
Nelson Vergel's Blog, page 7
July 20, 2012
Toxic Hepatitis In A Group Of Twenty Male BodyBuilders Taking Dietary Supplements
Hariri AT, Mood MB, Aryan E, Sadeghi M, Zanjani BR. Toxic hepatitis in a group of twenty male body-builders taking dietary supplements. Food Chem Toxicol. http://www.sciencedirect.com/science/article/pii/S027869151200484X
Dietary supplements have been used for decades for enhancing muscle growth. The harm caused by some of these products is well documented. We investigated and reported toxic hepatitis in 20 male athletes following self-prescribing of a number of dietary supplements which are lesser known. The patients' ages ranged from 24 to 32 with a mean of 28 years.
They had taken three kinds of supplements for one year including testosterone optimizer agent T Bomb II, a creatine supplement Phosphagen and an amino acid based supplement Cell-Tech. Based on the history, clinical examination, and laboratory findings the cases were diagnosed as toxic hepatitis. After discontinuation of taking the supplements, clinical recovery and improvement of liver function tests were achieved within 30 days.
Causality assessment with the CIOMS (Council for International Organization Medical Sciences) scale showed a "possible" grade of causality (+5 points) for these supplements. It can be concluded that these newer anabolic supplements may induce toxic hepatitis. Since the health risks of them may be severe, the use of these kinds of dietary supplements should be discouraged.



July 16, 2012
Free Testosterone Booklet- Boost Your Physical, Mental and Sexual Vitality
Use this link to download a free 14 page booklet on testosterone
Testosterone Benefits and Potential Side Effects-
Testosterone Benefits and Potential Side Effects-
July 7, 2012
Selective Androgen Receptor Modulators- Future Agents for Aging Related Muscle Loss
Oral selective androgen receptor modulators (SARMs) are investigational agents. Studied since 1998, they are still very much in the infancy of their development and marketing. SARMs may be able to provide the benefits of increased muscle mass and bone density, and fat loss that testosterone and other traditional anabolic/androgenicsteroids provide but without the unwanted side effects (prostatic enlargement). SARMs are not intended to be a form of testosterone replacement therapy. So, why am I talking about them?
More information:
Selective Androgen Receptor Modulators
More information:
Selective Androgen Receptor Modulators
July 3, 2012
How Long Does It Take for Testosterone to Work?
Objectives: Testosterone has a spectrum of effects on the male organism. This review attempts to determine, from published studies, the time-course of the effects induced by testosterone replacement therapy from their first manifestation until maximum effects are attained.Design: Studies in PubMed on testosterone replacement so far providing information on time course.Results: Effects on sexual interest appear after 3 weeks plateauing at 6 weeks, no further increments beyond. Changes in erections/ejaculations may require up to 6 months. Effects on quality of life manifest within 3-4 weeks, but maximum benefits take longer. Effects on depressive mood appear after 3-6 weeks with a maximum after 18-30 weeks. First effects on erythropoiesis (increased red blood cells) after 3 months, peaking at 9-12 months. Prostate specific antigen and volume rise, marginally, plateauing at 12 months; further increase related to aging rather than therapy. Effects on lipids appear after 4 weeks, maximal after 6-12 months. Insulin sensitivity may improve within few days, but effects on glycemic control become evident only after 3-12 months. Changes in fat mass, lean body mass and muscle strength occur within 12-16 weeks, stabilize at 6-12 months, but marginally continue to improve over years. Effects on inflammation occur within 3 to 12 weeks. Effects on bone detectable after 6 months but continue at least for 3 years.Conclusion: the time-course of the spectrum of effects of testosterone shows considerable variation, probably related to pharmacodynamics of the testosterone preparation. Genomic and non-genomic effects, androgen receptor polymorphism and intracellular steroid metabolism further contribute to such diversity.
Source: http://www.eje-online.org/content/early/2011/07/13/EJE-11-0221.abstract

July 2, 2012
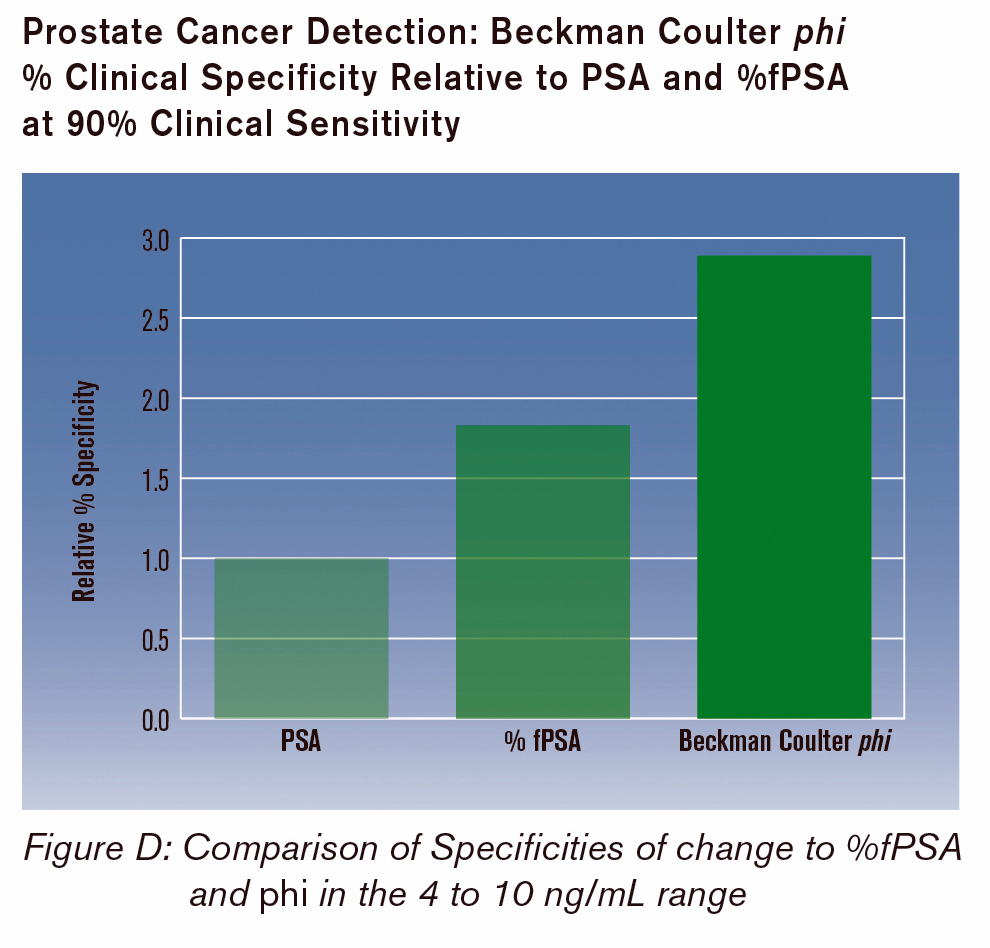
FDA OKs New Prostate Cancer Blood Test

A blood test for prostate cancer billed by its manufacturer as "an answer to the current PSA [prostate-specific antigen] testing controversy" has won FDA approval, the company said.Beckman Coulter said Monday that the agency had okayed its premarket approval application for the so-called Prostate Health Index test, which incorporates measurement of a PSA precursor protein called [-2] pro-PSA along with total and free PSA.The test is indicated for men with regular PSA test results in the range of 4ng/mL to 10 ng/mL, just above the upper limit of normal.According to the co-discoverer of [-2] pro-PSA, Kevin Slawin, MD, of Memorial Hermann-Texas Medical Center in Houston, the marker is more closely associated with prostate cancer than total and free PSA. Combining the three markers makes the Prostate Health Index more specific than conventional PSA testing.
More: http://www.medpagetoday.com/HematologyOncology/ProstateCancer/33486
Beckman Coulter Prostate Health Index

June 27, 2012
High Calorie Breakfast Helped People Lose More Weight than a High Calorie Dinner
Comparison of the Effect of High Calorie Breakfast Diet vs High Calorie Dinner Diet on Weight Loss
[SUN-LB3] Comparison of the Effect of High Calorie Breakfast Diet vs High Calorie Dinner Diet on Weight Loss, Ghrelin, Lipids and Appetite Scores in Obese Non Diabetic Women
http://www.abstracts2view.com/endo/view.php?nu=ENDO12L_SUN-LB3
Daniela Jakubowicz, Mona Boaz, Yosepha Bar-Dayan, Julio Wainstein. Tel Aviv University, Holon, Israel; Tel Aviv University, Holon, Israel.
Background: Recently we have shown that compared to low carbohydrate (CH) diet, an isocaloric diet with addition of high calorie breakfast (B) that also included dessert, promoted sustained weight(W) loss(WL) and prevented W regain by reducing diet-induced compensatory changes in hunger, cravings and ghrelin suppression. Direct effects of meal timing (morning vs. evening increased calories) were not tested.
Objective: To search whether a change in meal timing by increasing calories in the morning vs in the evening has a differential impact on WL, ghrelin suppression, lipids and appetite scores. Our hypothesis is that comparing with high calorie dinner (D) + reduced B (HCDd), the high calorie B + reduced D (HCBd), would enhance WL, ghrelin suppression and appetite scores.
Methods: 73 obese women (BMI 32.3±2.0 kg/m2), aged 46±6 years, were randomized to two isocaloric (1400 kcal) weight loss diets during 12 weeks (Wk). Both diets had the same composition but differ in the meal timing distribution
1)HCBd consisted in large B with 700 Kcal(Kc)with % of CH; protein; fat: 50:30:20%; lunch (500 Kc, 20:45:25%), and small D (200 Kc, 13:40:47%).
2)HCDd consisted in low calorie B (200 Kc, 13:40:47%),lunch(500 Kc, 20:45:25%), and large D (700 Kc, 50:30:20%).
Anthropometric measures were assessed every 4Wk. Fasting glucose, insulin, ghrelin, lipids, OGTT, craving scores as well as B and D challenge were performed at baseline and at Wk12
Results: After Wk12 intervention, the HCBd group (g) lost 8.7±1.4 kg vs 3.48±2.3 kg the HCDd g. In comparison to the HCDd g, the HCBd g showed 61% greater WL, P<0.05,a 35% greater reduction in waist circumference (P<0.06) and a 17% greater reduction in percent body fat (P=NS). Ghrelin levels were reduced after B by 46.2% in the HCBd group and 18.5% after D in the HCDd g(P>0.005). Satiety was significantly improved and hunger and craving scores significantly reduced in the HCBd vs HCDd g (P>0.005). Mean serum triglyceride levels decrease by 44% (from 184.2±16.6 to 102.2±7.7 mg/dl) in the HCBd g while increase 6.3% (from 180.5±20.6 to 192.4±17.5 mg/dl) in the HCDd g(P>0.005). Total cholesterol (C), HDL-C and LDL-C, did not differ between the groups.
Conclusion: Isocaloric WL diets with different meal timing, differently influence WL rate, ghrelin, appetite and lipid levels. HCBd with reduced intake at D result in enhanced WL, increased ghrelin suppression and might be useful alternative for management of obesity.

[SUN-LB3] Comparison of the Effect of High Calorie Breakfast Diet vs High Calorie Dinner Diet on Weight Loss, Ghrelin, Lipids and Appetite Scores in Obese Non Diabetic Women
http://www.abstracts2view.com/endo/view.php?nu=ENDO12L_SUN-LB3
Daniela Jakubowicz, Mona Boaz, Yosepha Bar-Dayan, Julio Wainstein. Tel Aviv University, Holon, Israel; Tel Aviv University, Holon, Israel.
Background: Recently we have shown that compared to low carbohydrate (CH) diet, an isocaloric diet with addition of high calorie breakfast (B) that also included dessert, promoted sustained weight(W) loss(WL) and prevented W regain by reducing diet-induced compensatory changes in hunger, cravings and ghrelin suppression. Direct effects of meal timing (morning vs. evening increased calories) were not tested.
Objective: To search whether a change in meal timing by increasing calories in the morning vs in the evening has a differential impact on WL, ghrelin suppression, lipids and appetite scores. Our hypothesis is that comparing with high calorie dinner (D) + reduced B (HCDd), the high calorie B + reduced D (HCBd), would enhance WL, ghrelin suppression and appetite scores.
Methods: 73 obese women (BMI 32.3±2.0 kg/m2), aged 46±6 years, were randomized to two isocaloric (1400 kcal) weight loss diets during 12 weeks (Wk). Both diets had the same composition but differ in the meal timing distribution
1)HCBd consisted in large B with 700 Kcal(Kc)with % of CH; protein; fat: 50:30:20%; lunch (500 Kc, 20:45:25%), and small D (200 Kc, 13:40:47%).
2)HCDd consisted in low calorie B (200 Kc, 13:40:47%),lunch(500 Kc, 20:45:25%), and large D (700 Kc, 50:30:20%).
Anthropometric measures were assessed every 4Wk. Fasting glucose, insulin, ghrelin, lipids, OGTT, craving scores as well as B and D challenge were performed at baseline and at Wk12
Results: After Wk12 intervention, the HCBd group (g) lost 8.7±1.4 kg vs 3.48±2.3 kg the HCDd g. In comparison to the HCDd g, the HCBd g showed 61% greater WL, P<0.05,a 35% greater reduction in waist circumference (P<0.06) and a 17% greater reduction in percent body fat (P=NS). Ghrelin levels were reduced after B by 46.2% in the HCBd group and 18.5% after D in the HCDd g(P>0.005). Satiety was significantly improved and hunger and craving scores significantly reduced in the HCBd vs HCDd g (P>0.005). Mean serum triglyceride levels decrease by 44% (from 184.2±16.6 to 102.2±7.7 mg/dl) in the HCBd g while increase 6.3% (from 180.5±20.6 to 192.4±17.5 mg/dl) in the HCDd g(P>0.005). Total cholesterol (C), HDL-C and LDL-C, did not differ between the groups.
Conclusion: Isocaloric WL diets with different meal timing, differently influence WL rate, ghrelin, appetite and lipid levels. HCBd with reduced intake at D result in enhanced WL, increased ghrelin suppression and might be useful alternative for management of obesity.
HIgh Calory Breakfast Helped People Lose More Weight than a High Calorie Dinner
Comparison of the Effect of High Calorie Breakfast Diet vs High Calorie Dinner Diet on Weight Loss
[SUN-LB3] Comparison of the Effect of High Calorie Breakfast Diet vs High Calorie Dinner Diet on Weight Loss, Ghrelin, Lipids and Appetite Scores in Obese Non Diabetic Women
http://www.abstracts2view.com/endo/view.php?nu=ENDO12L_SUN-LB3
Daniela Jakubowicz, Mona Boaz, Yosepha Bar-Dayan, Julio Wainstein. Tel Aviv University, Holon, Israel; Tel Aviv University, Holon, Israel.
Background: Recently we have shown that compared to low carbohydrate (CH) diet, an isocaloric diet with addition of high calorie breakfast (B) that also included dessert, promoted sustained weight(W) loss(WL) and prevented W regain by reducing diet-induced compensatory changes in hunger, cravings and ghrelin suppression. Direct effects of meal timing (morning vs. evening increased calories) were not tested.
Objective: To search whether a change in meal timing by increasing calories in the morning vs in the evening has a differential impact on WL, ghrelin suppression, lipids and appetite scores. Our hypothesis is that comparing with high calorie dinner (D) + reduced B (HCDd), the high calorie B + reduced D (HCBd), would enhance WL, ghrelin suppression and appetite scores.
Methods: 73 obese women (BMI 32.3±2.0 kg/m2), aged 46±6 years, were randomized to two isocaloric (1400 kcal) weight loss diets during 12 weeks (Wk). Both diets had the same composition but differ in the meal timing distribution
1)HCBd consisted in large B with 700 Kcal(Kc)with % of CH; protein; fat: 50:30:20%; lunch (500 Kc, 20:45:25%), and small D (200 Kc, 13:40:47%).
2)HCDd consisted in low calorie B (200 Kc, 13:40:47%),lunch(500 Kc, 20:45:25%), and large D (700 Kc, 50:30:20%).
Anthropometric measures were assessed every 4Wk. Fasting glucose, insulin, ghrelin, lipids, OGTT, craving scores as well as B and D challenge were performed at baseline and at Wk12
Results: After Wk12 intervention, the HCBd group (g) lost 8.7±1.4 kg vs 3.48±2.3 kg the HCDd g. In comparison to the HCDd g, the HCBd g showed 61% greater WL, P<0.05,a 35% greater reduction in waist circumference (P<0.06) and a 17% greater reduction in percent body fat (P=NS). Ghrelin levels were reduced after B by 46.2% in the HCBd group and 18.5% after D in the HCDd g(P>0.005). Satiety was significantly improved and hunger and craving scores significantly reduced in the HCBd vs HCDd g (P>0.005). Mean serum triglyceride levels decrease by 44% (from 184.2±16.6 to 102.2±7.7 mg/dl) in the HCBd g while increase 6.3% (from 180.5±20.6 to 192.4±17.5 mg/dl) in the HCDd g(P>0.005). Total cholesterol (C), HDL-C and LDL-C, did not differ between the groups.
Conclusion: Isocaloric WL diets with different meal timing, differently influence WL rate, ghrelin, appetite and lipid levels. HCBd with reduced intake at D result in enhanced WL, increased ghrelin suppression and might be useful alternative for management of obesity.
[SUN-LB3] Comparison of the Effect of High Calorie Breakfast Diet vs High Calorie Dinner Diet on Weight Loss, Ghrelin, Lipids and Appetite Scores in Obese Non Diabetic Women
http://www.abstracts2view.com/endo/view.php?nu=ENDO12L_SUN-LB3
Daniela Jakubowicz, Mona Boaz, Yosepha Bar-Dayan, Julio Wainstein. Tel Aviv University, Holon, Israel; Tel Aviv University, Holon, Israel.
Background: Recently we have shown that compared to low carbohydrate (CH) diet, an isocaloric diet with addition of high calorie breakfast (B) that also included dessert, promoted sustained weight(W) loss(WL) and prevented W regain by reducing diet-induced compensatory changes in hunger, cravings and ghrelin suppression. Direct effects of meal timing (morning vs. evening increased calories) were not tested.
Objective: To search whether a change in meal timing by increasing calories in the morning vs in the evening has a differential impact on WL, ghrelin suppression, lipids and appetite scores. Our hypothesis is that comparing with high calorie dinner (D) + reduced B (HCDd), the high calorie B + reduced D (HCBd), would enhance WL, ghrelin suppression and appetite scores.
Methods: 73 obese women (BMI 32.3±2.0 kg/m2), aged 46±6 years, were randomized to two isocaloric (1400 kcal) weight loss diets during 12 weeks (Wk). Both diets had the same composition but differ in the meal timing distribution
1)HCBd consisted in large B with 700 Kcal(Kc)with % of CH; protein; fat: 50:30:20%; lunch (500 Kc, 20:45:25%), and small D (200 Kc, 13:40:47%).
2)HCDd consisted in low calorie B (200 Kc, 13:40:47%),lunch(500 Kc, 20:45:25%), and large D (700 Kc, 50:30:20%).
Anthropometric measures were assessed every 4Wk. Fasting glucose, insulin, ghrelin, lipids, OGTT, craving scores as well as B and D challenge were performed at baseline and at Wk12
Results: After Wk12 intervention, the HCBd group (g) lost 8.7±1.4 kg vs 3.48±2.3 kg the HCDd g. In comparison to the HCDd g, the HCBd g showed 61% greater WL, P<0.05,a 35% greater reduction in waist circumference (P<0.06) and a 17% greater reduction in percent body fat (P=NS). Ghrelin levels were reduced after B by 46.2% in the HCBd group and 18.5% after D in the HCDd g(P>0.005). Satiety was significantly improved and hunger and craving scores significantly reduced in the HCBd vs HCDd g (P>0.005). Mean serum triglyceride levels decrease by 44% (from 184.2±16.6 to 102.2±7.7 mg/dl) in the HCBd g while increase 6.3% (from 180.5±20.6 to 192.4±17.5 mg/dl) in the HCDd g(P>0.005). Total cholesterol (C), HDL-C and LDL-C, did not differ between the groups.
Conclusion: Isocaloric WL diets with different meal timing, differently influence WL rate, ghrelin, appetite and lipid levels. HCBd with reduced intake at D result in enhanced WL, increased ghrelin suppression and might be useful alternative for management of obesity.
June 26, 2012
ENDO Conference:Standard Dose of Vitamin D May Not Enough For Some Patients
[MON-350] Evaluation of Response to Treatment with 50,000 IU of Vitamin D3 in Deficient Patients
Tatiane Vilaca, Marilia Camargo, Marise Lazaretti-Castro. Universidade Federal de São Paulo - UNIFESP, São Paulo, Brazil.
Background: Inadequate vitamin D status has been associated with an increased risk of several diseases, including osteoporosis, cardiovascular disease, diabetes, cancer, multiple sclerosis and infections. Serum 25-hydroxyvitamin D is the classic marker of vitamin D status and is determined by environmental (season, latitude, sunlight, diet), demographic (ethnicity, body mass index) and genetic (polymorphism in metabolism and transport genes) factors. (1) However, the features that modify the response to vitamin D supplementation remain unclear. The Endocrine Society suggests the use of 50,000 IU of vitamin D2 or D3 weekly over eight weeks for the treatment of deficient adults to achieve a blood level of 25-hydroxyvitamin D above 30 ng/mL. (2)
Objective: The aim of the present study was to evaluate the response to supplementation with 50,000 IU of vitamin D3 in deficient patients.
Patients and Methods: Twenty-five osteoporotic female patients with vitamin D deficiency (25-hydroxyvitamin D < 20 ng/ml) received eight capsules of 50,000 IU of vitamin D3 for treatment. All capsules were manufactured at the same place. The patients were instructed to take one capsule a week for eight weeks. All patients reported appropriate adherence to treatment and none reported any gastrointestinal problems.
Results: After treatment, serum levels of 25-hydroxyvitamin D were reevaluated. More than half of the patients (13/25) did not achieve the levels recommended by the Endocrine Society (> 30 ng/ml). Both groups of patients (successful treatment and unsuccessful treatment) had similar body mass index values and initial pretreatment levels of 25(OH)-vitamin D. The group with the worse response was older.
Discussion: A number of authors have reported considerable inter-individual variation in serum 25-hydroxyvitamin D response to supplementation with identical doses. In the present study, this variation was found using the dose recommended by the Endocrine Society. The data suggest that the standard dose may not be enough to treat all patients and that reevaluation of vitamin D levels after treatment should always be considered.
1 Mason RS et al. European Journal of Clinical Nutrition (2011) 65, 986–993. 2 Holick MF el al. J Clin Endocrinol Metab. 2011 Jul;96(7):1911-30.
Sources of Research Support: São Paulo Research Foundation (FAPESP 2008/555677).
Nothing to Disclose: TV, MC, ML-C
Date: Monday, June 25, 2012
Session Info: POSTER SESSION: Vitamin D Deficiency & Metabolic Outcomes (1:30 PM-3:30 PM)
Presentation Time: 1:30 pm
Room: Expo

Tatiane Vilaca, Marilia Camargo, Marise Lazaretti-Castro. Universidade Federal de São Paulo - UNIFESP, São Paulo, Brazil.
Background: Inadequate vitamin D status has been associated with an increased risk of several diseases, including osteoporosis, cardiovascular disease, diabetes, cancer, multiple sclerosis and infections. Serum 25-hydroxyvitamin D is the classic marker of vitamin D status and is determined by environmental (season, latitude, sunlight, diet), demographic (ethnicity, body mass index) and genetic (polymorphism in metabolism and transport genes) factors. (1) However, the features that modify the response to vitamin D supplementation remain unclear. The Endocrine Society suggests the use of 50,000 IU of vitamin D2 or D3 weekly over eight weeks for the treatment of deficient adults to achieve a blood level of 25-hydroxyvitamin D above 30 ng/mL. (2)
Objective: The aim of the present study was to evaluate the response to supplementation with 50,000 IU of vitamin D3 in deficient patients.
Patients and Methods: Twenty-five osteoporotic female patients with vitamin D deficiency (25-hydroxyvitamin D < 20 ng/ml) received eight capsules of 50,000 IU of vitamin D3 for treatment. All capsules were manufactured at the same place. The patients were instructed to take one capsule a week for eight weeks. All patients reported appropriate adherence to treatment and none reported any gastrointestinal problems.
Results: After treatment, serum levels of 25-hydroxyvitamin D were reevaluated. More than half of the patients (13/25) did not achieve the levels recommended by the Endocrine Society (> 30 ng/ml). Both groups of patients (successful treatment and unsuccessful treatment) had similar body mass index values and initial pretreatment levels of 25(OH)-vitamin D. The group with the worse response was older.
Discussion: A number of authors have reported considerable inter-individual variation in serum 25-hydroxyvitamin D response to supplementation with identical doses. In the present study, this variation was found using the dose recommended by the Endocrine Society. The data suggest that the standard dose may not be enough to treat all patients and that reevaluation of vitamin D levels after treatment should always be considered.
1 Mason RS et al. European Journal of Clinical Nutrition (2011) 65, 986–993. 2 Holick MF el al. J Clin Endocrinol Metab. 2011 Jul;96(7):1911-30.
Sources of Research Support: São Paulo Research Foundation (FAPESP 2008/555677).
Nothing to Disclose: TV, MC, ML-C
Date: Monday, June 25, 2012
Session Info: POSTER SESSION: Vitamin D Deficiency & Metabolic Outcomes (1:30 PM-3:30 PM)
Presentation Time: 1:30 pm
Room: Expo
June 25, 2012
Results from a 15 year study using a long acting testosterone injection (Nebido) show great improvements in several parameters in men
More from the ENDO meeting happening now in Houston :
Results from a 15 year study using Nebido injections (it will be called Aveed when it is hopefully approved in the US). I am amazed on how HDL increased since that kind of dose is usually associated with decreases in HDL cholesterol. Almost too good to be true but it was probably due to the weight loss and reduction in metabolic syndrome in those men.
http://www.abstracts2view.com/endo/view.php?nu=ENDO12L_SAT-117




