And are you ready for this? The savings over 5 years is estimated at 153 million. Ouch, only 1.2%. This can not be about cost savings.
So What Is This Really All About?
I am going to go out on a limb here and predict what I think this project is all about.
 I have written previously about the Tsunami of coming surgeries as a result of aging baby boomers (see article). At some point rationing will begin. Hidden away in the midst of this project, is an interesting request for hospitals to collect data 90 days pre-surgery and one-year post surgery on every patient’s functional abilities. The hospitals will benefit financially from collecting this data in the form of high reimbursements and so are likely to comply.
I have written previously about the Tsunami of coming surgeries as a result of aging baby boomers (see article). At some point rationing will begin. Hidden away in the midst of this project, is an interesting request for hospitals to collect data 90 days pre-surgery and one-year post surgery on every patient’s functional abilities. The hospitals will benefit financially from collecting this data in the form of high reimbursements and so are likely to comply.
Forgive me for being skeptical, but the outcome data is needed to assess definitively who fails to benefit from a functional standpoint and ultimately who gets care denied.
Instead of attaining the elusive and dubiously achievable twin goals of better care with less cost, they will be creating the actuarial tables for denial and in the process overlaying more bureaucracy and oversight, including the power of the audit, on an already burdened system. This will increase the likelihood that excellent surgeons and caregivers will retire without talented replacements in the waiting.
Seriously what surgeon wants to spend 1/3 of his life training just to become an employee of corporate America?
The other major result of this proposal as it rolls out across the entire country will be many smaller hospitals now offering the surgery will stop doing so because of the possible penalties involved leaving only the larger centers of excellence to do the job.
Whle this may seem attractive to achieve higher quality, having less choice on where to have the surgery, having to travel farther or wait longer because capacity has shrunk are not positives at all.
Big hospitals end up with monopolies and inevitably quality starts to decline soon after all competition has been eliminated.


August 17, 2015
Home or Skilled Nursing Facility After Knee Replacement Surgery?
There Is No Place Like Home
For over 20 years I have been recommending going home after knee replacement surgery rather than to a skilled nursing facility. I have previously detailed my reasons for choosing the home environment elsewhere.
But I would like to share with you an additional study that has relevance to this discussion even though it was done with data from total hip replacement Patients.
In the recent past, many facilities have undergone facelifts from interior designers and structural changes in order to draw and attract short-term stays by replacement clientele. While not quite Club Med, these are no longer your grandmother’s nursing homes.
So while Medicare changes in reimbursement rates in 1991 were incentivizing hospitals to shorten the length of stay for typical surgical procedures, skilled nursing facilities were see a growing opportunity to increase their bottom line by providing short term care for those who felt they were not ready to go home.
The length of stay for a total hip replacement dropped from an average of 9.1 days in 1991 to 3.7 days in 2008. In addition the proportion of patient discharged directly home declined from 68% to 48% and the proportion of patients discharged directly to skilled care increased from 17.8% to 34.3 %.
A study of Medicare recipients during 1991 to 2008 reveal that 30-day hospital readmissions increased from 5.8% to 8.5% for primary total hip replacements and from 8.7% to 14.1% for revision hip replacements.
Is A Shorter Length of Stay At A Hospital The Reason For Increase Readmission Rates?
So what caused the increase in readmission rates? Typically it is thought that the reduction in length of stay at the hospital has lead to discharging more unstable patients and is being used to justify going to a bundled payment system in which Medicare will penalize hospitals for “patient dumping” by holding them responsible for increasing costs throughout the episode.
Indeed the following quote from the study conclusions highlights this thinking.
These findings reinforce the potential wisdom of moving to bundled payments, reimbursing for episodes of care, or a combination of both as a way for incentivizing the correct LOS [length of stay], rather than perpetual reductions in LOS that seem to be occurring.
The trouble with this study is that it failed to look into whether the choice between home care and SNF might not have influenced readmission rates.
Medicare cites surgical infections (18.8%) as the top reason for hospital readmissions for both hip and knee replacements. In fact a study done in 2009 determined that, after controlling for ASA score, age, sex, and hospital complications, the odds of complications and hospital readmission are higher for elective patients who are discharged to an SNF after lower extremity joint arthroplasty and a short LOS (average, 3.6 days) than those discharged home.
Wanting to stay at a swanky SNF (aka Club Med) after a knee replacement?
You might want to rethink that option.
My contention all along has been that SNF’s are likely to increase a person’s infection rate because it put patients in close proximity to germs that would not normally be found in their own home environment.
By the way, several other things that have been deemed to put patients at higher risk for infection include the following: prior open surgical procedures, immunosuppressive therapy, poor nutrition, hypokalemia, diabetes mellitus, obesity, a history of smoking and surgery that took longer than 2.5 hours.
For a more detailed look into several other reasons I recommend home care following a total knee, see the following article
Sources:
Clinical Characteristics and Outcomes of Medicare Patients Undergoing Total Hip Arthroplasty, 1991-2008.
http://jama.jamanetwork.com/article.a...
Comprehensive Care for Joint Replacements Monograph.
Infection in total knee replacement: a retrospective review of 6489 total knee replacements.
http://www.ncbi.nlm.nih.gov/pubmed/11716377
Does Discharge Disposition After Primary Total Joint Arthroplasty Affect Readmission Rates?
http://www.kpimplantregistries.org/Pu... Disposition.pdf
May 19, 2015
Truth Telling MD Debunks Knee Replacement Surgical Claims
The round up is going to occur every so often-basically when I feel there is enough quality information to pass onto you and will include a brief summary and hopefully some insights.
Truth Telling MD Debunks Knee Replacement Surgical Claims on the Net
The first sentence of this next article starts out “Total knee replacements are one of the most successful procedures in all of medicine.” Over 6,000 websites contain this exact sentence.” Actually google searching in NY yields over 9,000 results of pages that use this exact phrase. Much of what passes as information today is swiped from one or two places and repeated over and over again. Oh snap now my article will come up in the results as well for this phrase.
I work really hard to avoid passing on what I think is meaningless information or outright marketing hype. I want to highlighted this next article because it was written by an MD who chronicles his forthright comments as he searches the google search engine results for knee replacement + New Orleans. He is reading between the lines of the slick advertising and so should you. Enjoy.

Knee Replacements – New Orleans Magazine – May 2015 – New Orleans, LA “Total knee replacements are one of the most successful procedures in all of medicine.” Over 6,000 websites contain this exact sentence.
A Google search linking knee replacement and New Orleans returned 244,000 hits one day and 246,000 the next. The first site to pop up, fueled no doubt by some payment to Google, promises an “advanced technology and technique” yielding better clinical outcomes, quicker recovery time, reduced pain, highly accurate placement of knee implants and shorter hospital stays.
Checking a Medicare website, I was unable to verify the claim of shorter hospital stays, but this hospital’s complication rate after knee replacements was “no different than the national rate.” Looking at other measures this hospital reported fewer intravenous line infections but more surgical site infections after colon surgery. And the amount of time patients were kept in their emergency room before admission was almost twice the Louisiana average.
The second hit took me to a company website promoting a replacement joint “lab-tested to simulate the number of steps the average person takes in 30 years.” Insert your location in their Find a Physician box ,and up pop names of select orthopedic surgeons who use their “exclusive technology.” There were eight surgeons certified to use their specific device on the Northshore but only four in Jefferson and Orleans parishes. Scrolling down to technical notes, I read, “The results of laboratory wear simulation testing have not been proven to predict actual joint durability and performance in people.”
The third hit was a Northshore orthopedic surgeon who believes in “the body’s natural ability to heal itself.” Another local practice site describes in laymen language what knee replacement involves both during and after surgery. I searched some text from this local website online and found huge hunks of identical wordage online from Mayo Clinic.
Angie’s List popped up part way down the first page of hits. It promised to name 12 knee replacement surgeons to avoid and 35 top-rated ones. When they asked for my credit card number to collect a monthly fee, I moved on, knowing that office staff and PR firms can outdo even former Assistant Federal Attorneys in their posting abilities.
Another link was to an archived local television news segment reporting how “a local surgeon has created a way for knee replacement patients to go home the same day and heal faster.” Turns out the Rapid Recovery Knee Replacement this team “created” is a an off-the-shelf program sold to hospitals and physicians to market and streamline joint replacement surgeries with an eye for higher revenue returns.
OutPatient Knee Replacement:The Next Big Thing
There is a big push to lower the cost of knee replacements as large volumes of surgeries are helping to accelerate healthcare costs. In the first article, Brobson Lutz, MD. talked about an ” off-the-shelf program sold to hospitals and physicians to market and streamline joint replacement surgeries with an eye for higher revenue returns.” There are pros and cons for outpatient surgery and I’ll be doing a full article soon but keep in mind this revolution is not patient centric. You will see plenty of articles similar to the one below. Beware. Mostly these are glorified press releases promoting the strategy as part of an advertising campaign by the hospital…My advice at this point is to avoid right now until more data comes in.
Cabell Huntington Hospital performs outpatient knee replacementAlthough total knee replacements are more or less common these days, Cabell Huntington Hospital reports performing something new — a total knee replacement done on an outpatient basis.
“Still, even today, only about 1 percent of total joint replacements in this country are done on an outpatient basis, and I’m delighted to report that we have the framework and ability to do this in Huntington.” Cabell Huntington Hospital performs outpatient knee replacement – Business, Government Legal News from throughout WV
More Reasons To Avoid Low Volume Hospitals
And if you needed more reasons to pick a high volume hospital read this really informative piece. Thde bottom line is if you live someplace rural SERIOUSLY consider having the surgery somewhere else even if that means you have to travel and stay with a family member or friend for awhile before heading home.
Risks Are High at Low-Volume HospitalsRisks Are High at Low-Volume Hospitals – US News As many as 11,000 deaths may have been prevented between 2010 and 2012 if patients who went to the lowest-volume fifth of the hospitals had gone to the highest-volume fifth.
Like other hospitals in thinly populated areas, Sterling Regional Medical Center does a bit of everything. The 25-bed Colorado hospital has its own heliport, delivers about 200 babies a year and admits more than 1,200 patients for a variety of conditions and procedures. Replacing worn and painful hips and knees is among them. To patients, the surgery may seem perfectly routine.
These large numbers of low-volume hospitals, the analysis found, continue to put patients at higher risk even after three decades of published research have demonstrated that patients are more likely to die or suffer complications when treated by doctors who only occasionally see similar patients rather than by experienced teams at hospitals with more patients and established protocols.
“You can save your life by picking the right place,” says Leah Binder, director of the Leapfrog Group, a consortium of major employers that emphasizes safety in measuring hospital performance.
May 7, 2015
The 5 Best Practices For Knee Replacement Surgery Recovery
How well will you do with your recovery? Most people will tell you that it depends on you and while that is true, there are best practices that when taken together constitute an effective system. Knee replacement surgery recovery can be accomplished with greater easy and less frustration when a well planned system is implemented which allows you to recover quickly from a knee replacement.
Could you climb the sand dune without the stairs (see featured image)? Of course, but thoughtfully constructed steps with handrails would sure beat a solo climb.
Here’s is a video that discusses the 5 best practices following knee replacement surgery that will significantly accelerate your recovery.
While you may not be able to find a surgeon or a hospital that is doing all 5, try to find one who is at least incorporating 3 or more of these best practices into his post-surgery knee replacement rehab system.
Keep in mind this is the ideal. Feel free to download the Knee Replacement Leverage Analysis (KLRA test) so that you can discuss this with your surgeon. Any questions please leave a comment.
Download The KRLA
April 28, 2015
Is The Rehab Industry Being Honest About the Effectiveness Of Their Treatment Methods?
In the last 10 years, a revolution of sorts has taken place in the knee replacement industry. Patients are younger, more active, and more likely to be in the workforce when needing knee replacement surgery. In many cases this means completing knee replacement rehab programs using paid time off (PTO) or vacation time, causing financial and/or life stress.
Knee replacement recovery protocols, despite the surge in younger patients remain tailored to retirees, and stifled by inertial forces that limit creativity and vision.
You probably didn’t know that in 2010, the American Physical Therapy Association admitted that
“The most efficient and cost effective way to achieve the goals of excellent range of motion and the ability to ambulate and self-progress with home exercise remains elusive.”
and
“No available evidence dictates which stretches are best and how often they should be performed.”

2010 State of Art Monograph
American Physical Therapy Association
Consider the following two outdated models of recovery:
Here is What Typically Happens in the The Spinning Wheels Model of Knee Replacement Recovery
Patients take limited pain medicine initially to avoid addiction or because they are not taught proper pain management. Then they exercise at too low a frequency to make progress and they lack good leverage methods. Most of the time they are just following instructions. The problem is they make slow and painstaking progress in therapy following knee replacement that can be compared to a hamster on a treadmill spinning his wheels.
Urgency to get back to work, forces them to get off the limited narcotics they were taking way before achieving significant range of motion recovery.
Back at work, they now have to find time and money for additional outpatient therapy treatments for total knee recovery while dealing with stiffness, pain and the frustration of a seemingly endless road to recovery.
The Rambo Model of Knee Replacement Recovery
Here is What Typically Happens:
Patients take an aggressive approach, attending outpatient PT directly after the hospital. They will be hopelessly mired in a cycle of pain and swelling because they have not respected the three sequential phases of knee replacement therapy. This will result in more overall pain and suffering and needless prolonging of the recovery time.
The average target for range recovery at week 11 and 13 is listed on Healthline, a well respected website, as “possibly 115 degrees” and “115 degrees” respectively.
PTO time may last 6 weeks if you are lucky, 12 weeks is too long to wait to get 115 degrees range of motion!
This is an unacceptable rehab trajectory for today’s knee replacement surgery candidates who are still in the workforce.
Want to learn about a better way?
If you have been following along with this multi-part series, you now understand how leverage, acting like a pump, can reduce the swelling in your knee and enable you to regain your range of motion swiftly and safely at a predictable rate following knee replacement surgery.
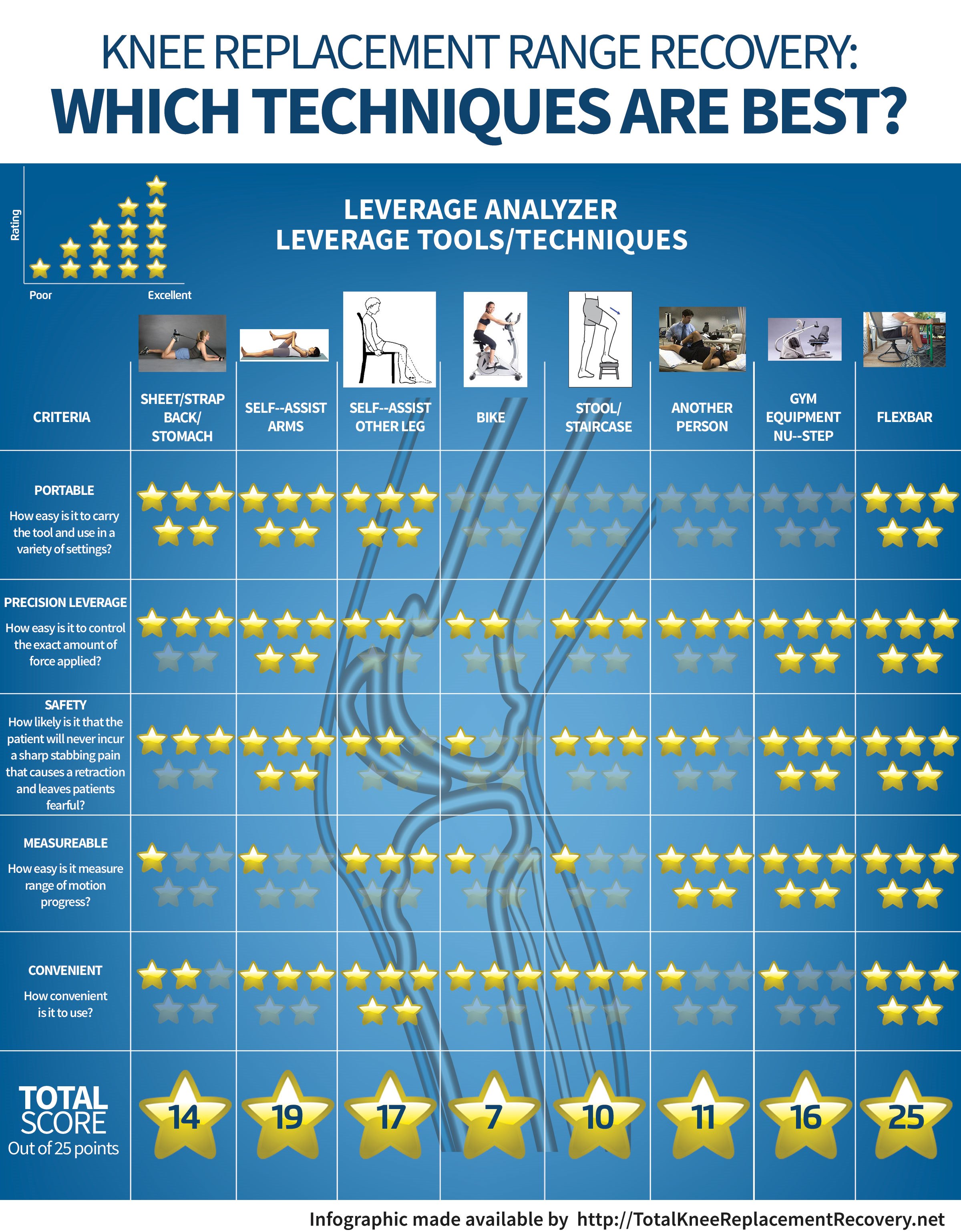
Two core principles from the No Days To Waste 7 Point Stretching Program were introduced, Feedback Loop and Power Leverage. We also unraveled the pros and cons of traditional leverage and feedback methods in visual format with the “Knee Replacement Recovery: Which Techniques Are Best” infographic.
The “No Days To Waste” Program is a powerful integrated system designed to achieve the following outcomes:
Return to work with at least 125 degrees range of motion
Reduce dependence on outpatient PT Clinics
Fast track the overall rehab process
Save money on outpatient services by not wasting time on range recovery
Get off narcotic pain medicine as quickly as possible
Limit risk of narcotic addiction and side effects
Want a fast start on your recovery?

April 9, 2015
Traditional Stretching Methods Could Prolong Your Knee Replacement Recovery!
In this lesson you are going to learn about how using traditional methods of stretching exercises after a knee replacement, ones that have been used for the past 20 years, may actually prolong your recovery and why. Anyone who has had a knee replacement will instantly recognize many of these methods. Leverage in many different forms is used to facilitate bending of a swollen resistant knee.
Initial reactions by many patients to this somewhat counter-intuitive concept is “Why Don’t I wait for the swelling to go down and THEN try to bend my knee?”. The answer to this is that waiting passively for knee swelling to go away is like waiting for evaporation to eliminate the flood waters that have entered your house-serious damage will have taken place in the meantime or at the very least a ridiculously unnecessary delay will have ensued.
 When you bend your knee it helps the body displace swelling located in the joint back into the body tissues similar to a mechanical pump removing flood waters from your home. Now that you have a basic understanding of why, we shall look at the traditional physical therapy after a knee replacement and the methods that fluid can be pumped.
When you bend your knee it helps the body displace swelling located in the joint back into the body tissues similar to a mechanical pump removing flood waters from your home. Now that you have a basic understanding of why, we shall look at the traditional physical therapy after a knee replacement and the methods that fluid can be pumped.Traditional Rehabilitation Leverage Methods Explained
Muscles in Your Own Leg (Leg slide) -This is probably one of the most well known knee replacement physical therapy exercises-sitting in a chair and attempting to slide your leg back as far as possible. This is the poorest leverage available secondary to the weakness that usually exists in the leg prior to surgery. Limitations: need for slick flooring surface.
Self-Assist Other Leg-This is similar to the stretch above except that it uses the non-surgical leg to assist the bend . Legs do not have as much fine motor control as the arms, and some people have trouble controlling the amount of force applied. Limitations: non-surgical leg is bad, bilateral surgery.
Sheet/Strap on your Stomach or Back-Lying on your back or stomach and using a sheet or strap to help pull the leg into flexion is another exercise after total knee replacement. Limitations: need a bed or ability to get up/down off the floor easily and safely, measurement.
Stool/Staircase-Stepping up onto a stool or a staircase and leaning forward will force a bend in the knee. Limitations: need equipment, staircase with a railing that is safe, balance, measurement.
Another Person-A physical therapist applies force to bend the knee for you or with your assistance. Limitations: very easy to over-do with resulting setback, availability.
Gym Equipment (Nu-step)-Equipment used in a physical therapy rehab setting that allows for a gradual increase of range that can be dialed out. Limitations: access.
Self-Assist Arms-Lying face up on the floor or bed and using your arms to assist the bending movement of your knee. Limitations: not for early stages of recovery, measurement.
Bike-Using a bike pedal and other leg to force a knee bend on the post-surgical side. Limitations: difficult to control force applied, easy to over-do.
The following infographic is a pictorial representation showing the weaknesses and strengths of each technique. The rating system is my own, developed over 20 years of practice.
As you can see, The F.L.EX bar is rated the highest of all the stretching techniques because it solves the majority of the problems associated with the other methods. The F.L.EX bar was designed specifically with knee replacement recovery in mind. (Click on image to enlarge)
Feel free to share this infographic with friends and neighbors as well as on Facebook, Twitter and other websites.
Share this Image On Your Site
Please include attribution to totalkneereplacementrecovery.net with this graphic.
The F.L.EX Bar is everything needed in a leverage system.
• Portable
• Convenient to Use
• Safe
• Measurable
• Precision Control
I hope you can see how a portable leverage tool that is easy to use in any room in the house or in any office in an upright position can offer massive value to the post-op surgical patient!
Traditiona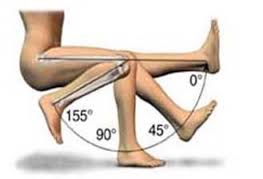 l Feedback Methods Explained
l Feedback Methods Explained
The physical therapist uses a tool called a goniometer to measure your progress at regular intervals. As we learned from part II of this series, not having access to your own feedback system can case massive delays and wasted time and effort. Fortunately there is a better way.
Tune in next to find out whether the rehab industry is really being honest about the effectiveness total knee replacement exercises?
If you missed the first two articles in the series you can find them here
Article One: How to Speed Up Recovery?
Article Two: The Number One Reason for Slow Recovery
Already know you want a fast start on your recovery?
March 27, 2015
The Number 1 Reason For Slow Knee Replacement Recovery
Imagine Training For A 220 Yard Dash Without A Stop Watch
Without a stop-watch athletes and coaches are sunk. There is no way to tell if a particular method of training is working. In short, no stopwatch, no feedback, No correction, no success! And this is where so many struggling with rehab for knee replacement go wrong.
Patients need a “stopwatch” for knee replacement training, because feedback loops are critical for any successful endeavor.
The type of feedback needed in recovery for a knee replacement is relative improvement in knee range of motion available with every session, not “verbal encouragement” like, “Doing well” or “Keep it up.
Feedback loops signal when work has been hard enough to make progress and when it has not, allowing for course corrections that save valuable time and effort. It will also yield critical information about overtraining.
This principle has been tested and proven in a multitude of disciplines and needs no outside endorsement. It does however need to be applied adequately to the challenge of rehab after a total knee.
Traditional Feedback
Traditionally, feedback after a knee replacement is intermittent in the form of a therapist using a device called a goniometer to measure the knee range of motion, daily at first, then dropping to several times a week. In other words, the average patient is in the dark trying to determine whether each session is effective or not. 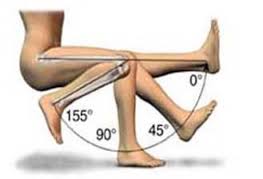
Patients might have some vague sense that they are better one day to the next as noted by the stiffness in their knee, but no hard, fast evidence.
The “No Days to Waste” 7 Point Stretching system includes measurement techniques that can be easily taken by the patient without the need for a therapist to be present. Patients are encouraged to see visual progress toward goals and get re-energized to continue working hard to obtain them.
Conversely, when they start to deviate from the program and lose traction, they are instantly alerted to the lack of progress. No more wasting days of recovery on poor technique and ineffective exercise.
Fool Proof System
Patients come to trust the system as they witness range of motion improve at a predictable 2-3 degree per day. The feedback loop is also invaluable in driving home the all-important emphasis about frequency. When frequency dips below 4x/day, patients have to work all that much harder next session to get back to baseline. They quickly realize that this is ultimately self-defeating.
When a goal involves some level of discomfort, it is easy to fool oneself into believing a particular effort was enough to achieve success. With the “No Days to Waste” Program, the guesswork is removed and steady progress maintained. No more overconfidence or cutting corners.
Tune in shortly to find out why traditional methods of stretching could actually slow you down.
Watch out for Part Three in this series where you will learn why traditional stretching methods could prolong your knee replacement recovery!
If you missed the first video Go HERE
Already know you want a fast start on your recovery?
March 24, 2015
In Honor of Obamacare Anniversary-Long Wait Times for Knee Replacement Surgery Coming To A Hospital Near You
I just couldn’t resist. The irony was too compelling, the contrast too stark to pass up. I was greeted in my inbox this morning by two seemingly unrelated emails. One notified me of an article published in the Ottawa citizen about wait times for knee replacement surgery. The other email was from whitehouse.gov-these actually have the potential to evoke laughter if there were not so many people in our country who believe the nonsense that pours forth as an oracle from “The One”.
 So here I am cup of coffee in hand, and while the whitehouse.gov is “celebrating the fifth anniversary of Obamacare, the Ottawa citizen was celebrating a reduction in the absurdly long wait times for knee replacement surgery candidates. Now candidates only have to wait … get this…one year. Victory!
So here I am cup of coffee in hand, and while the whitehouse.gov is “celebrating the fifth anniversary of Obamacare, the Ottawa citizen was celebrating a reduction in the absurdly long wait times for knee replacement surgery candidates. Now candidates only have to wait … get this…one year. Victory!
It was a supremely well-done Orwellian piece of journalism by a senior Ottawa Citizen journalist and a portent of what is to come here in the states. And it bears looking at the article in detail and recording for posterity. Later on I’ll be deemed prophetic and spot on…when really it was all right there in the Ottawa Citizen for anyone with eyes to see.
Here is the first quote
A few years ago, Soulière [a French person] likely would have faced a long, painful wait for surgery. But thanks to a central intake and assessment program that has sharply reduced wait times for people needing knee and hip replacements…
Yes thanks be to the government central intake and assessment system—Winston would be proud. They corrected an inefficient antiquated system of direct referral from physician to surgeon. The nerve of those people thinking they could bypass the government.
At any rate the new system was able to reduce by 40% of the number of people typically referred but that would not have ended up as knee replacement candidates. The article doesn’t tell us by what clairvoyant means the government was able to identify so called non-candidates but since the government central intake system personnel likely don’t have medical degrees I imagine it had something to do with money.
Quote Number 2
The old system also distributed patients unevenly among orthopedic surgeons, producing waiting lists for surgery that stretched to two years in some cases …Because the central approach distributes the surgical load more evenly among available surgeons, the long backlogs characteristic of the past have been largely eliminated, Sly-Haney explains.
There is a lot being said here between the lines. It seems clear that certain surgeons were favored over others by the referring doctor and/or the patients. I wonder why? Did the people get to pick their “new” doctor or were they simply assigned to one of the less poplar and/or less skilled surgeons?
Thank God for the central intake people, the poor slobs that are getting their knees done should NOT be allowed to wait for one of the best surgeons.
Quote Number 3
There’s capacity in the Champlain region to do more orthopedic surgeries, Schonberg says, but so far the province hasn’t anted up the necessary funding.
So glad the government will be picking winners and losers in the lottery for a new knee in the future.
Excess capacity and long wait times…Humm. Couldn’t they use the excess capacity to reduce the current wait times…oh that’s right …morale is so “good” among surgeons in Canada they must have a shortage.
It’s easy to see why this is working so well….
Treat surgeons so poorly that there is a shortage of needed labor
Weed out 40% of the candidates for surgery as determined by some actuarial table
Force patients to be operated on by the worst surgeons
Then declare a successful reduction in wait times
If only we had the government inserting itself in the midst of all of our problems.
Long Wait Times for Knee Replacement Surgery Coming
All this is coming to a hospital near year…despite obvious idiots celebrating Obamacare we have every reason to be worried. Mark my words it’s coming.
March 21, 2015
How To Speed Up Recovery After A Knee Replacement
With the signs of spring upon us it seems fitting that the theme of my next 4 posts will be about liberating yourself from a long and drawn out recovery following knee replacement surgery. While there are pockets of solid recovery instruction, I am painfully aware that many people will not have access and will find the recovery burdensome. So in honor of spring read on..because there is a method that achieves predictable AND excellent results.
During the course of my physical therapy career, I inadvertently stumbled on an interesting finding-I could predict patients knee replacement recovery in range of motion/per day, when they diligently followed the system that I taught them.
Nothing in my training or professional instruction prepared me for this revelation. Up to that point in my career, and even today conventional wisdom remains that, “All patients are different and progress at different rates based on their motivation, follow-through, and perhaps background. Despite everyone being given the same or similar knee replacement protocol, recovery after knee replacement surgery was and is highly variable.
What I had discovered was the synergistic effect of combining several well-established principles into a comprehensive system. I’ve named this system- “No Days to Waste”, because each and every person’s life is too valuable to waste weeks and even months struggling to recover after knee replacement surgery.
This post initiates a 4 part series introducing several of the core principles that make the No Days To Waste System so effective. I will also be using this series to explain the theory and uses of the F.L.EX Bar- a patented tool specifically created to promote accelerated knee range of motion recovery following a knee replacement.
Patients who purchase my book can get the F.L.EX bar blueprint that shows them how to make the tool at home. Since writing the book, readers who lack the interest or aptitude to make the bar have requested a purchase option. That is now a reality along with a new manual that goes into greater depth on how to implement and carry out the “No Days To Waste” Strategy.
Two Core Principles
Power leverage and the feedback Loop are two of the seven core principles that are used to speed up your range of motion recovery after a knee replacement.
For the sake of this series let’s assume you have adequate pain management. (less than 5 out of 10)
Power Leverage
Leverage is using some force besides the power of the surgical leg alone to assist in bending the knee. This is important because swelling tends to restrict your ability to bend the knee. The action of bending the knee helps drive fluid out of the knee and into the surrounding tissues. A good source of leverage makes it easier to bend the knee and accomplish the task of driving fluid out of the knee.
Now that you know why leverage is important, I want to teach you the parameters of how to control it.
Let’s Start With The Concept Of 3-Level Stretching.
A Level One Stretch is a low intensity stretch. It is a relatively easy motion that will only maintain your present range. Generally you are able to do other activities as well, like talk on the phone, watch TV or read the newspaper. Progress with range of motion will be minimal or non-existent if the intensity remains at this level. There is high potential to form adhesions when patients do not push onward.
A Level Two Stretch is a moderate intensity stretch. There will be some discomfort and feeling of pulling in your knee. Patients in this mode are focused and do not want to chit-chat or do anything else while so engaged. The stretching does not seem easy at first but after 10-20 repetitions and a 10-15 second hold, the knee loosens up and might even begin to feel more like a level one.
A Level Three Stretch is a high intensity stretch. You are at the end range of comfort and safety but will make excellent progress at this level. Discomfort should never be over 5/10. Your goal for each session should be to gradually get to Level 3. Being too aggressive in this level may cause a stretching injury and/or a stabbing, sharp painful sensation that causes automatic recoil from the stretch.
Commonly, patients fear applying force in therapy after knee replacement surgery because they have no idea how to approach a Level 3 stretch to get the benefit without the danger. This reality is why I only recommend certain types of leverage and why the additional principle of feedback is so important as a complimentary strategy.
The risk of danger in Level three can be mitigated with our next principle, feedback. The feedback method taught makes it easy to approach a low to mid-Level Three stretch with complete safety and confidence.
Watch out for Part Two in this series where you will learn about the number one reason for slow recovery.
Already know you want a fast start on your recovery?
March 13, 2015
Give Me 3 Minutes and I Will Tell You How to Accelerate Your Knee Replacement Recovery
To build the muscles of your knee back to full strength after knee replacement surgery or to build any muscle for that matter, you have to give the muscle a signal. What is that signal? You must ask the muscle to do something that it is not used to doing. When a new challenge presents itself and the muscle does not feel up to the challenge- the muscle will initiate steps to build up so that next time it will be ready.
The key is to not accelerate this challenge too quickly because your tendons have the potential to

Tell Your Muscles to Get Stronger
react in a negative way. Tendons need time to adjust to new challenges as well. Increasing a workload on a muscle too quickly can result in tendinitis, an inflammation that causes pain. It is a signal your body sends to tell you to slow down.
So if you are eager recovery quickly from your knee replacement surgery, knowing exactly how to ramp up your strength training without overdoing it is critical. So here is the key to knee replacement therapy success…
Purchase A Set Of Home Ankle Weights Before Your Knee Replacement Surgery
One of the best knee replacement exercise equipment pieces to purchase is an ankle weight. I know it’s not sexy, but it is so important. Just like a lot of things in life. Here are the criteria you should use when selecting a set.
Adjustable weight set (2 weight cuffs)
2-1/2 lb. each or 5 lb. total for the average total knee candidate [one-half pound increments]
5 lb. each or 10 lb. total for those heading back to physical occupations that are demanding or high activity levels.[one pound increments]
Adjustable units should be a slug or sand packet that ideally slip in and out on the outside of the weight cuff
Avoid zippered units like the plaque unless you like needlessly wasting time
The adjustable units of weight (1/2 lb Increments are best) increase the challenge systematically to ensure an even acceleration of strength without a set back.
I am sure many of you may be thinking …I don’t really need to do this because I will be going to physical therapy after my knee replacement. Rehabilitation facilities are great but most insurance companies will only pay for 3 days a week.
What will you be doing on the other days? Once your knee is strong enough to do active range of motion with weights, doing active range of motion without them do nothing to improve your knee strength. Yes you will be reducing stiffness and promoting blood flow, but you are spinning your wheels as it relates to strength training.
The other big reason to use a home weight set is to establish a base of strength at home that you can build on when you go to outpatient. I mean why on earth pay a $40 co-pay to do exercises at a rehab center that you could have performed at home? Save the $40 co-pay for using advanced strength building devices and save yourself some cash.

Here Are The Steps To Accelerate Your Knee Replacement Recovery
Step One:
Do 4 separate exercises sessions per day without weights doing each exercise 20-30 times.
Step Two:
When this can be performed with ease: Add 1/2 -1 pound ankle weight
* If adding the weight for all four sessions seems to hard… Add in for two of the sessions and work up to 4 sessions.
Step Three:
Continue to repeat step two until you can do 2 1/2 for all your exercises
At this point you have a very good base level of strength and in most cases this sequence can be completed in 2-3 weeks following surgery.
A simple weight set costs $10-15 at Walmart and can save you time by accelerating your recovery and save you money on PT co-pays. What are you waiting for?
Here are some examples of ankle Weights

Do Not Purchase -They Are Not Adjustable

Do Not Purchase-They Will Drive You Insane Trying to Adjust the Weight

A Good Low Cost Model

Premium Model Using Slugs That Can Be Inserted on the Outside
And if you have no extra money at all. Here is an idea to get a similar effect on the cheap. Remember though that you will need to make more than one or keep changing the amount of sand.


