
Nelson Vergel's Blog, page 10
April 29, 2012
Best Testosterone Interview- Dr Michael Scally
From: Testosterone: A Man's Guide (click here for amazon link)
Interview WithDr. Michael ScallyNelson Vergel (NV): Dr. Michael Scally is a well-known expert on men’s health in general, and specifically he’s an expert on hormone therapy and issues surrounding testosterone replacement. Dr. Scally, can you tell us a little bit about your background?Michael Scally (MS): My education includes a double degree major in chemistry (1975) and life sciences (1975) from the Massachusetts Institute of Technology (MIT) Cambridge, MA. From 1975 to 1980, in the MIT division of Brain Sciences & Neuroendocrinology, I researched and published investigations on neurotransmitter relationships. During this time, I entered the prestigious Health Sciences & Technology Program, a collaboration of the MIT and Harvard Medical School. In 1980, I was awarded by Harvard Medical School a Doctorate of Medicine, MD. In 1983, I completed a fellowship in anesthesiology at Parkland Southwest Memorial, in Dallas. From 1983 to 1994, I was a private practice anesthesiologist. In 1984, I set up the first ambulatory, outpatient, surgery center at Houston.In 1994, I became interested in general and preventative medicine with a focus on endocrinology. I have been active in this area since that time.In 1995, I inquired to Wyeth Pharmaceuticals about the association between primary pulmonary hypertension and pondimin (fenfluramine). I came to learn, this inquiry later was used as evidence in the class-action suit against Wyeth and was instrumental in showing that the known adverse effects were known to Wyeth but not revealed to the public.During 1994, I competed in the Mr. Texas Bodybuilding Championship, placing second. While exercising, I was approached by a number of weightlifters on the medical treatment to restore the hypothalamic-pituitary axis (HPTA) after stopping anabolic steroids (AAS). Many of these same individuals also used over-the-counter (OTC) supplements.As you might know, many bodybuilders are trying to decrease their body fat and increase their muscle mass as much as they can. And with these two specific goals in their mind, they were having a hard time because they were taking this over-the-counter supplement. Within a short time later, I discovered an over-the-counter weight loss supplement containing an ingredient, tiratricol, toxic to the thyroid. The reporting of this to the federal agency, MedWatch, was instrumental in the nationwide seizure of the supplement thus avoiding a disaster to the public health and welfare. We published our findings in the peer-reviewed literature, being the first to do so.This spurred on my interest in the field of men’s health, particularly in the field of testosterone and anabolic steroids. I recognized the use of a treatment for stopping anabolic steroids, both prescription and nonprescription, was without any scientific support. The accepted standard of care within the medical community for anabolic steroid-induced hypogonadism is to do nothing with the expectation the individual will return to normal unassisted. This is proving not to be the case and now jeopardizes the health and welfare of countless individuals.I developed a treatment for anabolic steroid-induced hypogonadism that has been published and presented before the Endocrine Society, the American Association of Clinical Endocrinologists, American College of Sports Medicine, and the International Workshop on Adverse Drug Reactions and Lipodystrophy in HIV. The condition of anabolic steroid-induced hypogonadism is found in nonprescription and prescription AAS alike. The failure of the medical community to recognize the importance of anabolic steroid-induced hypogonadism, particularly in the research setting, is the focus of my recently published book, “Anabolic Steroids—A Question of Muscle: Human Subject Abuses in Anabolic Steroid Research.”NV: There are lots of misconceptions when it comes to testosterone replacement in men. Will you tell us, in your opinion, what are the main misconceptions? For instance, some doctors may think that giving testosterone to somebody with low testosterone may affect the liver, or may cause cancer of the liver or prostate.MS: There are many misconceptions regarding anabolic steroids, which include testosterone. You mentioned two of the areas: liver and prostate cancer. Other areas are enlargement of the prostate or benign prostate hypertrophy, anabolic steroid dependency, cardiovascular disease, and addiction.I believe that many of the misconceptions come about by the politicization of anabolic steroids. As far as prescribed medicines are concerned, anabolic steroids are the only group of drugs with a law specifically aimed at their use. This has led to a lack or absence of good research. Instead, what the medical community has relied on are anecdotal and inflammatory reports.This is probably most evident in the medical community’s steadfast refusal to accept that anabolic steroids increase muscle mass and strength. We now know that anabolic steroids conclusively do increase muscle mass and strength and athletic performance.As far as liver effects, use of the oral anabolic steroids has been reported to cause liver dysfunction and cancer. These reports are primarily in individuals with a preexisting condition treated for extended periods. The intramuscular injections and transdermal preparations do not appear to be associated with liver problems, and routine monitoring is therefore unnecessary. In the thousands of patients I have treated with testosterone, I never even think about liver problems being a contraindication, because they just do not come up.In non-obstructive benign prostatic hyperplasia (BPH), testosterone replacement therapy is not a concern. The prostate volumes increase in an inconsistent manner. As with any treatment, careful monitoring will alert one to a problem.As far as prostatic cancer, there is no association. In 2004, a New England Journal of Medicine article review of over 60 studies on testosterone replacement therapy concluded that there is no causal or association with prostate cancer.NV: But testosterone replacement seems to be getting more and more mainstream. Ever since the introduction of gels like Androgel and Testim, more and more doctors feel comfortable prescribing testosterone. But yet, there are still a lot of fears, too. Another fear is changes in lipids and cardiovascular risks associated with testosterone. Can you expand on that a little?MS: The available data indicate that testosterone replacement therapy within the physiologic range by transdermal or injectable testosterone preparation is not associated with worsening of the lipid profile. Studies using physiologic replacement doses of testosterone show no change, or only a slight decrease, in HDL, often with a reduction in total cholesterol. The oral non-aromatizable anabolic steroids appear to lower high-density lipoprotein (HDL) levels.The belief that testosterone is a risk factor for cardiac disease is based on the observation that men have both a higher incidence of cardiovascular events and higher testosterone levels than women do. There is little data for this idea. Many studies suggest the opposite. There are multiple studies showing a relation between hypogonadism and an increased cardiovascular risk.There is evidence that testosterone replacement therapy may be beneficial for men with cardiac disease. In a small study, men with chronic stable angina who were treated with transdermal testosterone replacement therapy had greater angina free exercise tolerance. Importantly, testosterone replacement therapy has not shown an increased incidence of cardiovascular disease or stroke.NV: There are some data on hypogonadism and increased risks of cardiovascular events. Is that what you mean? Some people actually become so severely hypogonadal, they actually may be risking higher incidence of heart attacks and strokes?MS: That is correct. There are numerous studies demonstrating the relationship between low testosterone levels and adverse cardiovascular events, as well as stroke. Also, there are case study reports of people who stop anabolic steroids, and then suffer a heart attack. In the book that I wrote, one of the studies in the published literature, looking at the effects of anabolic steroids in certain populations, for 12 weeks, did not look at the patients after they stopped the drug. If you want to lookat the effects of these drugs, you need to see what happens when you stop them. I filed a Freedom of Information Act to obtain the patient records. One of the patients actually suffered a heart attack within four weeks of stopping the anabolic steroid. The details, including the original patient records, of this case are reported in my book.
NV: Should patients with an increased or elevated prostatic specific antigen (PSA) avoid testosterone? What role does testosterone replacement therapy (TRT) have on prostate cancer, if any? Is there a risk of worsening prostate cancer with TRT?MS: You brought up a number of important and controversial issues. It is generally agreed that TRT with established prostate cancer is contraindicated.It is known that suppression of testosterone levels causes regression of prostate cancer, and it is now commonplace for men with metastatic prostate cancer to undergo treatment designed to lower testosterone levels. The question becomes if lowering testosterone causes prostate cancer to regress, does elevating testosterone cause prostate cancer to appear?There are case reports suggesting that TRT may convert an occult cancer into a clinically apparent lesion. These studies are wrong. One must be very careful in attributing causality to testosterone, since over 200,000 men are given a diagnosis of prostate cancer each year, and most of these cases are first detected by a rise in the PSA level unrelated to testosterone therapy. Studies have demonstrated a low frequency of prostate cancer in association with TRT. Despite extensive research, there is no compelling evidence that testosterone has a causative role in prostate cancer.There appears to be no compelling evidence at present to suggest that men with higher testosterone levels are at greater risk of prostate cancer or treating men who have hypogonadism with exogenous androgens increases this risk. In fact, prostate cancer becomes more prevalent exactly at the time of a man’s life when testosterone levels decline.Little evidence exists on the safety of TRT initiation after treatment for primary prostate cancer. In one very small case series, TRT after treatment of organ confined prostate cancer produced no adverse effects. There are no large, long-term studies proving that the risk of recurrence is not affected by TRT. Personally, I would be reluctant to provide TRT in prostate cancer; treatment should be left to strict research protocols.PSA is a serum glycoprotein made by the normal prostate that is widely used as a tumor marker, because elevated PSA levels correlate with the risk of prostate cancer. A PSA value greater than 4.0 ng/mL has been the standard indication for prostate biopsy since the introduction of this test in the 1980s.Testosterone trials have inconsistently shown a rise in PSA, typically between 0.2 and 0.5 ng/mL. A greater increase in PSA arouses concern that prostate cancer has developed. It is my practice to recommend a prostate biopsy in any patient with a yearly PSA increase of 1.0 ng/mL or more. If the PSA level increases by 0.75 ng/mL in one year, I repeat the PSA measurement in three to six months and recommend a biopsy if there is any further increase.NV: Can you explain what polycythemia is and what it means when it comes to cardiovascular risk and other issues?MS: In respect to anabolic steroid-induced polycythemia, polycythemia is a condition that results in an increased level of circulating red blood cells in the blood stream. Erythrocytosis is a more specific term that is used to denote increased red blood cells. People with polycythemia have an increase in hematocrit, hemoglobin, or red blood cell count above the normal limits. The reporting of polycythemia is typically in terms of increased hematocrit or hemoglobin.Hematocrit is a blood test that measures the percentage of red blood cells found in the whole blood. This measurement depends on the number and size of red blood cells. Normally, for a male, the hematocrit raises up to a level of 52–54 depending on the reporting laboratory reference range. Polycythemia is considered when the hematocrit is greater than the upper limit of normal.Hemoglobin is the protein molecule in red blood cells that carries oxygen from the lungs to the body’s tissues and returns carbon dioxide from the tissues to the lungs. The hemoglobin level is expressed as the amount of hemoglobin in grams (g) per deciliter (dl) of the whole blood, a deciliter being 100 mL, for adult males: 14–18 gm/dL. Polycythemia is considered when a hemoglobin level is greater than 18 g/dL in men. It is a thickening of the blood. The blood becomes almost like sludge. You would think that with the increased number of red blood cells, it would carry more oxygen; but its oxygen-carrying capacity decreases markedly. Without treatment, polycythemia can be life threatening. Elevation above the normal range may have grave consequences, particularly in the elderly, since an attendant increase in blood viscosity could aggravate vascular disease in the coronary, cerebrovascular, or peripheral vascular circulation. However, with proper medical care, many people experience few problems related to this disease.Symptoms of polycythemia can be none to minimal in many people. Some general and nonspecific symptoms include weakness, fatigue, headache, itching, redness of your skin, bruising, joint pain, dizziness, abdominal pain, shortness of breath, breathing difficulty when you lie down; and numbness, tingling, or burning in the hands, feet, arms, or legs.NV: Or when they work out, they turn red.MS: That can certainly be a symptom of polycythemia.NV: Is the incidence of polycythemia related to the route of administration, dose, duration, and age? Is polycythemia common in replacement doses?MS: Yes. It occurs quite frequently in people who are just on replacement testosterone. Older men appear more sensitive to the erythropoietic effects of testosterone than young men do. Both testosterone dose and mode of delivery affect the magnitude of hematocrit elevation.The incidence of testosterone-associated polycythemia may be lower in males receiving pharmacokinetically steady-state delivery of testosterone formulations, than it is in receiving intramuscular injections.In patients using topical preparations, there is a 5–20 percent incidence of erythrocytosis. There is an apparent direct relation between testosterone dosage and the incidence of erythrocytosis. Erythrocytosis occurs in about 5– 15 percent by patches and in 10–20 percent with gel preparations depending on the use of 50 mg/day (delivering 5 mg /day) and 100 mg/day (delivering 10 mg/day) during the course of approximately 14 year.
The most commonly used forms of intramuscular-injectable testosterone esters are testosterone enanthate and cypionate. Injectable testosterone esters generate supranormal testosterone levels shortly after injection and then testosterone levels decline very rapidly, becoming subnormal in the days before the next injection.Testosterone ester injections have been reported to be associated with a higher risk of erythrocytosis than transdermal testosterone. It is unclear whether the higher frequency of erythrocytosis observed with injectable testosterone esters is due to the higher dose of testosterone delivered by the injections or the higher peaks of testosterone levels. In one study, intramuscular injections of testosterone enanthate produced an elevated hematocrit over 40 percent.NV: Is therapeutic phlebotomy a good way to manage polycythemia?MS: Untoward events are unlikely with mild erythrocytosis of relatively short duration. Therapeutic phlebotomy and blood donation are overall a safe procedure, the frequency of side effects being low and their severity weak. Other options include dosage reduction or the withholding of testosterone. However, these latter options can be problematic since the patient will experience symptoms of anabolic steroid-induced hypogonadism.This does present a catch-22 for many physicians. Because the half-life of the red blood cell is approximately 120 days, it might be a considerable length of time, more than three months or longer, to normalize the hemoglobin or hematocrit upon TRT cessation. But, the problem of anabolic steroid-induced hypogonadism symptoms complicated matters.Many a times, an attempt will be to maintain TRT while simultaneously performing a therapeutic phlebotomy. Because of the increased erythro-poiesis, production of red blood cells, it feels like the proverbial chasing one’s tail. In a number of therapeutic phlebotomies, the units of the blood that have to be taken off are clearly quite excessive; and we do not want to do that too quickly. It may come to be three, four, or even five pints of blood that have to be taken off.In order to get a good hold on the problem of polycythemia, it will be necessary to discontinue TRT. What we have done again, in our protocol, is that we have stopped the testosterone, thereby removing the cause of the increased red blood cell production, treat them with the HPTA protocol that prevents the hypogonadism, and have the therapeutic phlebotomy done. They are able to get the hemoglobin or hematocrit down to the normal level, do not go through the adverse effects of the hypogonadism; and then, at the other end, be able to start the testosterone therapy again. As far as we can determine, no testosterone associated thromboembolic events have been reported to date.NV: I am actually surprised how many patients are out there that do not have their physician following up their hematocrit when they are put on testosterone or anabolics for wasting syndrome. It is something that the physician should be looking out for and measuring.MS: The hemoglobin and hematocrit is part of the routine laboratory follow-up for anyone on TRT. If a patient complains of any of the symptoms we describe for polycythemia, a hemoglobin and hematocrit should be checked. One of the confounding problems is the symptoms tend to be nonspecific.NV: Can you say something about the prophylactic use of finasteride or dutasteride to avoid DHT-related problems like prostate enlargement or hair loss? Is there a role for the use of finasteride or dutasteride to prevent the possible increase of hair loss with TRT?MS: Finasteride and dutasteride are 5-alpha reductase inhibitors. 5-alpha reductase comes in two forms, type 1 and type 2, and is responsible for the conversion of testosterone into DHT. Finasteride inhibits type 2 only while dutasteride inhibits both forms.Finasteride comes in two doses depending on whether the indication is for hair loss or benign prostate hypertrophy. Propecia, 1 mg, is for hair loss. Proscar, 5 mg, is for prostatic hypertrophy.DHT has been shown to be important in the development of hair loss or male pattern baldness. I am unaware any studies indicating a worsening of hair loss or male pattern baldness, though this possibility has not been carefully studied. There are anecdotal reports. The prophylactic use of these drugs is an individual decision after weighing the risks and benefits.DHT is also important in prostate health. It is thought an overabundance of DHT may be important in benign prostatic hyperplasia (BPH) and prostate cancer. Dutasteride provides greater suppression of DHT than finasteride does, thereby underlying the hypothesis that inhibition of both type 1 and type 2 would provide correspondingly greater protection than inhibition of type 2 alone.However, significant side effects of finasteride use include reduced volume of ejaculate, erectile dysfunction, loss of libido, and gynecomastia. This will prevent many from their use.Some people think that DHT will affect lean body composition. DHT does have a higher affinity for the androgen receptor. But the enzyme that converts testosterone into DHT is not located in the muscle. There is no evidence for these drugs to effect muscle mass.NV: What about other issues related TRT, such as to increased estrogen levels and gynecomastia?MS: A small number report breast tenderness and swelling. Fluid retention is uncommon and generally mild, but TRT should be used cautiously in men with congestive heart failure or renal insufficiency. After confirmation of elevated estrogen, estradiol, levels, this can be treated with either an aromatization inhibitor or estradiol receptor blocker. This must be done very carefully as any prolonged reduction in estradiol levels runs the risk of causing osteoporosis.Exacerbation of sleep apnea or the development of sleep apnea has been associated with TRT who have other identifiable risk factors for sleep apnea. The mechanism appears to be central mediated rather than by means of changes in the airway. Other side effects include acne, oily skin, increased body hair, and flushing. Hypertension has rarely been reported.Of course, the adverse effect I am most concerned with is androgen-induced hypogonadism, which occurs in one hundred percent of individuals stopping TRT, the variables being the duration and severity.On testosterone replacement therapy, for those without organic hypogonadism, those with late onset of hypogonadism, the only thing that I always caution about is that people should not be on testosterone replacement therapy, year after year after year, without stopping every 12–18 months to restore the axis, to make sure the function is still there. The longer you are on testosterone, the harder it is going to be to come off testosterone.NV: In your opinion, can you tell us a little bit about the different options for TRT? Have you seen any difference in using gels versus injections? Is there any advantage or disadvantage to using either one?MS: Injectable, transdermal, buccal, and oral testosterone formulations are available for clinical use. These forms of treatment differ in several key areas.Oral preparations include methyl testosterone and fluoxymesterone, which are rarely prescribed because of their association with substantial liver toxicity. In Europe, there is an oral preparation of testosterone undecanoate, Andriol. It has a poor history of bioavailability.Recently, the FDA approved a buccal preparation of testosterone, Striant. Striant requires administration twice a day. It is used little at this time.Transdermal testosterone is available as a patch, Testim, and gel, Androgel. Daily application is required for each of these. They are designed to deliver 5–10 mg of testosterone a day. The advantages include ease of use and maintenance of relatively uniform serum testosterone levels over time. Skin irritation in the form of itching and redness is a frequent adverse effect of Testim with reports as high as 60–70 percent. This is uncommon with Androgel. Inadequate absorption through the skin may limit the value of transdermal preparations in some persons. A common problem is the low dose preparations provide inadequate serum testosterone levels. This is also seen with the high dose.The topical have become, by far, the most-used products in the last decade or so, approaching a billion dollars in sales. Androgel is the biggest product of the topical.If the patient is not too scared of doing injectables, oil-based testosterone ester preparations are available. The most commonly used injectables are Delatestryl or testosterone enanthate and depo testosterone or testosterone cypionate. In my practice, the typical dose is between 100 and 150 mg/week. The peak serum levels occur in 2–5 days after injection, and a return to baseline is usually observed 10 days after injection. In this manner, adequate serum levels are maintained. Intramuscular injections of testosterone can cause local pain, soreness, bruising, redness, swelling, and possible infection.NV: Most doctors prescribe 1-cc of 200 mL of testosterone every two weeks. Can you describe the problems with this schedule, if any?MS: This is a problem that is seen much more often than necessary. Many doctors use a typical dose is 100 mg/week or 200–300 mg every two to three weeks.Within 7–10 days after injection, the serum testosterone levels are low to abnormally low. This is described as a “roller coaster” effect, characterized by alternating periods of symptomatic benefit and a return to baseline symptoms, corresponding to the fluctuations in serum testosterone levels. This can be discovered by having the testosterone level checked within 24 hours prior to injection.NV: Can you talk to us a little bit about compounding pharmacy products? In particular, when using testosterone gels with concentrations higher than 1 percent for reaching total testosterone blood levels above 500 ng/L. Have you had any experience with the compounding industry?MS: I have had some experience with the compounding industry. Compounding pharmacies are very capable at providing higher concentrations of transdermal testosterone preparations. Because of this, they are able to supply a transdermal product in small volumes. They also tend to be less expensive than commercially available pharmaceutical testosterone replacement options.NV: Do you think it is advisable to get your testosterone levels rechecked after a few weeks of starting any of the therapies?MS: My protocol is that once I start a patient on testosterone, I check the testosterone level 4–6 weeks after initiating TRT. In patients using topical preparations, I recommend testing within 4–6 hours after application. Those using injectables of testosterone esters, I recommend testing within 24 hours before their next scheduled injection.NV: Do you have any preference between the free testosterone and total testosterone test?MS: In the monitoring of the patient on TRT, I utilize the total testosterone. The initial evaluation of a patient might include the use of free testosterone or bioavailable testosterone. In a symptomatic individual, the total testosterone can be normal but the free or bioavailable testosterone abnormal.Testosterone circulates in three forms. Testosterone circulates in a free or unbound state, tightly bound to SHBG, or weakly bound to the blood protein albumin. Bioavailable, non-SHBG, testosterone includes free testosterone and testosterone that is bound to albumin but does not include SHBG -bound testosterone.Examined changes over time have demonstrated a decrease in the total testosterone and an increase in SHBG levels. Because of this, the total testosterone might be normal, whereas the free or bioavailable testosterone is abnormal. If these alternative methods are used to diagnose hypogonadism, their utility during TRT is limited.I would caution about the assay methodology used to calculate the free or bioavailable testosterone. The methods used to conduct the measurements vary in their accuracy, standardization, the extent of validation, and the reproducibility of results.Bioavailable testosterone is measured or calculated in several ways. SHBG bound testosterone can be precipitated with ammonium sulfate and the remaining testosterone is then taken as the bioavailable.Measures of free testosterone (FT) are controversial. The only standardized and validated method is equilibrium dialysis or by calculating free testosterone levels based on separate measurements of testosterone and SHBG. Other measures of free testosterone are less accurate.NV: And your goal is usually to have patients above what level?MS: I like their total testosterone trough or lower level to be in the 500–700 range, normal being 300–1,000 ng/dL.NV: Besides checking of the initial T level, can you elaborate on the monitoring during TRT?I recommend a periodic follow-up of patients receiving replacement testosterone therapy at the interval of three months during the first year of treatment. Afterward, patients are followed up every six months. It is important to do a review of systems to ensure the relief of the complaining symptoms as well as no worsening or new symptoms.In addition to the serum total testosterone, I routinely monitor the basic chemistry profile, which includes liver function, kidney function, electrolytes, glucose, lipid panel, and hemoglobin or hematocrit. At three months, I will often include estradiol and DHT levels.If the patient is older than 50 years, I include the PSA. The role of digital rectal examination (DRE) and PSA in detecting early, clinically significant, prostate cancer is controversial. I discuss this with each patient and allow them to decide on their use.NV: How about the new non-steroidal androgens that are in the pipeline? Can you tell us what you have read about them?MS: They are called SARM: selective androgen receptor modulators. They are going to become more and more popular. The closest SARM that is coming to the market, and it is years away, is called ostarine. It is being developed by GTx, Inc. Ligand Pharmaceuticals has a SARM in early phase of development. They are both traded on the NASDAQ Exchange.The initial studies are being done in cancer patients. The data collected is change in muscle mass and strength. The clinical outcome being measured is the six-minute walk test.My feeling on this is that we have a long way to go before these things come to market. If they come to market within the next 5–10 years, we will be lucky. As far as I know, these are the only SARMs in human clinical trials.NV: I have also heard that SARMs may not have any influence on sexual function, only on lean body mass and maybe some functional capacity. They are really not replacement of testosterone. Are they?MS: From the initial studies, these are meant to take the place of anabolic steroids, not testosterone. There are no indications SARMs are being developed as TRT. The data from both animal and human studies is that they act similarly, if not identically, to anabolic steroids. They act through the androgen receptor. They do cause HPTA suppression.Even though they have the same effect, they will be able to be marketed without that name “anabolic steroids.” This would be an obvious advantage in their marketing. It should be noted that these drugs, SARMs, have already found their way into the nonprescription or illicit market.NV: Can somebody on testosterone replacement become less fertile? If a man wants to impregnate his wife after, let us say, a year of testosterone replacement, is there any risk for that man to become less fertile to his wife?MS: Testicular size and consistency often diminish, and men should be advised that fertility would be greatly compromised during testosterone replacement therapy because of downregulation of LH and FSH.The general rule is they will become less fertile. But you cannot depend on its use as a fertility drug. And that is where we come in with contraceptive studies. We have many, many contraceptive studies that use testosterone cypionate at 200 mg a week and find that, yes, it decreases fertility. But there is still a subset of men that still produce sperm that are fertile.NV: Are these men good candidates for a protocol to reset their HPGA?MS: We have had many men who come to the clinic with the actual complaint that they were using anabolic steroids, or they were using testosterone, and they now want to get their wife pregnant. Although many will return to normal after stopping TRT, this period can be lengthy.The amazing thing to me is that the number of people that come to me, who have seen the doctor, who are either non-prescription or prescription anabolic steroid users, testosterone with or without combination of anabolic steroids, who have the problem of infertility; and their doctors have no idea what to do, except to do nothing. But on top of this are all the psychological problems and effects that come along with doing nothing as a consequence of anabolic steroid-induced hypogonadism. The HPTA protocol has restored fertility as well as decreased the time substantially.NV: Can you expand about resetting the HPGA?The word resetting is a misnomer, though recent studies published in the New England Journal of Medicine (NEJM) do indicate this possible. In 2007, the NEJM reports on the resetting of the HPTA after TRT for adult onset idiopathic hypogonadism. This is the first report demonstrating HPTA plasticity in adulthood. The term I prefer is HPTA functionality and restoration.There are clear conditions under which testosterone requires administration for life-long treatment. However, there are increasing numbers of individuals being treated with TRT who do not fall under these disorders. TRT is being prescribed more and more for late onset hypogonadism. This is called by many other names, including andropause, androgen deficiency of the aging male, and others.There are no consequences of the decline in serum testosterone with age that are known with certainty. Several parallels exist between the effects of aging and those of hypogonadism, which suggest that the decline in serum testosterone might be a cause of several effects of aging. Since the long-term effects of androgen treatment for late onset hypogonadism or andropause are not well-known, I discontinue therapy on an approximate annual basis to ensure HPTA normalization—functionality. This allows the patient the autonomy to stop therapy should the need arise.What is clear is that upon stopping testosterone or anabolic steroids, a period of anabolic steroid-induced hypogonadism ensues. This occurs in one hundred percent of individuals stopping testosterone. The only variables are the duration and severity. The duration of hypogonadism, or the severity of hypogonadism, is typically related to the anabolic steroid drug, dose, and duration.In other words, one person that is on testosterone for an entire year; they may come back to normal within 1 or 2 months. Another person may take 12, 18 months, or even 3 years to come back to normal. The best studies we have on this are contraceptive studies with testosterone for over a year. And what we find in those studies is that it may take up to three years for a person to return to normal.If they have been taking those anabolic steroids to improve their body composition, increase the lean body mass, and decrease the body fat, that all goes back to normal after stopping anabolic steroids. But you are also going to be exposed to the other adverse effects of hypogonadism, which include adverse psychological and cardiovascular effects. Some of the adverse psychological effects are depression, decreased cognitive abilities, insomnia, decreased libido, and erection dysfunction. More significantly, after cessation adds the comorbid condition of hypogonadism to their already existing chronic illness.AAS, including testosterone, licit and illicit, administration induces a state of hypogonadism that continues after their cessation. All compounds classified as androgens or anabolic steroids cause a negative feedback inhibition of the hypothalamic-pituitary testicular axis, suppress endogenous gonadotropin secretion, and as a consequence serum testosterone.The symptoms of AIH are identical to classical hypogonadism. This problem prevents many of discontinuing testosterone or anabolic steroids. As we have said, there are many reasons for stopping testosterone, including polycythemia, gynecomastia, and other issue as compliance, affordability, and changing life style.The accepted standard of care within the medical community for anabolic steroid induced hypogonadism is to do nothing with the expectation the individual will return to normal unassisted. But the literature shows this not to be the case.AIH is critical toward any planned use of AAS or similar compound to effect positive changes in muscle mass and muscle strength as well as an understanding for what has been termed anabolic steroid dependency. The further understanding and treatments that mitigate or prevent AIH could contribute to androgen therapies for wasting associated diseases and stopping nonprescription AAS use.NV: What is used for restoring the hormonal axis?MS: A combination of three drugs. The individual use of HCG, clomiphene citrate, and tamoxifen is well-known, well-accepted, and well-tested standards of care treatments in peer-reviewed medical literature for diagnostic testing for underlying pathology of hypogonadism. The HPTA protocol uses the medications human chorionic gonadotropin, clomiphene citrate, and tamoxifen.The first phase of the HPTA protocol examines the functionality of the testicles by the direct action of HCG. HCG raises sex hormone levels directly through the stimulation of the testes and secondly decreases the production and level of gonadotropin LH. The increase in serum testosterone with the HCG stimulation is useful in determining whether any primary testicular dysfunction is present.This initial value is a measure of the ability of the testicles to respond to stimulation from HCG. Demonstration of the HPTA functionality is an adequate response of the testicles to raise the serum level of T well into the normal range. If this is observed, HCG is discontinued. The failure of the testes to respond to an HCG challenge is indicative of primary testicular failure. In the simplest terms, the first half of the protocol is to determine testicular production and reserve by direct stimulation with HCG. If one is unable to obtain adequate (normal) levels successfully in the first half, there is little cause or reason to proceed to the second half.The second phase of the HPTA protocol, clomiphene and tamoxifen, examines the ability of the hypothalamic-pituitary axis to respond to stimulation by producing LH levels within the normal reference range. The clomiphene citrate challenge differentiates secondary hypogonadism. Clomiphene is an antiestrogen, which decreases the estrogen effect in the body. It has a dual effect by stimulating the hypothalamic pituitary area and it has an antiestrogenic effect, so that it decreases the effect of estrogen in the body. Tamoxifen is more of a strict antiestrogen; it decreases the effect of estrogen in the body, and potentiates the action of clomiphene. Tamoxifen and clomiphene citrate compete with estrogen for estrogen receptor binding sites, thus eliminating excess estrogen circulation at the level of the hypothalamus and pituitary, allowing gonadotropin production to resume. Administering them together produces an elevation of LH and secondarily gonadal sex hormones. The administration of clomiphene leads to an appropriate rise in the levels of LH, suggesting that the negative feedback control on the hypothalamus is intact and that the storage and release of gonadotropins by the pituitary is normal. If there was a successful stimulation of testicular T levels by HCG, but an inadequate or no response in LH production, then the patient has hypogonadotropic, secondary, hypogonadism.In the simplest terms, the second half of the protocol is to determine hypothalamo-pituitary production and reserve with clomiphene and tamoxifen. The physiological type of hypogonadism—hypogonadotropic or secondary—is characterized by abnormal low or low normal gonadotropin (LH) production in response to clomiphene citrate and tamoxifen. In the functional type of hypogonadism, the ability to stimulate the HPTA to produce LH and T levels within the normal reference range occurs.There is a dearth of good studies in anabolic steroids, both while you are taking them and after you stop them, I think this is going to be something that we are going to need to look at in the future. In fact, we are going to plan on looking at it in our proposed clinical studies that we have with our company for the prevention of anabolic steroid-induced hypogonadism.Dr Michael Scally can be contacted at mscally@alum.mit.edu . His book “Anabolic Steroids - A Question of Muscle: Human Subject Abuses in Anabolic Steroid Research” is available on Amazon.com



April 28, 2012
Is It Safe to Have Your Prescription Filled At A Compounding Pharmacy?

For centuries, physicians have prescribed medications for their patients. The pharmacist followed exactly the physician's specifications and meticulously formulated these prescriptions. As the science of medicine advanced, many of the standard prescriptions began to be formulated and manufactured by pharmaceutical manufacturers. Most phamacists welcomed the change, since this removed most of their physical hand labor. Now phamacists could concentrate on spending more time with the patients and the dispensing and counseling process.
However, physicians began to notice that not all patients responded to the standardized manufactured medicines. There was still a need to formulate or "compound" prescriptions to the individual needs of these patients. Many patients were sensitive to the various fillers, dyes and preservatives that were used in commercial medicines. A few pharmacists responded to theses special needs by continuing to carefully compound these prescriptions to the exact specifications ordered by the physician without the offending chemicals. Some medications have been discontinued by the manufacturers simply because it became unprofitable to manufacture them. This became a real problem for the patient who had responded well to these drugs. Where could this person obtain their needed medication? Again, the compounding pharmacist is usually able to meet this need.
The compounding pharmacist who is committed to the art and skill of prescription compounding has made a significant investment in obtaining pure drugs and chemicals along with highly specialized equipment in order to make these medications. The compounding pharmacist must be involved in obtaining extra education and training which is unique in the profession of pharmacy. Compounding laboratories and sterile environments are all part of the compounding pharmacy. Literature to verify and validate the use of unique compounded medications must be researched and distributed to the physicians who choose to treat the unique needs of their patients.
FrequentlyAsked Questions about Compounding
(This comes from the International Academy of Compounding Pharmacists (IACP) www.iacprx.org)
What is pharmacy compounding?
In general, pharmacycompounding is the customized preparation of a medicine that is not otherwise commercially available. These medications are prescribed by a physician,veterinarian, or other prescribingpractitioner, and compounded by a state-licensed pharmacist. A growing number of people and animals have unique health needs that off-the-shelf, one- size-fits-all prescription medicines cannot meet. For them, customized medications are the only way to better health.
Who are compounding pharmacists?
Pharmacy compounding is a centuries-old, well-regulated and common practice. Pharmacists are some of the most respectedand trusted professionals in the United States. In a recent survey, pharmacists ranked second (only behind nurses)as the most trusted professionals in American society. Compounding has evolved into a specialtypractice within the pharmacy community today. New applications to meet today’s patient needs require additional education, equipment, and processes that not all pharmacies possess.
How are compounding pharmacies and pharmacists regulated? Should there be increased federal oversight?
All pharmacies and pharmacists are licensed and strictly regulated at the state level. Compounding is acore component of pharmacy and has always been regulated by state boards, which are constantly updating their standards and regulations. In addition,standards set by the United States Pharmacopeia (USP) are integrated into the practiceof pharmacy compounding. The PharmacyCompounding Accreditation Board (PCAB) has developed national standardsto accredit pharmacies that perform a significant amount of compounding.
Does the FDA have the expertise and federal powerto regulate compounding pharmacies? Why shouldn’t compounded medications, especially the most commonly used combinations, have to go through FDA’s established drug approval process?
The medicalprofession, including the practice of pharmacy, has always been regulated by the states. State boards of pharmacy are in the best position to inspect pharmacy operations, develop appropriate regulations, and respond to problemsor violations. The FDA does have an important role to play in makingsure that ingredients used in compounding are safe and are manufactured by the FDA-registered and inspected facilities, but there is no such thing as an “FDA-approved” pharmacy.
The FDA’s drug approvalprocess takes yearsand can cost hundreds of millions of dollars. Requiring this for individuallypersonalized medications that fulfill an individual doctor’s prescription is both impractical and contrary to the best interestsof patients requiring immediatetreatment.
What suppliers sell ingredients to compounding pharmacies? How are these suppliers regulated?
Just like big pharmaceutical manufacturing companies, compounding pharmacies get their ingredients for medications from the suppliers that areregistered and inspected by the FDA. Foreign suppliers are FDA- registered facilities.
There are thousands of FDA-approved drugs on the market for just about any ailment. Why do we still need compounded medications?
Some valuable medications and their different delivery methods are only available by compounding. Restricting a doctor’s access to compounded medications would be a serious mistake.Moreover, because of the economics of pharmaceutical manufacturing, FDA-approved drugs that serve a limited population are often discontinued by manufacturers. In mostof these cases the only option left fordoctors and theirpatients is to havea compounding pharmacist make the discontinued drug from scratch using pharmaceutical grade ingredients.
Are compounded medications safe? How does one know that the compounded medication they are taking is safe and effective?
Compounded medications are similar to the so-calledoff-label use of FDA-approved drugs. When the FDA approves a specific drug as safe andeffective, this determination appliesonly to the specific disease or condition for which the drug was tested. But physicians and veterinarians often prescribe medications for treatments for which they have not been specifically approved. Medical professionals do this because,in their judgment, the treatment is in the best interest of the individual patient.
Similarly, medical professionals often prescribe compounded medications because they believeit is the best medical option for their patients. It is estimated that one fifth of all prescriptions writtenfor FDA-approved drugs are for uses for which they were not specifically approved.
Compounding Pharmacy :
There are compounding pharmacies in most large cities in the United States. However, not all are the same when it comes to pricing, customer service, and compliance to sterilization regulations. You should call them to compare prices and to provide your credit card and addressinformation. Prices for testosterone products (creams, injections, pellets), HCG, TRIMIX, clomiphene (Clomid), anastrazole (Arimidex), nandrolone, pain creams, Sermorelin, estrogen/progesterone creams, erectile dysfunction medications in sublingual and other fast acting formulations and other compounded products can vary widely among compounding pharmacies. If your doctor uses only one compounding pharmacy, tell him or her that you will shop around before committing to theirs as the main source of your products.
I highly recommend : APS Pharmacy due to their great prices, high safety and sterilization compliance (I have visited their facilities) and customer care. For more information, email Anthony at anthony@apsmeds.com[image error]
April 21, 2012
Testosterone Research Studies Currently Looking for Patients
Those of you who want to help advance the understanding of testosterone use for different conditions can join research studies that are currently enrolling. I was amazed to see how many studies are out there! However, none are looking at long term management of side effects like polycythemia with therapeutic phlebotomy, testicular atrophy with long term or cycled HCG therapy, HPGA normalization protocols using HCG+Clomid+estrogen blockers, and other important modalities that are being used by many physicians but with little controlled data.Remember that some studies have placebo arms. Every study requires for you to read and sign a consent form that should clearly describe the risks and implications in joining the study. Make sure that the private investigator or research nurse overseeing the study explains things to you clearly.
Testosterone Research Studies Currently Looking for Patients

April 19, 2012
When Testosterone Replacement Doesn’t Lead to Better Erections
Excerpt from the book: Testosterone: A Man's Guide
Most men find that their sexual desire increases after they start testosterone replacement. Sexual dreams and nighttime/morning erections may be more easily achievable, but in some casestestosterone alone does not make erections strong or lastingenough for successful intercourse. So, some men need some extra help to make sure that their improvedsex drive matches an improved and hard erection.
Before we start coveringother options for improving erections, let’s talk about steps you should take before you start combination therapy of testosterone plus other options. If erectile dysfunction or sex drive is not improved while on testosterone, ask your doctorabout adjusting your dose of testosterone. Ensurethat your total testosterone level is between 500 and 1000 ng/dL. Also, have your doctor check your blood levels of estradiol and prolactin. High estradiol blood levels causedby conversion of testosterone into this female hormone by the aromatase enzymemay cause sexual dysfunction (this can be treatedwith low dose anastrazole). So is high prolactin's effect on erectile function. Low levelsof thyroid hormone, infections, lack of sleep, alcohol, smoking,medications and depression also can cause erectiledysfunction in the presenceof normal testosterone levels. Blood pressure medications are known to be one of the main causes of erectiledysfunction, so discuss the different type of medications to keep your blood pressurein normal ranges(high blood pressure is also a risk factor for erectiledysfunction). Last but not least, lack of attraction for our sexual partner can get in the way of achievinga strong erection.
If high estradiol of over 30 pg/dl is found (by ultrasensitive testing), then anastrozole at 1mg three times a week may be enough to bring it down to healthy levels. Remember that estradiol is important for men to keep healthy skin, hair, and brain function. High prolactin can be treated with cabergoline.
HCG - As mentioned before,human chorionic gonadotropin (HCG) mimics LH and stimulates the Leydig cells of the testicles to produce testosterone. HCG has been successfully used alone or in combination with testosterone replacement to normalize testicular size after long term anabolic steroid or testosterone use. It has also anecdotally helped men whose sexual drive does not improve on testosterone replacement alone.
No published studies have been done on this benefit,however. Doses of 250-500 IU twice a week while on testosterone replacement are being prescribed by several physicians who report that their patients perceive improvements in sexual desire and erectilefunction on this regimen. We do not know if this effect lasts afterlong term HCG use or if it is better to cycle it on and off.
PD-5 Inhibitors - For many older men the use of prescription phosphodiesterase type 5 inhibitor (PD-5) medications like Viagra, Cialis, and Levitra—may be needed in combinationwith testosterone replacement. However, somemen do not respond well to these oral agents or haveside effects such as headaches,nasal congestion, flushing,gut problems, and, inthe case of Cialis, back pain. Cialis may last longer than the others (36 hours compared to 4 hours for Viagra or Levitra), but so may its side effects. Some men take Claritin and ibuprofen with these drugs to pre-treat nasal congestion and headaches, respectively.
Sildenafil (Viagra) was the first PDE5 inhibitorto enter on the market in1998. The usual dose of sildenafil is 50 mg (25 to 100 mg) taken one hourbefore sex. The effects of sildenafil last for approximately four hours, and patients should be instructed to use no more than one dose within 24 hours. Fatty meals reduce the absorption of sildenafil; therefore, the drug should be taken on an emptystomach. This may be an inconvenient factor that needs careful planningof which some patientsare not aware.
Vardenafil (Levitra), the first second-generation PDE5 inhibitor to be developed, is given at a usual dose of 10 mg (2.5 to 20 mg) one hour before sex. Older men and those with moderate liver dysfunction should receive a lower initial dose of 5 mg. Vardenafil begins working within 30 to 45minutes after administration and lasts for about four hours. As with sildenafil, patients taking vardenafil should not use more than one dose within a 24-hour period. Patientsshould not take vardenafil withinthree hours of fatty meals, due to a reduction in absorption.
The newest PDE5 inhibitoris tadalafil (Cialis),which has a longer duration of action--approximately 36 hours--than sildenafil or vardenafil. In addition, the usual dose of 10 mg (5 to 20 mg) should be taken about 30 minutes before sexual activity. This shorteronset time can possibly allow patients more opportunity for spontaneity. Food intake does notappear to affect the absorption of tadalafil; this makes it very practical for men who donot plan ahead when they have sex. Cialis is approved for low dose daily use, but most insurance companies will not pay for it. If you want to try a 5 or 10 mg dose daily, you can get a free 30 day supply aftergetting a doctor’s prescription and taking the following voucherto your pharmacy after downloading it and printing it (you have to answer some questions online first). You are betteroff asking your doctorfor a prescription for 10 mg per day and cut the pills in half for the first week to see if 5 mg per day works well enough for you. If not, you can go up in dose.Here is the web site address to downloadthe voucher:
Free One Month Supply Voucher
Though considered generally safe for most patients,including those taking multipleantihypertensives, PDE5 inhibitors are not a viable treatment option for every man with ED. Theyneed to be used with careful monitoring in patientswith a cardiovascular history that includes heart attacks or stroke (withinthe past two weeks) and hypotension (blood pressure <90/50 mmHg),Because PDE5 is inhibited in penile tissue as well as extra genital tissue, patients treated with PDE5 inhibitors may experience headache, facial flushing, nasal congestion, dyspepsia, and dizziness. Sildenafil also inhibits PDE type 6 in the retina.Therefore, patients treatedwith sildenafil may experience sensitivity to light, blurred vision,and loss of blue-green color discrimination, all of which are generallyconsidered reversible. Tadalafilalso inhibits PDE type 11 in skeletal tissue,possibly leading to backand muscle pain.
ED drugsare available by prescription but I have heard that some men are ordering them without a prescription from overseas websites to save money (overseas sources can be ten times cheaper than products in the United States). This book does not endorse the use of these drugswithout a prescription, but it is my duty to mention facts about what is happening out in the real world. For a reviewof online sites that sell erectile dysfunction drugs, visit:
Review Online Pharmacies
The followingtable shows how long each commercially available PD-5 drug starts working and how long they stay in your body. This numbers vary depending on the amount of food or alcoholyou ingest beforetaking them, your body weight, and your liver metabolism.
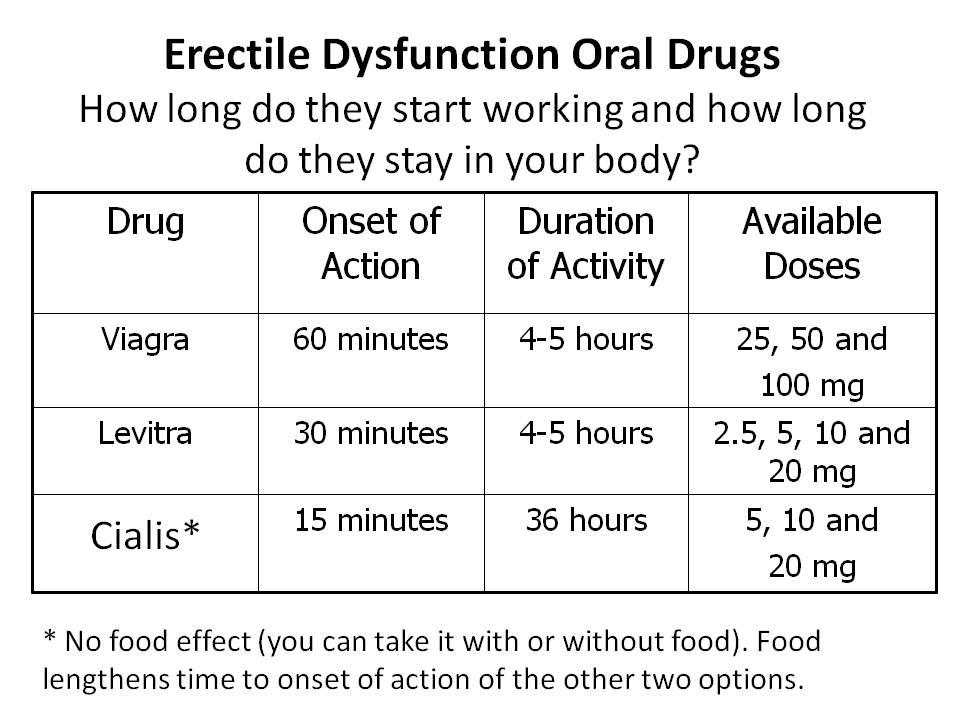
If you are older than age 65, or have serious liver or kidneyproblems, your doctor may start you at the lowest dose (25 mg) of Viagra or any of the other two drugs.
Tell your doctor about all the medicinesyou take. ED drugs and other medicines may affect each other. Especially tell your doctor if you take any of these:
• Medicines called alpha-blockers. These include Hytrin® (terazosin HCl), Flomax® (tamsulosin HCl), Cardura® (doxazosin mesylate), Minipress® (prazosin HCl), Uroxatral® (alfuzosin HCl), or Rapaflo® (silodosin). Alpha-blockers are sometimes prescribed for prostate problemsor high blood pressure. In some patients the use of PDE5 inhibitor drugs with alpha-blockers can lower blood pressure significantly, leading to fainting. You shouldcontact the prescribing physician if alpha-blockers or other drugs that lower blood pressure are prescribed by another healthcare provider
• HIV protease inhibitors including Ritonavir (Norvir®) or indinavir sulfate (Crixivan®), saquinavir (Fortavase® or Invirase®) or atazanavir (Reyataz®)• Antifungals like ketoconazole or itraconazole (such as Nizoral® or Sporanox®)
• Antibioticslike erythromycin or clarithromycin
• Tell your doctor if you take medicinesthat treat abnormal heartbeat. These include quinidine, procainamide, amiodarone, and sotalol.Patients taking these drugs should not use ED drugs.
If you are takingHIV protease inhibitors your doctor may recommend the lowest dose of each ED drug to start with and work your way up if the starting dose does not provide the desire benefits.Norvir, part of HIV protease inhibitor regimens, can boost blood levels of Ed drugsby slowing down the liver’s clearance of those drugs, so lower doses are needed to achieve the desired effect with the fewest side effects.
In rare instances, men taking PDE5 inhibitors have reported a sudden decrease or loss of vision. It is not possible to determine whether these events are related directlyto these medicines or to other factors. If you experience sudden decrease or loss of vision, stop taking PDE5 inhibitors and call a doctor right away.
Sudden decrease or loss of hearing has been rarely reported in people taking PDE5 inhibitors. It is not possible to determine whether these events are relateddirectly to the PDE5 inhibitors or to other factors. If you experience sudden decrease or loss of hearing, stop taking the oral ED drug and contact a doctorright away.
If you have prostate problems or high blood pressurefor which you takemedicines called alpha blockers, your doctor may start you on a lower dose of ED drugs.People who use recreational drugs called “poppers” like amyl nitrite and butyl nitrite should becareful while using ED drugs since a sudden decrease in blood pressure can occur.
Other options for men who need an extra erectile boost while using testosterone replacement:
Y ohimbine —Available over-the-counter or by prescription (Yocon); increases sex organ sensitivity. It can raise blood pressureand cause insomnia and anxiety, so talk to your doctor. A small study showed that men who used yohimbine with the amino acid argininehad better erections (read section on supplements in this book)
Muse (alprostadil )—this is a prescription pellet that insertsinto the urethra to produce an erection. Not very popular since some men do not respond well or are afraid to hurt themselves if they do not stick the pellet applicator carefully through the external urethralorifice of the penis head. You can ask your urologist for a sample with a training video that comes with it to see if this option is for you.
T rimix or Quadmix —Available by prescription from compounding pharmacies. These are mixtures of prostaglandins and papaverine that increase blood flow and retentioninto the penis. Prostaglandins are mediators and have a varietyof strong physiological effects, such as regulating the contraction and relaxation of smooth muscle tissue. Prostaglandins are not hormones and they are not producedat one discrete site, but ratherin many places throughout the human body.
Trimix is a mixture of two prostaglandins (phentolamine and alprostadil) plus papaverine (a vasodilator medication) that increase blood flow to the penis and cause strong and lastingerections, with or without sexual stimulation. These compounds appear to act together to increase arterial inflow, dilate smooth muscles,and restrict venous outflow promoting erectile rigidity with greatersuccess and in smaller doses than if these compounds were used as single therapies.
An example of a dosage combination for tri-mix is 10 microgramsof alprostadil, 500 microgramsof phentolamine and 15 mg of papaverine. Dosing of tri-mix preparations has notbeen standardized.
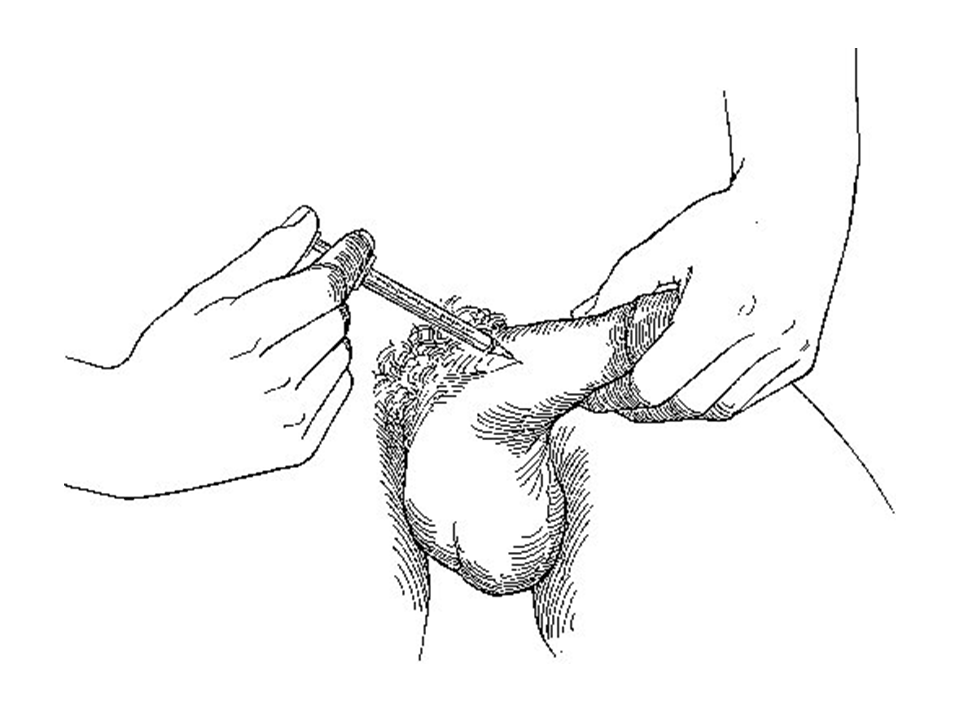
Trimix is injected directly into the side of the penis through a fine- gauge “insulin-style” needle in very small amounts (0.1-0.5cc) that increase bloodflow to the penis. It results in strong and lasting erections. The main potential side effect are hematomas(bruising), fibrosis if used toofrequently and on the same injection site,pain, and dangerously long-lasting erections(priaprism). Priaprism may sound great but this can literally kill your penis by causing gangrene of the tissue after stagnant blood coagulates inside it. I know men who had to go to an emergency room 8hours after having used too much Trimix and have the blood drained from their penis. To ensure perfect injection techniqueand dosing, it is imperative to be trained on how todose this with the help of an urologist.
Compounding pharmacies sell two types of Trimix formulations: Freeze dried (powder to be mixed later with water) or pre-mixed vials. Some men find the freeze dried form not to be as effective.
It is extremely important to remember never to use Viagra, Cialis, or Levitra before or at the sametime as you use Trimix. This is a dangerous combinationthat can increasethe risk of priaprism. Be particularly careful with Cialis since it can stay in your blood stream for a longertime. I know someone who had priaprism since he had forgotten he had taken Cialis two days before using Trimix.
Most men who use Trimix love it, even if they have had to learn the hardway about priaprismduring one instance.Most of these men did not respond well nor had too many side effects to oral agents like Viagra or Cialis.
For instructions on how to inject Trimix, read:
Instructions and general information about Trimix
For instructions for physicians on how to treat priaprismin the unfortunate case that it happens:
Priapism in Emergency Care
A 10 cc bottle of Trimix can cost from $70 to $100 in compounding pharmacies. If a dose of 0.15 cc is needed per erection, this bottle can be good for 67 erections. In comparison with Cialis and Viagra($16 a pill), this option seems economical. APSMeds.com has good prices, quality control and customer service, and can ship to your home.
You will need a prescription written as : TRIMIX (10 micrograms of alprostadil, 500 micrograms of phentolamine and 15 mg of papaverine) , 5 mls, as directed. Make sure you ask for insulin syringes (30 gauge, 1 inch needles), and alcohol swabs with your order.
Caverject — This is an injectable form of alprostadil. Injections of alprostadil have been reported to cause pain, bleeding, hematomas and scar tissue leading to Peyronie’s Disease (excessive curvature of the penis) in some patients. Caverjet is available by prescription and it is nota compounded product,so some doctorswho are not comfortable prescribing compounded products feel more at ease prescribing it. However, it is not as effective as Trimix, it requires a large injection volume, and it comes preloaded in syringes with thick needles. It is also10 times more expensive than Trimix but severalinsurance companies pay forit (Trimix is rarely covered by insurance). This injection into the penis that produces an erectionthat can last 1 to 2 hours. Followinstructions from your urologist since overdosing can also cause priaprism.
For the best treatmentalgorithm for physicians who want to learn more about how to prescribe, dose and manage injectable ED drugs like Trimix,Caverjet and other formulations, this article is probably the most comprehensive. It was written by Jeffrey A.Albaugh, who is an Advanced Practice Urology Clinical Nurse Specialist at Northwestern Memorial Wellness Institutein Chicago (source:Urol Nurs. 2006;26(6):449-453. © 2006 Society of Urologic Nurses and Associates ) :

Penile restriction rings —these rubber or leatherrestricting bands (commonly known as “cock rings”) can be very effective at maintaining erections after the penis fills up with blood. Be careful not to use it too tight. Neoprene and leather rings are the most common. Theycan be found online.


Other options are penile vacuum devices and penile implants. Due to the scope of this book, these two options will not be reviewed. Plenty of information can be found by Googling those terms.

It is estimated that some degreeof ED affects half of all men over theage of 40 and that 150 million men worldwidesuffer from ED. Up to 35% of men with ED are non-responsive to standard therapieswith phosphodiesterase-5 inhibitors, representing an estimated marketof $500 to $600 million per year. So, there is a huge interest from pharmaceutical companies to keep researching new drugs in this field.
Out of many that are being tested, there are about 4 new erectile dysfunction medications that have made it through several clinical trials and many of them are in the final stages of being approved. The ED market is an extremely competitive field. Viagra will lose its patentin 2012 and genericversions will become widely available. Whether this will mean that Viagra will be cheaperin the United States then is yet to be seen. Manydrugs have become generic and yet their prices do not drop when that happens.
Medications that could cause decreased sex driveor erectile dysfunction:One reason that testosterone may not lead to better erections and sex drive is the use of medications that may interfere with those two benefits.
A great review of all studies of drugsthat affect sexual functionin men was provided by Dr. Walter K.H. Krause in his book “Drugs Compromising Male Sexual Health”.He was able to identifyevidence from different studies (many uncontrolled and small) about the common classes of prescription medications that can cause erectile dysfunction. It isnot known if testosterone replacement can counteractthe effects of these medication classes. Among the medications are:
• Antidepressants: Selective serotonin reuptake inhibitors (SSRIs), tricyclic antidepressants, monoamineoxidase inhibitors
• Blood pressure medications (antihypertensives): Alpha andregenergic antagonists, beta-blockers, diuretics, guanethidine, methyldopa
• Narcoticsand opiates
• Barbiturates and benzodiazepines
• Hormone relatedproducts: Anabolic steroids, antiandrogens used in prostate cancer, estrogens,medroxyprogesterone, 5-alpha- reductaseinhibitors (Proscar, Propecia)
• Anti-acids: Histamine2 receptor antagonists (Tagamet), proton pump inhibitors (Prilosec)
• Cholesterol–lowering agents: Bile acid sequestrants, fenofibrates(Tricor, etc), statins(Lipitor, etc)
For more information, read Testosterone: A Man's Guide[image error]
April 18, 2012
Top Selling Testosterone Book Helps Men Improve Their Vitality

Houston, TX (PRWEB) April 18, 2012“Testosterone: A Man’s Guide- Practical Tips for Boosting Physical, Mental and Sexual Vitality” (Milestones Publishing, available on amazon.com) has been recently published to educate men about testosterone deficiency, its symptoms, diagnosis and treatment, with practical "how-to" information generated by an empowered patient and treatment advocate after 20 years of research.
The overall prevalence of testosterone deficiency (hypogonadism) in the United States is approximately 39 percent in men 45 years or older according to the 2006 Hypogonadism in Males (HIM) study, one of the largest studies ever done on testosterone deficiency. Recent estimates show that 13 million men in the United States may experience testosterone deficiency, although fewer than 10 percent receive treatment for the condition. So why are so few men receiving treatment for hypogonadism? This alarming low rate is not surprising since most men feel awkward about talking to their doctors about the two main symptoms of testosterone deficiency: depression and sexual dysfunction. And when they do, sometimes they encounter resistance from doctors that are not well trained in managing testosterone replacement therapy.
“What Nelson Vergel has done is to distill difficult-to-find medical information in simple terms for anyone to understand and apply it to their health,” said Dr. Shannon Schrader, a well known physician in Houston. “It is rare to have self-empowered patients become experts and advocates who then make it easier for everyone to learn from their experiences. Nelson has been doing that for 20 years and now he packages his experiences to help men to get a better understanding of testosterone,” added Dr Schrader.
“There are several books on testosterone written by doctors that are too medical or not practical enough for patients,” said Fred Walters, founder of the Houston Buyer’s Club, a nutritional supplement company. "As patients, we have been waiting for someone like Nelson to give us practical information on this important subject in layman’s terms. I am glad that he has been able to save many of us time and costly mistakes when navigating through the complex issues of testosterone replacement. He is living proof of his work,” added Walters.
“In my work as a lecturer and patient advocate, it has amazed me to see so many men suffer needlessly for years before finding out that their physical and sexual fatigue could be reversed easily by the safe use of testosterone,” said Nelson Vergel. “I hope my book clarifies fears that men and their physicians have about testosterone causing prostate cancer, liver problems, rage, and other side effects that have yet to materialize in any research studies”
If are you or someone you know having these problems: Fatigue and low or no sex drive?Less mental focus?Less tolerance to stress and feel down?Fat gain and muscle lossNo improvements in body after exercising for monthsAre afraid of testosterone replacement due to lack of informationThen, this book may help.
This book will explain in clear and practical language the symptoms and treatments of testosterone deficiency to help determine if you are a good candidate for this therapy. Testosterone replacement therapy (TRT) can dramatically boost sex drive and function, strength, energy levels, mood, mental focus, and lean body mass while decreasing fat in men with testosterone deficiency syndrome (hypogonadism). However, it is not a therapy to start without proper knowledge about potential side effects and their management. There are several options for testosterone replacement available by prescription but many men do not know how to decide which is best for them. This book reviews all options from the author’s point of view as an educated patient who has used all available options and has researched the current scientific data. Al myths and misconceptions surrounding testosterone are fully explained and resolved.
After reading this book you will know:If you have low testosterone blood levelsWhat your best TRT option is more suitable for you, if you need one.How to avoid the main mistakes that men make when using TRTHow to identify and treat potential side effects before they become a problemHow to talk to your doctor about getting TRT, or how to find a doctor who prescribes testosteroneWhat foods and medicines can lower your testosteroneThe truth about non-prescription testosterone boostersHow to apply for financial assistance from testosterone manufacturersWhat compounding pharmacies are and how they can customized TRT options for youAbout the author: Nelson Vergel, BsChE, MBA, is practicing what scientists can only theorize. He started testosterone replacement therapy in 1993 as a desperate attempt to survive and overcome wasting syndrome. Testosterone gave him his health back which propelled him to become an expert on its use. After years of trial-and-error and self-empowerment, he is ready to share his knowledge with the world. With a chemical engineering degree, countless of hours in scientific conferences and memberships in several metabolic research and wellness groups, he was been able to digest scientific information on the subject to translate it in layman’s terms for all to benefit. He is the co-author of the book “Built to Survive: A Comprehensive Guide to the Medical Use of Anabolic Therapies, Nutrition and Exercise for HIV+ Women and Men” and the founder the non-profit organizations Program for Wellness Restoration (PoWeR) and the Body Positive Wellness Clinic in Houston, Texas. He has given over 700 lectures in English and Spanish in the United States and abroad about testosterone, nutrition, exercise, aging, and general wellness to men and women.
For updates on this book and to join Nelson’s email list, visit http://www.TestosteroneWisdom.com[image error]
Spanish Translation: Monitoreando la Terapia de Reemplazo de Testosterona
Este capitulo fue extraido del libro "La Testosterona" (puede ser comprado en www.testosteronewisdom.com o en amazon.com)
El primer paso para la correcta evaluación de la terapia de reemplazo es facilitarle a su médico un historial médico minucioso. . Los pacientes que deseen ser proactivos, pu- eden llevar este formulario y entregarles una copia a sus médicos.Se es- pera que cada médico tenga un formulario similar, aunque la mayoría de ellos no formulan preguntas relacionadas con la funciónsexual o el uso de andrógenos. Hágale saber a su médico acerca de todos los medicamentos que toma para poder descartar la disfunción sexualinducida por fármacos antes de iniciar la testosterona.También considerofirmemente que si un paciente acudeal médico para obtener una prescripción de Viagra, Cialis o Levitra, el médico debería revisar los niveles de testosterona en la sangre del paciente para asegu- rarse que esa no es la raíz del problema.Es probable que los hombres hipogonadales no respondan muy bien a estos medicamentos si no se nor- malizanprimero sus nivelesde testosterona. Los estudios que combinan la testosterona y fármacos orales para aumentarla sexualidad han mostrado efectos sinérgicos en beneficios sexuales.Los siguientes consejospara evaluar el reemplazode testosterona son recomendados por varios grupos de médicosy practicantes:
1. Usteddebería ser evaluadodespués del primermes de terapia para medir sus niveles de testosterona en la sangre.Si su médico no le pre- gunta, hágale saber usted sobre su calidadde vida. Asegúrese que su médico esté al tanto de sus niveles de energía, humor y función sexual, así como también cualquier efecto secundario potencial (mamas sen- sibles, disminución en el flujo urinario, malhumory acné).2. Cuandoesté usando testosterona, su médico querrámedir sus niveles de testosterona total en la sangre justo antes de la próxima inyección correspondiente después del primer mes (toma tiempo para que los niveles sanguíneos se estabilicen). Si la testosterona se encuentra>70 ng/dl (24,5 nmol/litro) ó <350 ng/dl(12,3 nmol/litro), su médico ajustará la cantidad o la frecuencia de su dosis. Mencioné esto previa- mente en el libro, pero es necesariorepetirlo aquí: Algunoshombres necesitan niveles por encima de 500 ng/dl para poder experimentar cualquiera de losbeneficios sexuales que se espera de la testosterona. Es importante ser honesto cuandosu médico le pregunte sobre su de- sempeño sexual.3. Su médico revisarásus hematocritos antes de iniciar la testosterona, después de 3 meses y luego cada año después de eso. Si sus hematocri- tos están por encima de 54%, puede que usted necesiteuna flebotomía terapéutica (lea la sección“Revisando el Incremento del Espesor de la Sangre (Policitemia)” para mayores detalles).4. Estépreparado para hacerseun examen rectal digital y un examen sanguíneo de antígeno prostático específico (APE) antes de iniciarla testosterona, y repetirlo a los 3 meses. No sería irracional realizarlo también una vez cada 6 meses, especialmente en hombres mayores. Un APE por encima de 4 ng/ml puede ser razón para preocuparse y referirlo a un urólogo.Si se observa un incremento en los niveles de APE encima de lo normal, es necesariodetener el reemplazo de tes- tosterona. Nota: al inicio del reemplazo de testosterona en hombres mayores, cuando los nivelesde testosterona están en rápido aumento, también es probableque incremente el APE. Esto sucede especial- mente cuando se empleangeles de testosterona, ya que elevanla DHT más que las demás opciones. Una vez que se hayan estabilizado los niveles de testosterona, el APE disminuyecasi hasta el valor base. Es importante esperar hasta alcanzar un “estado seguro”después de las fluctuaciones dela testosterona antesde medir el APE; un mes aproxi- madamente debería ser suficiente.5. Si usted comienzaa experimentar sensibilidad, dolor o crecimiento en las mamas, pídale a su médico que mida su nivel de estradiol en sangre realizando un análisis sensible(no el examen regular usado para mujeres). El valornormal de estradiol en hombres es 14-54 pg/ml (20-200 pmol/litro). Los hombres que presenten alto estradiol pueden ser tratados con inhibidores del receptor de estrógeno (más detalles en “Evitando el agrandamiento de mamas (ginecomastia)”).[image error]
April 17, 2012
New Study: Lack of a Full Night's Sleep Can Make You Fat
Source (click here)
"Disturbed sleep resulted in a 27 percent average decrease in insulin secretion after eating, and higher glucose levels over a longer period of time, sometimes high enough to make the subject prediabetic. In addition, there was an average 8 percent decrease in resting metabolism rate, a measure of how much energy the body consumes at rest, that translates into a theoretical weight gain of more than 12 pounds a year."
Previous studies also linked interrupted or poor sleep to higher cortisol blood levels, which was thought to explain some of the weight gain. It has also been speculated that those who keep late hours to go to sleep tend to overeat at night. But this study actually measured insulin response and blood sugar in those who had interrupted sleep and saw a dramatic decrease in insulin's effectiveness at controlling blood sugar.
So, to keep from gaining weight, it is not only important to eat healthy and exercise, but to try to get a full night sleep every night. [image error]
"Disturbed sleep resulted in a 27 percent average decrease in insulin secretion after eating, and higher glucose levels over a longer period of time, sometimes high enough to make the subject prediabetic. In addition, there was an average 8 percent decrease in resting metabolism rate, a measure of how much energy the body consumes at rest, that translates into a theoretical weight gain of more than 12 pounds a year."
Previous studies also linked interrupted or poor sleep to higher cortisol blood levels, which was thought to explain some of the weight gain. It has also been speculated that those who keep late hours to go to sleep tend to overeat at night. But this study actually measured insulin response and blood sugar in those who had interrupted sleep and saw a dramatic decrease in insulin's effectiveness at controlling blood sugar.
So, to keep from gaining weight, it is not only important to eat healthy and exercise, but to try to get a full night sleep every night. [image error]
April 16, 2012
Testosterone Replacement Decreases Mortality in a VA Cohort
From: The Endocrine Society
AbstractContext: Low testosterone levels in men have been associated with increased mortality. However, the influence of testosterone treatment on mortality in men with low testosterone levels is not known.Objective: The objective of the study was to examine the association between testosterone treatment and mortality in men with low testosterone levels.Design: This was an observational study of mortality in testosterone-treated compared with untreated men, assessed with time-varying, adjusted Cox proportional hazards regression models. Effect modification by age, diabetes, and coronary heart disease was tested a priori.Setting: The study was conducted with a clinical database that included seven Northwest Veterans Affairs medical centers.Patients: Patients included a cohort of 1031 male veterans, aged older than 40 yr, with low total testosterone [≤250 ng/dl (8.7 nmol/liter)] and no history of prostate cancer, assessed between January 2001 and December 2002 and followed up through the end of 2005.Main Outcome Measure: Total mortality in testosterone-treated compared with untreated men was measured.Results: Testosterone treatment was initiated in 398 men (39%) during routine clinical care. The mortality in testosterone-treated men was 10.3% compared with 20.7% in untreated men (P<0.0001) with a mortality rate of 3.4 deaths per 100 person-years for testosterone-treated men and 5.7 deaths per 100 person-years in men not treated with testosterone. After multivariable adjustment including age, body mass index, testosterone level, medical morbidity, diabetes, and coronary heart disease, testosterone treatment was associated with decreased risk of death (hazard ratio 0.61; 95% confidence interval 0.42–0.88; P= 0.008). No significant effect modification was found by age, diabetes, or coronary heart disease.Conclusions: In an observational cohort of men with low testosterone levels, testosterone treatment was associated with decreased mortality compared with no testosterone treatment. These results should be interpreted cautiously because residual confounding may still be a source of bias. Large, randomized clinical trials are needed to better characterize the health effects of testosterone treatment in older men with low testosterone levels.[image error]
How to Prevent Heart Attacks if You are Using Testosterone
Testosterone and anabolics can increase red blood cells. The proportion of red blood cells in the blood is called hematocrit. High hematocrit (polycythemia) can make blood viscous and increase the work load on the heart, which can cause serious cardiovascular problems and even heart attacks and strokes. So, it is important to monitor hematocrit and know how to manage it if it is high. Preventing and Managing Polycythemia
From:Testosterone: A Man's Guide
It's important to check patients' hemoglobin and hematocrit blood levels while on testosterone replacement therapy. As we all know, hemoglobin is the substance that makes blood red and helps transport oxygen in the blood. Hematocrit reflects the proportion of red cells to total blood volume. A hematocrit of over 52 percent or a hemoglobin value over 19 g/dl should be evaluated. Decreasing testosterone dose or stopping it are options that may not be the best for assuring patients' best quality of life, however. Switching from injectable to transdermal testosterone may decrease hematocrit, but in many cases not to the degree needed.
The following table shows the different guideline groups that recommend monitoring for testosterone replacement therapy. Since hematocrit increases usually happen during the first few months of testosterone replacement, all guideline groups agree on measuring hematocrit at month 3, and then annually, with some also recommending measurements at month 6 after starting testosterone.
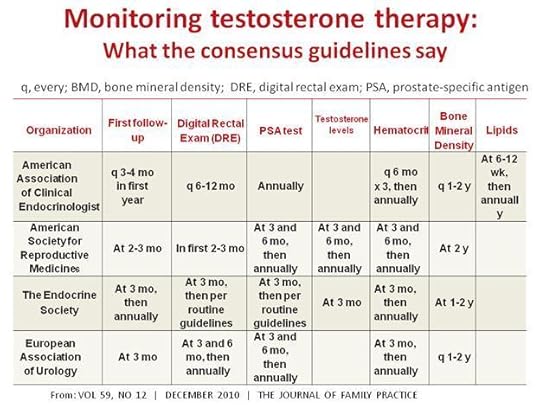
Many patients on testosterone replacement who experience polycythemia do not want to stop the therapy due to fears of re-experiencing the depression, fatigue and low sex-drive they had before starting treatment. For those patients, therapeutic phlebotomy may be the answer. Therapeutic phlebotomy is very similar to what happens when donating blood, but this procedure is prescribed by physicians as a way to bring down blood hematocrit and viscosity.
A phlebotomy of one pint of blood will generally lower hematocrit by about 3 percent. I have seen phlebotomy given weekly for several weeks bring hematocrit from 56 percent to a healthy 46 percent. I know physicians who prescribe phlebotomy once every 8-12 weeks because of an unusual response to testosterone replacement therapy. This simple procedure is done in a hospital blood draw or a blood bank facility and can reduce hematocrit, hemoglobin, and blood iron easily and in less than one hour. Unfortunately, therapeutic phlebotomy can be a difficult option to get reimbursed or covered by insurance companies. The reimbursement codes for therapeutic phlebotomy are CPT 39107, icd9 code 289.0.
Unless a local blood bank is willing to help, some physicians may need to write a letter of medical necessity for phlebotomy if requested by insurance companies. If the patient is healthy and without HIV, hepatitis B, C, or other infections, they could donate blood at a blood bank (it is good to remember that there is a ban on gay blood donors in the United States, however).
The approximate amount of blood volume that needs to be withdrawn to restore normal values can be calculated by the following formula, courtesy of Dr. Michael Scally, an expert on testosterone side effect management. The use of the formula includes the assumption that whole blood is withdrawn. The duration over which the blood volume is withdrawn is affected by whether concurrent fluid replacement occurs.
Volume of Withdrawn Blood (cc)=
Weight (kg) × ABV×[Hgbi - Hgbf]/[(Hgbi +Hgbf)/2]
Where:
ABV = Average Blood Volume (default = 70)
Hgbi (Hcti) = Hemoglobin initial
Hgbf (Hctf) = Hemoglobin final (desired);
So, for a 70 kg (154 lbs) man (multiply lbs x 0.45359237 to get kilogram) with an initial high hemoglobin of 20 mg/mL who needs to have it brought down to a normal hemoglobin of 14 mg/mL, the calculation would be:
CC of blood volume to be withdrawn = 75 x 70 x [20 - l4]/[(20 + l4)/2] = 75 x 70 x (6/17) = approximately 1850 cc;
One unit of whole blood is around 350 to 450 cc; approximately 4 units of blood need to be withdrawn to decrease this man's hemoglobin from 20 mg/mL to 14 mg/mL.
The frequency of the phlebotomy depends on individual factors, but most men can do one every two to three months to manage their hemoglobin this way. Sometimes red blood cell production normalizes without any specific reason. It is impossible to predict exactly who is more prone to developing polycythemia, but men who use higher doses, men with higher fat percentage, and older men may have a higher incidence.
Some doctors recommend the use of a baby aspirin (81 mg) a day and 2,000 to 4,000 mg a day of omega-3 fatty acids (fish oil capsules) to help lower blood viscosity and prevent heart attacks. These can be an important part of most people's health regimen but they are not alternatives for therapeutic phlebotomy if the patient has polycythemia and does not want to stop testosterone therapy. It is concerning that many people assume that they are completely free of stroke/heart attack risks by taking aspirin and omega-3 supplements when they have a high hematocrit.
Although some people may have more headaches induced by high blood pressure or get extremely red when they exercise, most do not feel any different when they have polycythemia. This does not make it any less dangerous. It may be a silent killer that is easy to prevent.
[image error]
April 13, 2012
Propecia and Proscar Cause Sexual Dysfunction, the FDA says
The FDA made a few changes to Propecia and Proscar which include:
a revision to the Propecia label to include libido disorders, ejaculation disorders, and orgasm disorders that continued after discontinuation of the drug,a revision to the Proscar label to include decreased libido that continued after discontinuation of the drug, anda revision to both the Propecia and Proscar labels to include a description of reports of male infertility and/or poor semen quality that normalized or improved after drug discontinuation.More : Finasteride causes sexual problems in men[image error]
a revision to the Propecia label to include libido disorders, ejaculation disorders, and orgasm disorders that continued after discontinuation of the drug,a revision to the Proscar label to include decreased libido that continued after discontinuation of the drug, anda revision to both the Propecia and Proscar labels to include a description of reports of male infertility and/or poor semen quality that normalized or improved after drug discontinuation.More : Finasteride causes sexual problems in men[image error]


