
Leslie Glass's Blog, page 290
March 6, 2019
John Stamos Thanks Jodie Sweetin For His Sobriety
From Tyler McCarthy @ Fox News: John Stamos got to give a heartfelt thanks to his “Fuller House” co-star Jodie Sweetin for changing the course of his life through sobriety.
The 55-year-old star had the opportunity to introduce Sweetin at the Skirball Cultural Center in Los Angeles Thursday to present her with the Writers in Treatment’s Experience, Strength and Hope Award for her book about her journey to sobriety “Unsweetined” as well as the advocacy she’s done for the recovery community.
While introducing the former “Full House,” and current “Fuller House,” star, Variety reports that Stamos choked back tears as he described the impact that Sweetin had on his own journey of sobriety.
“It took me a long time, a long time disappointing everyone who cared about me, culminating in a terrible DUI where I could have killed somebody,” Stamos said. “I hit rock bottom. Jodie lovingly allowed me to walk my own path and when I finally humbled myself to ask for your help, I realized that the perky little blabbermouth had become the master of wisdom and was right by my side during some of the most difficult days of my life.”
The outlet reports that Sweetin was instrumental in organizing 12-step meetings for Stamos both at his house and on the set of the Netflix sitcom revival.
“Thank God, my wife and my new son will only know me as a sober husband and father,” the actor said. “This is Jodie’s legacy in my life.”
Stamos also took to Instagram to share his affection and gratitude for his on-screen niece.
“Proud moment last night honoring @jodiesweetin at the Experience, Hope & Strength Awards. Who knew this little blonde scene-stealer in a side pony-tale would grow up and change so many lives. (Mine included) Her sobriety is inspirational to say the least. Congrats Jodie on this award recognizing your extraordinary journey. You give so many people HOPE. Love you! UJ.”
After introducing Sweetin, who is eight years sober, she took the time to congratulate him on his four years of sobriety.
“John, I’m so proud of you and it’s been the greatest thing to watch someone that you love have the light come back on again,” she said.

The post John Stamos Thanks Jodie Sweetin For His Sobriety appeared first on Reach Out Recovery.


Fast Food To Fatten On
From The NY Times By Tiffany Hsu
Fast food chains have tried for years to woo health-conscious diners by mixing lighter fare like salads and yogurt with the usual burgers, fried chicken and shakes.
But as menus swelled over the past three decades with grilled chicken wraps (McDonald’s) and “fresco” burritos (Taco Bell), many options grew in size and the calories and sodium in them surged, according to new study from researchers at Boston University and Tufts.
The researchers studied 1,787 entrees, sides and desserts at 10 chains — Arby’s, Burger King, Carl’s Jr., Dairy Queen, Hardee’s, Jack in the Box, KFC, Long John Silver’s, McDonald’s and Wendy’s — from 1986 to 2016. In that time, the number of items in those three categories rose 226 percent.
According to the study — published last week in The Journal of the Academy of Nutrition and Dietetics — even with lighter items in the mix, fast food menus are less healthy than they were 30 years ago.
ENTREES
Bulging portions at the heart of the meal
The fat and salt content and the sheer size of fast food meals have long been a public health concern. They are often blamed for pushing up the obesity rate among adults in the United States, which rose to 40 percent in 2016 from 13 percent in the early 1960s.
The new study suggests the problem is getting worse.
Across the 10 chains, the researchers found, the average entree weighed 39 grams more in 2016 than in 1986 and had 90 more calories. It also had 41.6 percent of the recommended daily allotment of sodium, up from 27.8 percent.
Customers could be forgiven for not knowing. Local governments have adopted menu-labeling initiatives that require fast food restaurants to list calorie counts for the items they sell, but such measures have faced substantial opposition, including from the Food and Drug Administration.
“The restaurants really haven’t done enough,” Megan A. McCrory, the lead researcher, said. “The big picture is that there have been some positive changes, but they’re small, and over all, the changes have gotten worse.”
DESSERTS
More than just a little something sweet
In 2016, the average fast food dessert weighed an extra 71 grams and had 186 more calories than the average dessert 30 years earlier, the researchers found.
One possible reason is that restaurants are counting on bigger sundaes and cookies as a way of increasing the amount spent on each order and attracting more customers, said Darren Seifer, a food and beverage industry analyst at NPD.
“The majority of fast food traffic is around lunchtime, when people aren’t typically getting dessert,” he said. “But offering larger portion sizes is one way restaurants can promise more value.”
Just last month, McDonald’s introduced “donut sticks” dusted with cinnamon sugar. Six sticks have 280 calories. But you can also order a serving twice the size for less than the cost of two single orders.
SIDES
Adding those extras adds up
The researchers found that there were 42 more calories on average in items like chips, soups and French fries in 2016 than there were in 1986. Sodium content rose to 23.2 percent of the recommended daily allotment from 11.6 percent, even though portion size did not grow substantially.
Consumed together as a single meal, the study found, the average entree and side account for nearly 40 percent of a 2,000-calorie daily diet.
The study mentions several proposals meant to help consumers scale back their fast food intake, including a system that would let them order smaller portions at lower prices.
Whether the industry will embrace such ideas is unclear. In the meantime, menus continue to grow, sometimes blurring the line between entree and side. Jack in the Box is testing Burger Dippers, which the company describes as “the burger you eat like a fry.”
As with those that preceded them, some of the new offerings appear to be geared toward people who want to eat healthy foods. Carl’s Jr. recently added a plant-based burger, the Beyond Famous Star, to its lineup.
Ordered with cheese, it has more than 700 calories.
The post Fast Food To Fatten On appeared first on Reach Out Recovery.
March 5, 2019
How To Quit Antidepressants: Very Slowly, Doctors Say
From The New York Times:
Mustering solid evidence, two psychiatrists have denounced their field’s standard guidelines for how best to wean patients from depression medications.
Thousands, perhaps millions, of people who try to quit antidepressant drugs experience stinging withdrawal symptoms that last for months to years: insomnia, surges of anxiety, even so-called brain zaps, sensations of electric shock in the brain.
But doctors have dismissed or downplayed such symptoms, often attributing them to the recurrence of underlying mood problems.
The striking contrast between the patients’ experience and their doctors’ judgment has stirred heated debate in Britain, where last year the president of the Royal College of Psychiatrists publicly denied claims of lasting withdrawal in “the vast majority of patients.”
Patient-advocacy groups demanded a public retraction; psychiatrists, in the United States and abroad, came to the defense of the Royal College. Now, a pair of prominent British psychiatrists has broken ranks, calling the establishment’s position badly mistaken and the standard advice on withdrawal woefully inadequate.
In a paper published Tuesday in the Lancet, the authors argued that any responsible withdrawal regimen should have the patient tapering off medication over months or even years, depending on the individual, and not over four weeks, the boilerplate advice.
The paper is by far the strongest research-backed denunciation of standard tapering practice by members of the profession.
“I know people who stop suddenly and get no side effects,” said Dr. Mark Horowitz, a clinical research fellow at Britain’s National Health Service and King’s College London, and one of the paper’s authors.
But many people, he said, “have to pull apart their capsules and reduce the dosage bead by bead. We provided the science to back up what they’re already doing.”
The field of psychiatry has conducted few rigorous studies of antidepressant withdrawal, despite the fact that long-term prescription rates in the United States and Britain have doubled over the past decade, with similar trends in other Western countries.
More than 15 million Americans have taken the medications for at least five years, a rate that has almost more than tripled since 2000, according to a New York Times analysis of federal data.
Outside researchers who have studied withdrawal said the new paper was a welcome contribution. “I think what they’ve presented really reinforces what I’ve observed in clinical practice in many patients, and it’s almost identical to the tapering regimen I use,” said Dr. Dee Mangin, the chair of family medicine at McMaster University in Canada, who was not involved in the paper.
Dr. Mangin, who is completing her own two-year study of Prozac withdrawal, added, “The other important thing is that it validates patients’ own reports of their experiences. It’s tremendously frustrating when patients describe a different experience than physicians expect, and don’t feel they’re being heard.”
Dr. Horowitz and his co-author, Dr. David Taylor, a professor of psychopharmacology at King’s College and a member of the South London and Maudsley N.H.S. Foundation Trust, decided to address the topic in part because of their own experiences with medication.
Dr. Horowitz said he had severe withdrawal symptoms after tapering down after 15 years on antidepressants. Dr. Taylor had previously written about his own struggles trying to taper off.
The two psychiatrists began by visiting online forums in which people on antidepressants advised one another how best to withdraw. Those sites consistently recommended “micro-dosing,” reducing doses by ever smaller amounts over months or years, sometimes by removing one bead at a time from capsules.
The two researchers dug into the literature and found a handful of studies that provided evidence for that method.
In one 2010 study cited in the new paper, Japanese researchers found that 78 percent of people trying to taper off Paxil suffered severe withdrawal symptoms. The research team had them taper much more slowly, over an average of nine months and for as long as four years. With this regimen, only 6 percent of subjects experienced withdrawal.
In another study, Dutch researchers in 2018 found that 70 percent of people who’d had trouble giving up Paxil or Effexor quit their prescriptions safely by following an extended tapering regimen, reducing their dosage by smaller and smaller increments, down to one-fortieth of the original amount. This is the regimen recommended in the new paper.
Dr. Horowitz and Dr. Taylor also cited brain-imaging evidence. Antidepressants such as Paxil, Zoloft and Effexor work in part by blocking the serotonin transporter, a molecule that works in the synapses between brain cells to clear out the chemical serotonin, which is thought to help impart a sense of well-being in some people. By blocking the transporter, antidepressants prolong and enhance serotonin’s effects.
But the brain-imaging studies found that inhibition of the transporter increases sharply with addition of the drug and, by extension, also drops sharply with any reduction in dosage. The standard medical advice, to reduce dosage by half — for instance, by taking a pill every other day — and end medication entirely after four weeks, does not take this into account, the two researchers argued.
“Doctors have in mind that these drugs act in a linear way, that when you reduce dosage by half, it reduces the effect in the brain by a half,” Dr. Horowitz said. “It doesn’t work that way. And as a result, there’s a huge load in terms of the effect on brain receptors, and patients are being advised to come off way too quickly.”
Laura Delano, executive director of Inner Compass Initiative, a nonprofit organization that runs The Withdrawal Project and focuses on helping people learn about safer psychiatric drug tapering, said: “I didn’t know about the benefits of slow tapering when I came off five meds in five months, and had a very difficult time in withdrawal.”
The new paper, she added, “speaks to how hard it is to get this information into the clinical world. We laypeople have been saying this for a long time, and it’s telling that it took psychiatrists coming off meds themselves for this information to finally be heard.”
Dr. Horowitz and Dr. Taylor called for more, and more careful, research to be done on withdrawal, to bring their field up to speed, and to develop withdrawal strategies tailored to individual patients and individual drugs.
“I think psychiatrists are taught to learn things from textbooks and from well-conducted studies,” Dr. Horowitz said. “We don’t have many of those for withdrawal, so it makes it hard to believe it’s real. And psychiatrists spend a lot more time prescribing things than stopping them.”
The post How To Quit Antidepressants: Very Slowly, Doctors Say appeared first on Reach Out Recovery.
Fast-Acting Depression Drug, Newly Approved, Could Help Millions
From The New York Times:
A nasal spray version of the drug ketamine has shown promise as an antidepressant, even if its properties still aren’t well understood.
Of the 16 million American adults who live with depression, as many as one-quarter gain little or no benefit from available treatments, whether drugs or talk therapy. They represent perhaps the greatest unmet need in psychiatry. On Tuesday, the Food and Drug Administration approved a prescription treatment intended to help them, a fast-acting drug derived from an old and widely used anesthetic, ketamine.
The move heralds a shift from the Prozac era of antidepressant drugs. The newly approved treatment, called esketamine, is a nasal spray developed by Janssen Pharmaceuticals Inc., a branch of Johnson & Johnson, that will be marketed under the name Spravato. It contains an active portion of the ketamine molecule, whose antidepressant properties are not well understood yet.
“Thank goodness we now have something with a different mechanism of action than previous antidepressants,” said Dr. Erick Turner, a former F.D.A. reviewer and an associate professor of psychiatry at Oregon Health & Science University. “But I’m skeptical of the hype, because in this world it’s like Lucy holding the football for Charlie Brown: Each time we get our hopes up, the football gets pulled away.”
The generic anesthetic is already increasingly available for depression, at hundreds of clinics around the country that provide a course of intravenous treatments, and studies suggest it can help treatment-resistant people. It often causes out-of-body and hallucinogenic sensations when administered; in the 1980s and 1990s it was popular as a club drug, Special K.
The cost for these treatments typically is out of pocket, as the generic anesthetic is not approved by the F.D.A. for depression. In contrast, esketamine likely would be covered under many insurance plans, and its side effects, though similar to those of generic ketamine, are thought to be less dramatic.
The recommended course of the newly approved drug is twice a week, for four weeks, with boosters as needed, along with one of the commonly used oral antidepressants. F.D.A. approval requires that doses be taken in a doctor’s office or clinic, with patients monitored for at least two hours, and their experience entered in a registry; patients should not drive on the day of treatment.
Esketamine, like ketamine, has the potential for abuse, and both drugs can induce psychotic episodes in people who are at high risk for them. The safety monitoring will require doctors to find space for treated patients, which could present a logistical challenge, some psychiatrists said.
The wholesale cost for a course of treatment will be between $2,360 and $3,540, said Janssen, and experts said it will give the company a foothold in the $12 billion global antidepressant market, where most drugs now are generic.
The approval of esketamine marks a new approach to treating serious mood problems, experts said. Prozac and similar drugs enhance the activity of brain messengers such as serotonin; they are mildly effective, but they take weeks or months for their effects to be felt, and for many patients they provide little or no relief from depression. In contrast, the ketamine-based compounds — several others are being developed — work within hours or days, and are effective in some people who are considered “treatment resistant,” meaning they have not benefited from other antidepressants.
“These are exciting times, for sure,” said Dr. Todd Gould, an associate professor of psychiatry in the University of Maryland School of Medicine. “We have drugs that work rapidly to treat a very severe illness.” Dr. Gould was not involved in the Janssen study but has identified a metabolite, or ketamine breakdown product, that could be developed into another drug.
Experts with long experience in treating depression were encouraged by the news, but also chary. The effectiveness of the previous class of antidepressants such as Prozac and Paxil was vastly exaggerated when they came on the market. And the results of esketamine trials, which were paid for and carried out by Janssen, were mixed.
In each trial submitted, all patients were started on a new antidepressant drug, and given a course of esketamine treatment or a placebo. In one monthlong study, those on esketamine performed better statistically than those on placebo, reducing scores on a standard, 60-point depression scale by 21 points, compared to 17 points for placebo. But in two others trials, the drug did not statistically outperform placebo treatment. Historically, the F.D.A. has required that a drug succeed in two short-term trials before it is approved; the agency loosened its criteria for esketamine, opting instead to study relapse in people who did well on the drug.
In that trial, Janssen reported that only about one-quarter of subjects relapsed, compared to 45 percent of subjects who received the placebo spray. All the subjects had been given a diagnosis of treatment-resistant depression, or T.R.D., having previously failed multiple courses of drug treatment.
“We’ve had nothing new in 30 years,” said Steven Hollon, a professor of psychiatry and behavior sciences at Vanderbilt University. “So if this drug is an effective way to get a more rapid response in people who are treatment resistant, and we can use it safely, then it could be a godsend.”
Desperate for relief
One question that will need to be answered is how well esketamine performs in comparison to intravenous ketamine.
Theresa, 57, an adjunct professor of English in New York, who asked that her last name be omitted to protect her privacy, has lived much of her life with deep depression. She tried a course of I.V. generic ketamine last summer, at a local clinic, which typically entails a half-dozen infusions, given over a couple of weeks, for about $500 apiece, with follow-up “booster” treatments as needed.
“I remember floating, I was really high,” she said. “I was tripping on sounds, textures and shapes, that was very much a part of it.”
The first infusion provided no relief, she said. But after the third or fourth, she noticed a satisfying “shift” in her underlying mood. “It’s a hard thing to describe. I was still anxious, but I felt somehow more solid, like something gelled within me, and my husband has noticed it, too.”
Dr. Glen Brooks, the founder and medical director of NY Ketamine Infusions, a clinic in downtown Manhattan, said he has treated some 2,300 people, of all ages, with intravenous ketamine, the generic anesthetic. His clients had received a variety of diagnoses, including post-traumatic stress, anxiety, and obsessive-compulsive disorder, as well as depression.
“What they all have in common is that other medications have failed,” Dr. Brooks, an anesthesiologist, said. “They’re hopeless, and they think, ‘Nothing else has worked, why should this?’” He said that, in his experience, the infusions quickly reduced symptoms for teenagers and young adults, but seemed to be less effective for people over 50.
The data that Janssen presented to the F.D.A. likewise suggested that esketamine was less effective in people aged 65 and older, barely better than placebo treatment.
Ketamine was developed more than five decades ago as a safer alternative to the anesthetic phencyclidine, or PCP, and is used worldwide, in operating rooms, on the battlefield and in pediatric clinics. The World Health Organization has listed ketamine as one of its essential medicines since 1985.
By the 1990s, interest turned to the drug’s potential to combat depression, when a government scientist named Phil Skolnick argued that targeting glutamate pathways — the primary “excitatory,” or neuroactivating, brain processes — could produce antidepressant effects. In 2000, a team of researchers at Yale University and the Connecticut Mental Health Center, led by Dr. Robert M. Berman, reported that doses of ketamine provided quick relief to seven people with depression.
The field took off in 2006, when a team at the National Institute of Mental Health led by Dr. Carlos Zarate Jr. reported that 18 treatment-resistant people who received the drug intravenously reported that their despair lifted within hours.
“What seems remarkable is that the drug also seems to help domains other than depression, like anxiety, suicidal thinking, and anhedonia” — the inability to feel pleasure — said Dr. Zarate, chief of the N.I.M.H.’s experimental therapeutics and pathophysiology branch. “It seems to have more broad effects, on many areas of mood.”
The apparent ability of ketamine to blunt suicidal thinking is particularly compelling, and Janssen is pursuing this indication for esketamine. In jails and psychiatry wards, suicide is an acute risk for people in crisis, and a fast-acting drug could save many lives, doctors said.
For now, no one knows whether esketamine, or any of the other ketamine-based compounds being studied, are any more effective than the generic anesthetic itself — or, for that matter, whether the out-of-body and hallucinatory “side effects” are in fact integral to its antidepressant properties.
“For that, we will need head-to-head studies,” Dr. Zarate said. “And we don’t have those yet.”
The post Fast-Acting Depression Drug, Newly Approved, Could Help Millions appeared first on Reach Out Recovery.
What Does an Anxiety Disorder Feel Like? Here Are 4 Signs You May Have a Problem
From Jeffery Kluger @ Time: If 2.6 billion people were suffering from an illness, you’d think we’d all be more familiar with it. That figure represents 33.7% of the population of the world, after all. It also represents the share of that population that will at some point experience an anxiety disorder, according to the National Institutes of Health.
For those billions, the experience of clinical anxiety can range from a persistent fretfulness, distractedness and a sort of whole-body clenching, to the paralytic crisis of a full-blown panic attack. All of it feels lousy; all of it is a state you race to escape — which typically only makes it worse. But all of it, happily, is diagnosable, controllable and ultimately treatable. The key is recognizing if your anxiety rises to the level of a clinical condition, and if it does, what to do about it.
Anxiety may, by definition, feel bad, but that doesn’t mean it therefore is bad. It’s a menacing world out there, and your brain needs a way to grab your attention when you’re stumbling into danger. The job of doing that is actually handled by two brain regions: the amygdala, situated deep in the brain’s basement, and the higher, more complex cerebral cortex.
As befits its humble location, the amygdala processes very basic emotions — fear, anger, guilt, envy — and handles them quickly and unthinkingly. The fear you experience from a menacing stranger and the fear you experience from a scary movie set off the same amygdala alarms, and do it within 20 milliseconds — a very good thing if the danger is real. The job of determining whether it is or not goes to the cerebral cortex, which sorts things through more coolly and either responds to the threat or shuts down the siren the amygdala has set off.
Sometimes, however, the alarm gets stuck. The cerebral cortex can get flummoxed trying to sort real risks from exaggerated ones: Doorknobs do carry germs, so how do you know the one you touched didn’t have something deadly? People do suffer social humiliation at parties or while giving speeches; how do you know you won’t be one of them?
The most common recognized anxiety disorders include general anxiety disorder, agoraphobia (or fear of being in public situations you can’t escape), social anxiety disorder, post-traumatic stress disorder (PTSD), specific phobias, obsessive compulsive disorder (OCD) and separation anxiety disorder. There is no blood test or brain scan that can conclusively diagnose any of them, but here are four signs that may point to trouble.
You Have A High Level Of Distress
Anxiety is a question of degree. It’s one thing to be jittery before an important test or presentation or to worry about your health when an epidemic is in the news. And if you have a particular sensitivity — flying, dentists, working the room at a crowded party — you’re going to be tense as one of those situations approaches. If the tension consumes your day, however, if it crowds out other thoughts or if the psychic pain goes from troubling to severe, that’s another matter.
“Anxiety will prevent people from sleeping; they’ll find themselves crying over it,” says psychologist Golda Ginsburg, professor of psychiatry at the University of Connecticut School of Medicine and a specialist in child and adolescent mental health. “There are students who will vomit in the days leading up to a test.”
In some cases, the emotions become so severe they lead to a panic attack, a sort of weaponized anxiety that hits fast and hard and includes such symptoms as dizziness, rapid heart rate, depersonalization or out-of-body experience and a fear of losing control or dying. “If you suddenly have to slam on your brakes and swerve to avoid a collision, that pounding heart and rapid breath you feel for a few minutes after is a form of panic attack,” says psychologist Anna Albano, director of Columbia University’s Clinic for Anxiety and Related Disorders. “In the context of a disorder, however, you might start to feel the same thing the moment you walk into the office or a party.”
Your Panic Is Persistent
An anxious brain, like a non-anxious brain, is always learning. But the anxious brain sometimes learns the wrong things and has an awfully hard time unlearning them. Once you’ve decided that people at parties are probably judging you, your brain may lock that lesson in and pretty soon generalize it to any social encounter. Ditto an obsessive-compulsive fear of disease or a panic over separation or loss. Sometimes, especially in the case of OCD, it takes just a single traumatic event — a genuinely embarrassing social moment, say, or a legitimate medical scare — for the brain to establish a fixed fear. Left untreated, those anxieties can go on for months and years.
You Avoid Things Because Of Your Fears
We all avoid things we fear or dislike: you could go your whole life without roller coasters or cilantro or horror movies. But they don’t really affect your life. Anxieties start to strip away the things that do. “You may dread getting a medical test because of what you could learn,” says Albano. “But if you’re avoiding going to your doctor at all because of it, that’s a problem.”
People with an airplane phobia may, similarly, limit their travel to only places they can drive. People with big dreams may sometimes settle for smaller ones because their anxiety holds them back. “I know people who went to law school and wanted to pursue a career in criminal law but were afraid to be in front of a courtroom,” says Albano. “So they push documents in a law firm instead.”
Your Worries Interfere With Day-To-Day Life
Ultimately, an anxiety disorder may become so severe that the basic business of living becomes compromised. People suffering from OCD may need hours to get out of the house in the morning because the pillows on the bed aren’t arranged properly. Schoolwork and job performance may suffer because perfectionism makes it impossible to complete a project or because social anxiety makes it impossible to talk to classmates or colleagues. Things become worse when emotional symptoms lead to physical ones such as headaches, loss of appetite and sleeplessness. “The question I ask first is, ‘Is your anxiety impairing your functioning?’” says Goldberg.
Anxiety responds well to professional care. Treatment may include psychotropic medications like Zoloft or Prozac, which can at least lower the voltage of the pain. That may make it easier to embrace and practice the techniques of cognitive behavioral therapy, in which people learn to talk back to their anxiety, reframe their fears to something less extreme, and practice self-soothing techniques like mindfulness or distraction or breathing. Slow, graduated exposure to the very things people fear also helps the brain break the link between the trigger situation and the terror that follows.
No one can live a life untouched by anxiety. But with the right skills and the right help, no one needs to live one that is destroyed by it, either.
The post What Does an Anxiety Disorder Feel Like? Here Are 4 Signs You May Have a Problem appeared first on Reach Out Recovery.
When Cyber Bullying Turns Into Abuse
When do those stinging negative comments cross the line from a form of cyber bullying into abusive and hurtful attacks? After movements like #metoo and #sorrynotsorry, we might expect a kinder, safer world. Unfortunately, unkindness is alive and well. Many of today’s cyber bullying are abusive and include mansplaining, misogyny, trolling and defamation. Recovery gives us tools to cope.
Negative Comments Turn Into Cyber Bullying
Holly runs an inner-city bakery, and she raises money to help feed the homeless. On her bakery’s website, people can pre-order cakes and view her menu. She also has a blog where she shares recipes and occasionally writes about issues related to homelessness. Last month, her work with the homeless was featured in the local newspaper.
Of course, not everyone agrees on how to help homeless people. “Steve” is one such reader. He is furious with Holly, so he posted this retort about the newspaper’s article as a review of Holly’s bakery.
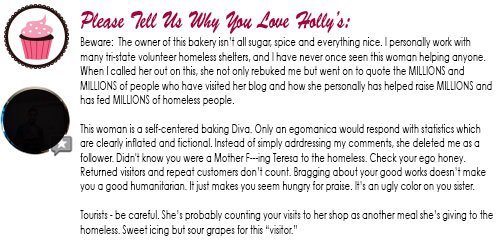
This is more than just a simple dissatisfied customer. This is cyber bullying. When we dissect Steve’s comment, we see he actually used four common tactics to attack Holly. The first of which is mansplaining.
What Is Mansplaining?
According to Miriam-Webster, mansplaining:
“Occurs when a man talks condescendingly to someone (especially a woman) about something he has incomplete knowledge of, with the mistaken assumption that he knows more about it than the person he’s talking to does.”
Here’s an example of mansplaining in action.
These sentences are examples of mansplaining because he, the reviewer, is not privy to the Holly’s statistics. Yet he thinks he knows more about her business, volunteer work and how to quantify them than she does. When you attack from ignorance your purpose is to hurt.
What Is Misogyny?
Per dictionary.com, misogyny is, “hatred, dislike, or mistrust of women, or prejudice against women.” In this example, the comments attack based on gender. He uses terms of endearment like “sister” and “honey” to insult.
This is a case of misogyny because the writer is a man and the target is a woman. If they were both of the same gender, we would still be looking at a patronizing case of intimidation.
What Is Trolling?
Wikipedia defines trolling as,
“A person who starts quarrels or upsets people on the Internet to distract and sow discord by posting inflammatory and digressive, extraneous, or off-topic messages in an online community (such as a newsgroup, forum, chat room, or blog) with the intent of provoking readers into displaying emotional responses and normalizing tangential discussion, whether for the troll’s amusement or a specific gain.”
Going back to our example, this entire review is an example of trolling. It’s off-topic because Steve’s concerns with Holly have nothing to do with her business or website. His anger is in response to an article published in an independent newspaper.
What Is Defamation?
Defamation is when a false statement is presented as fact to a third party. According to Legal Zoom,
“The difference between defamation and slander is that a defamatory statement can be made in any medium. It could be in a blog comment or spoken in a speech or said on television. Libelous acts only occur when a statement is made in writing (digital statements count as writing) and slanderous statements are only made orally.”
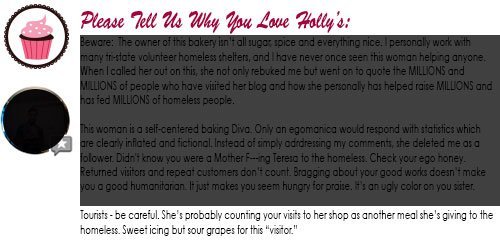
The comments in our example are in writing and nonfactual. Holly does not consider her paying customers to be homeless people. Steve’s scathing review is clearly meant to harm Holly’s business and livelihood. Therefore, this is a libelous act.
How To Respond?
Here’s why recovery is a game changer. Recovery teaches us so much more than how to be sober or quit using. Recovery shows us that we do have value, and recovery teaches us how to communicate even in difficult situations like cyber complaints.
To Stop Cyber Bullying, First, We Tell Someone
Abuse only survives in secrecy.
In this example, the writer wants to intimidate and silence. We often see this in family dysfunction as well. Families in crisis operate under three specific rules: Don’t talk, don’t trust, and don’t feel.
To get over such insults, we talk to someone we trust. Maybe it’s a sponsor or a counselor. We do not allow ourselves to be isolated. This only makes us more vulnerable to escalating cyber complaints.
After Sharing We Hit The Pause Button
Inflammatory responses do not require immediate reaction. It’s important to give yourself time to process your emotions and brainstorm with accountability partners.
We Use Social Media Tools To Protect Ourselves
Many social media accounts allow you to ban angry followers. You can also report harassing and inappropriate comments. Some defamation cases might require legal action.
What Can We Change
Finally, we change what we can. We cannot control bullies and trolls. At the end of the day, we can only change ourselves. We can’t stop someone from being mean or even lying about us in private or public. We do, however, have the ability to take action to protect our character, livelihood, and mental well-being.
The post When Cyber Bullying Turns Into Abuse appeared first on Reach Out Recovery.
6 Ways To Stand Up For Yourself
From Catherine Saint Louis @ The New York Times: No one sets out to be a doormat. Yet some people are chronically passive, always putting other’s needs before their own. These are the folks who end up babysitting for an acquaintance instead of going to their yoga class. In the long run, being unable to express what you want is a recipe for perpetual dissatisfaction, because your needs always end up on the back burner. The good news is people can learn to ask for the things they want at home, at work and even at a local restaurant when you get a burnt steak and want a new one.
Be Assertive, Not Aggressive
All of us have said yes to a commitment or task we didn’t really want to do. How many of us have rented a tux or bought a bridesmaid’s dress we couldn’t afford, and flown to be part of a wedding we didn’t really want to attend?
In the moment, unassertive behavior has certain perks. After all, dropping your plans to help a relative or disorganized boss means not only avoiding conflict but also avoiding letting anyone down. You get to be the hero!
But over time, being unable to express what you want is a recipe for perpetual dissatisfaction, because your needs always end up on the back burner.
Assertiveness Is The Answer
Excessively-agreeable types aren’t the only ones who can benefit from learning to be assertive. Overly hostile people benefit, too.
Aggressiveness is sometimes mistaken for assertiveness but they are different. It’s one thing to stand up for yourself, and quite another to bully others to get your way.
Here’s the difference between aggression and assertiveness. When there’s a difference of opinion, a hostile, aggressive boss may lose her temper in a meeting or resort to calling underlings names to end the discussion. But assertive people can stand up for themselves without tearing down anyone else. They might say, “I can see why your proposal has benefits, but here’s how I think we should proceed.”
Randy J. Paterson, a psychologist who wrote “The Assertiveness Workbook,” explained that “If you take an aggressive posture, you’re allowed on stage and your mission is to get everyone else off.” By contrast, assertive people are collegial thespians who don’t mind sharing the stage. They can be cordial even as they express an unpopular opinion.
In short, assertiveness is not a license to be rude, says Robert Alberti, a renowned psychologist who co-authored the seminal 1970s book about assertiveness: “Your Perfect Right.” The aim of the book, co-authored with Michael Emmons, a psychologist, was to teach people to express themselves while being respectful to others. They wrote: “Equality is fundamental to assertive living.”
How to Be Assertive
There are a number of ways assertiveness plays out. (And it can take practice.)
Assertiveness is a skill. It entails multiple abilities, not only being able to say no. Assertive people can also express negative feedback; they can make their needs known; and importantly, they can stand up for themselves in a way that doesn’t denigrate others.
Not sure how to be assertive? It takes some training, but you can learn how to express your thoughts comfortably without feeling unduly anxious. Here’s some things to try:
1. Be Brief
Julie de Azevedo Hanks, a Utah psychotherapist, likes to remind herself that “No is a complete sentence.” You are not obligated to explain at length to a friend or stranger why you’d prefer not to do something. (A boss may require more rationale, but a succinct answer is still best.)
2. Be Gracious In Declining An Invitation
Dr. Hanks, author of “The Assertiveness Guide for Women,” said that if she is asked to return as a speaker at a conference for a second year and she doesn’t want to go, she may say, “I’m glad it went well last year, but this year is no good.”
3. Use “I” Phrases
If a co-worker expects prompt answers to their Saturday night missives, inform them on Friday: “I need uninterrupted downtime this weekend so I’m not checking mail until Monday.” By contrast, “you” phrases sound accusatory and tend to backfire, as any spouse knows.
4. Stall
If you’re indecisive or need a moment to consider a request, use a delay tactic, Dr. Paterson advises. Say: “Let me check my schedule and get back to you.” No more knee-jerk “Yes’s”.
5. Prepare Responses
For repeat askers in your life, decide beforehand what requests are unreasonable and then formulate a “pleasant but firm” answer, Dr. Paterson said. For instance, if your mother wants you to paint her bathroom this weekend, you may decide you’re not willing to do it, even though you’ve long been her go-to painter. One way to go: “I don’t have time in my schedule to tackle this anytime soon, but I’m happy to send you a few names of reliable painters.”
6. Act It Out
It might seem silly, but rehearsing certain scenarios in front of the mirror or role playing with a trusted friend can help. Practice sounding relaxed, even if you aren’t.
Gut Check: Are You A Doormat?
Still not sure if you are saying yes too often to other’s requests? Ask yourself the following questions the next time you do something for someone else:
Am I Secretly Enraged?
One tell-tale sign that you may be too passive is having simmering rage that you keep to yourself. Anger is not just for aggressive people, Dr. Paterson explained. If you find yourself thinking that the world is populated with inconsiderate idiots who constantly ask you to do stuff and don’t appreciate your efforts, perhaps you are quietly seething, he said. Another sign is feeling like you’re a boiler with pressure building up.
Do I Give, Give, Give, With No Take?
Lisa M. Schab, a licensed clinical social worker in Libertyville, Ill., said her passive clients have a common complaint. “I did all this for them, and they do nothing for me.” If you are so generous that you are chronically resentful and drained, you may be overdoing it, she said. Healthy relationships are balanced, with give and take.
Is Your Body Language Telling You Something?
In their book, “Your Perfect Right,” Dr. Alberti and Dr. Emmons explained that people who look down and can’t make eye contact, even to a person they’re speaking to, come off as deferential and sheepish. At Starbucks, do you whisper when you order a latte? At a cocktail party, do you approach strangers with so much trepidation your body transforms into what the authors call a ‘Please don’t hurt me’ posture? You may be a pushover.
The post 6 Ways To Stand Up For Yourself appeared first on Reach Out Recovery.
Marijuana In Massachusetts Making Dogs Sick
From Brett Gubitosi @ New York Post: According to the Cape Cod Times, dogs are finding and ingesting marijuana on the Massachusetts peninsula, leaving owners concerned and vets overworked.
“It’s a rare day that we don’t have a ‘pot dog’ hospitalized in the ICU,” said Dr. Louisa Rahilly, medical director of Cape Cod Veterinary Specialists.
Dog owner Linda McCann said her minipoodle Brahms became “so stoned” after he ate a blunt lying in a parking lot during their morning walk.
“He usually barks at neighbors, greets people and the highlight of his day is getting a treat from the mailman,” said McCann following the incident. “But he didn’t move. His eyes were so dilated.”
Rahilly said the doped dogs don’t take cannabis well, leaving them “vomiting and urinating,” which could be mistaken for a stroke.
Another telltale sign of high dogs is their “drunken gait,” Rahilly noted.
Dogs who digest pot are expected to recover in 12 to 24 hours, according to Kevin Smith, co-owner of the Hyannis Animal Hospital.
“Similar to a person, if they ate too much edibles, it would be a bad 24 hours,” he said.
The American Society for the Prevention of Cruelty to Animals stated that the number of weed-related calls in 2018 totaled 1,800 — compared to 208 a decade ago.
The sale of recreational marijuana in Massachusetts was legalized on Nov. 20, 2018. McCann did not respond to The Post for comments.
The post Marijuana In Massachusetts Making Dogs Sick appeared first on Reach Out Recovery.
March 4, 2019
What Is A Living Amends?
When I first came to recovery, I was certain steps 8 and 9 would be a breeze. After all, I hadn’t hurt anyone (Step 8), so I didn’t need to make any amends (Step 9). I was wrong. So wrong. In fact, every day I make a living amends to my husband, son, Mom, and brother Ricky. Here’s how it works for me.
The List Of Wrongs
In Step 4, I took a “fearless and moral” inventory of my past. I made a list of everything I resented. I thought this was the part where I got to dump all of my anger on the people who abused me. It wasn’t. Instead, my inventory was an:
Examination of the part I played in past hurts
Unearthing of patterns where I repeated volunteered myself for abuse and manipulation
Analysis of my motives – almost all of my decisions were based on fear – I tried to control everyone around me to feel safe
Turns out, I was a bossy control freak who was terrified of everything. I was pushy and overbearing. I had all the answers, and I shared them with everyone. When they didn’t follow my advice, I let them know – repeatedly. When they had the nerve to do things their own way, I reminded them that I had first suggested a better plan. Yikes.
Three Ways I Make A Living Amends
My husband and son bore the brunt of my controlling behavior, so these days I work really hard at letting them do things their way using these three tactics.
1. I Keep My Mouth Shut
When my husband misses a turn because he’s in the wrong lane, I say nothing. When he runs out of medicine because he didn’t call the doctor for a refill, I trust he has the intelligence to solve his own problem. And I keep my mouth shut. When he handles a situation at work “the wrong way” I keep my opinion to myself.
For my son, I also took a big step back. He’s a teenager, so I try to let him function at that age level. I taught him how to do his own laundry. When he runs out of clean clothes, I don’t lecture or offer solutions. I let him decide if he wants to do laundry at midnight or wear dirty clothes. I no longer interrogate him about his day at school, so I can give my wise advice on how to handle difficult peers. If he doesn’t want to do his homework, I say nothing. It’s none of my business. I’m not his teacher, and I’m sure she’s skilled at handling that type of problem.
I applied the same hands off, lips sealed policy to my Mom and my brother Ricky. They are enmeshed in a toxic, symbiotic relationship. Instead of yin and yang, they are dependent and codependent.
My living amends to Ricky is simple. I don’t call him to see how his meeting went this week or what step he’s on. Nor do I play the peacemaker between him and our Mother. I let him live his life, and I live mine. If he specifically asks for my opinion, which he doesn’t, I will give it.
My Mom, on the other hand, loves to complain about Ricky’s behavior. Sometimes I can listen supportively for a short period of time. When she takes a breath, I ask if she wants my opinion. If she does, I say it once. If not, I change the subject. Over the years, in small bits and pieces, I have been able to share small pearls of my Al-anon wisdom.
2. I Give Them A PANDA
Another tool I love to use is a PANDA apology. Nicole Gehl over at Your Tango explains that PANDA stands for:
P: Promise it will never happen again
A: Admit you were at fault
N: No excuses
D. Describe how you would handle the situation next time
A. Act on your promise
After years of being bossy and overbearing, my basic apologies meant little. My living amends represents the last A in PANDA. I am determined to let my loved ones be independent. They don’t always see my hands off approach as sincere kindness, but my motives are pure. I’m doing what I think is best for all of us.
3. If I Must Say It, I Only Say It Once
Ninety percent of the time, I keep my mouth shut, but I am my son’s mother. I have a responsibility to parent him and speak out for his best interests. Likewise, my marriage is a partnership with my husband. I have an equal voice. Sometimes, my opinion is required. Early in my recovery, I learned neither my son nor my husband was listening to anything I said. So I said it again and again and again. Thus, I was a nagger.
Today, I know my words have value whether they pay attention or not. When it matters, I say something once. If they didn’t pay attention, I do my best to let them suffer the consequence. If they take my words for granted, sometimes, I take a break from talking. I don’t punish them with silence (although I did do that in the past). I write out really important things. They usually hear those messages loud and clear.
All of these tools have slowly brought more peace to my home. One final thought: watching my loved ones suffer any type of pain is a trigger for me. I want to rush in and save them. Sometimes, I need to take a time out in my bedroom with my door shut. This gives them freedom to do what they think is best, and I get to keep my serenity.
The post What Is A Living Amends? appeared first on Reach Out Recovery.
Kristin Davis On Sobriety And SATC
From Justine Browning @ Entertainment Weekly: Kristin Davis believes without her turn on Sex and the City, she likely wouldn’t be alive today.
The actress, who starred as Charlotte York for six seasons on the landmark HBO series, looked back at her time on the show during an interview with the podcast Origins With James Andrew Miller and revealed her early career success helped her to overcome alcohol addiction.
“I don’t think I would be alive,” she shared. “I’m an addict. I’m a recovering alcoholic. If I hadn’t found acting…acting is the only thing that made me want to ever get sober. I didn’t have anything that was that important to me other than trying to dull my senses.”
Davis, now 53, once feared her struggle would mean she wouldn’t live to see 30, but being part of a major production led her down the path of sobriety.
“I didn’t think I would live to be 30,” she said. “I started drinking very young and luckily I quit very young, before any success happened, thank goodness.”
She adds, “Because my love for acting was so big when I was very young, I had something that was more important to me than just drinking.”
The comedy, which helped kick off the golden age of TV prior to the release of The Sopranos and The Wire, aired its final episode in 2004 and later spawned two films —Sex and the City: The Movie (2008) and Sex and the City 2 (2010).
The Origins podcast episode “Tutu’s, Tete-a-Tete’s, and Taxi’s” also features interviews with cast members Sarah Jessica Parker, Cynthia Nixon, and Chris Noth.
The post Kristin Davis On Sobriety And SATC appeared first on Reach Out Recovery.


