
Aaron E. Carroll's Blog, page 143
March 7, 2017
Healthcare Triage: Wearable Tech Probably Won’t Help You Lose Weight
I once received a lot of blowback for an Upshot article in which I showed (with evidence) that exercise is not the key to weight loss. Diet is. Many, many readers cannot wrap their head around the notion that adding physical activity, and therefore burning more calories, doesn’t necessarily translate into results on the scale.
Well, here we go again because some of those folks also believe that fitness devices — Fitbit, Vivosmart, Apple Watch — must be helpful in losing weight. Unfortunately, evidence doesn’t support this belief either.
That’s the topic of this week’s Healthcare Triage.
This episode was adapted from a column I wrote for the Upshot. Links to further reading and sources can be found there.


The Republicans’ “American Health Care Act” in a few words as I can manage
The repeal and replace bill is here: The American Health Care Act. There will be a gazillion explainers, and that’s not my goal here. I’m trying to describe the bill in a few words as I can manage, to make a Healthcare Triage script. So here is my attempt. I’m going to leave comments open, and I encourage you to tell me where I’m wrong or missed something. I don’t tape until tomorrow. You can also tweet me suggested changes. Text of the bill here.
Medicaid
Medicaid is complicated. First of all, the bill leaves the expansion intact – for now. Everyone who signs up by 2020 gets to keep their Medicaid. But in that year, entry into the expansion is frozen, and people will only remain eligible if they don’t have a lapse in coverage of more than a month.
In some ways, this bill incentivizes states to sign up as many people as possible in the next three years, so that they qualify for a higher match amount when that goes into effect in 2020.
In 2020, we change Medicaid to a per capita block grant program. The cap rises by medical CPI plus 1%. The initial rate will be set by looking at 2016, and then increasing spending to 2019 based on that formula. That could lead to a drop in relative funding in 2020 if health care spending increases faster than inflation from now until 2020.
The amount allocated per person is based on five groups: (1) kids, (2) the elderly, (3) blind and disabled people, (4) previously eligible adults (pregnant women, parents), and (5) expansion eligible (working adults).
Lottery winners are not eligible for Medicaid. They spent a full six pages of the bill discussing this. I have no idea why.
The essential health benefits requirement for some Medicaid benchmark plans goes away. This seems to include the requirement that mental health services be covered the same as other health benefits.
Retroactivity changed. As of now, you can get Medicaid today and get it cover your spending for up to three months ago. This is important, because people could get coverage for things that occurred for some time before they signed up. That’s now reduced to the month in which they apply. Huge deal.
Additionally, now states have to re-determine eligibility for people on Medicaid at least every six months. This will lead to many people losing coverage, cause that’s much more of a pain than you think.
Other Payments
Disproportionate hospital payments are restored immediately to states that didn’t expand Medicaid, and to all states in 2020.
In 2018 and 2019, $15 billion is allocated for states to do with what they want. They could make high-risk pools. Or they could increase the size of the subsidies/tax credits. Or they could reinsure insurers to protect them from really high-cost patients.
From 2020 through 2026, that amount is reduced to $10 billion a year. To claim that money, states have to match in in increasing amounts, from 7% in 2020 to 50% in 2026.
Subsidies
Anyone who maintains continuous coverage will keep their community ratings – they can’t be charged more than others. If, however, they let their coverage lapse for 63 days in a year, they can be charged 30% more for 12 months.
The subsidies change, too. Now. They’re called tax credits. (Here’s a secret – they were tax credits before). But now they’re not based on how much you earn; they’re based on how old you are.
They also start to phase out when you earn $75,000 a year ($150,000 for joint tax filers).
As you can see from this handy chart from the KFF, a 27-year-old will get $2000, a 40-year-old will get $3000, and a 60-year-old will get $4000. That’s true if they make $20,000 or $75,000. Under the ACA, they got more money if they were poorer, and less if they were richer. Those making $75,000 get nothing now, for instance.
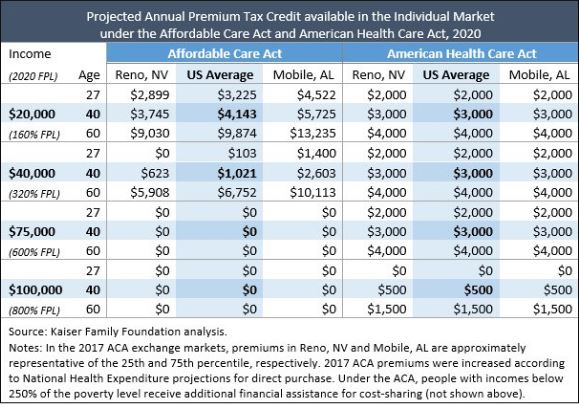
This means that poorer people, especially non-young poorer people, are going to have a much harder time affording insurance. People making more, ironically, are potentially in for a windfall.
Cost sharing subsidies are not appropriated for 2017, 2018, or 2019 – and they’re eliminated in 2020. Your subsidies also can’t be used to purchase any insurance that covers abortion.
The exchange market
There’s no more individual mandate or employer penalty – retroactive to 2016. Insurance companies will hate that. This will likely lead to adverse selection. That’s made worse ironically by the 30% penalty for late enrollment. Healthy people, once they’re out, simply won’t buy coverage until they’re sick – cause you’ll get the same penalty no matter what. Death spirals seem much more likely with this plan.
Age bands (the difference between what you can charge young and older people for insurance) are increased from 3:1 to 5:1 starting in 2018. This will make insurance cheaper for younger people and more expensive for older people.
Taxes
For 2017, all the taxes remain in effect. In 2018, though, they’re gone. This includes the Cadillac tax (delayed until 2025, which is the same thing), the medical device tax, the tax on high salaries of insurance executives, the Medicare tax on higher earners, taxes on insurance companies, pharma, and tanning salons, etc.
Misc.
The bill defunds Planned Parenthood, bur increases funding for community health centers.
People could now put even more money into their health savings accounts. The limit increases to at least $6,550 for an individual and $13,100 for a family in 2018.
What’s untouched?
Young adults can are still covered by family plans until they are 26.
Guaranteed issue and community ratings still exist (subject to continuous coverage).
Essential health benefits remain intact in the exchange market, including preventive services and maternity care.
Annual and lifetime limits are still banned.
My thoughts
There’s no CBO score yet, and it’s hard to know exactly what they find. But here are my thoughts: it’s hard to see how this won’t lead to a reduction in insurance coverage. Many people will find the subsidies insufficient to buy care.
It’s also hard to see how it will lead to much of a deficit reduction in the long term. There’s still a decent amount of spending in there and a declaration that many of the taxes/sources of revenue will end. That’s unless they plan deep, deep cuts to Medicaid in the future – which will come with its own issues.
I’m actually worried that their continuous coverage plan could actually make adverse selection worse. Why wouldn’t a healthy person go without insurance for a couple years if all they’re gonna see is a one year 30% increase in premiums as a penalty?
There’s a fair argument to be made that this is Obamacare Lite. There’s still a fair amount of regulation, the expansion is left intact until 2020, subsidies still exist – even the taxes don’t go away yet. But this is still a big difference from the ACA. The subsidies shift away from the poor to others. And Medicaid undergoes a huge sea change in 2020.
It’s a bill. It desperately needs a CBO score.
March 6, 2017
Social democracy and free speech in the university
On March 2nd, a crowd prevented the conservative writer Charles Murray from speaking at Middlebury College. They injured a professor trying to escort Murray away from the event. This is wrong and it’s important to understand why.
Tim Carney makes two points about these events. First, he suggests that suppression of free speech is consistent with if not required by social democratic politics. This couldn’t be farther from the truth. Second, he argues that academic communities like Middlebury should function according to norms of “civility, tolerance, and freedom to disagree”. Here he is completely right.
Social democracy is a loosely defined concept with a complex history, but briefly: social democrats affirm democratic institutions, capitalist economies, and a redistributive welfare state. Among the most important writers in the tradition are J. S. Mill and John Rawls, the leading English-speaking political philosophers of the 19th century and 20th centuries. Both writers championed civil liberties.
Mill wrote On Liberty, the most famous philosophical defence of free speech. If we seek truth, Mill argued, we must support open discourse.
In the case of any person whose judgment is really deserving of confidence, how has it become so? Because he has kept his mind open to criticism of his opinions and conduct. Because it has been his practice to listen to all that could be said against him; to profit by as much of it as was just, and expound to himself, and upon occasion to others, the fallacy of what was fallacious. Because he has felt, that the only way in which a human being can make some approach to knowing the whole of a subject, is by hearing what can be said about it by persons of every variety of opinion, and studying all modes in which it can be looked at by every character of mind. No wise man ever acquired his wisdom in any mode but this; nor is it in the nature of human intellect to become wise in any other manner.
Rawls is most famous for his doctrine of justice as fairness. But this was not, in his view, the most important principle of justice. Rawls subordinated his egalitarianism to the principle that:
each person is to have an equal right to the most extensive basic liberty compatible with a similar liberty for others.
According to Rawls, the basic liberties include freedom of speech. The left should never forget that its first principle is democracy.
It’s easy to endorse these principles, but it’s challenging to create and sustain institutions that embody free speech norms. The difficulties come from hard cases where principles collide. For example, suppose a student group wanted to fly Nazi banners from their dorm room windows. This is speech, but it expresses a desire to exclude or intimidate other students. In my view, a university ought to have such banners taken down. Now suppose there was a history seminar on the Holocaust and one of the Nazi students argued that the event never happened. In my view, the professor would be right to fail him: the student is wrong on the facts. But it would wrong to expel the student from the class. The Holocaust is the topic at hand and in this setting the student has the right to state his view.
The Middlebury events, however, came nowhere near the borders of such hard cases. Murray had an invitation to speak from a legitimate student group. There is no report that Murray said anything that can be construed as hate speech. I strongly disagreed with Murray’s book The Bell Curve, which argued that genetic determination of social structure made social policy futile (see James Heckman’s devastating review of the book in the Journal of Political Economy). But that disagreement would be a reason for me to, say, vote against him if he were proposed for a lectureship in my department. It’s not a justification for shouting him down if he were giving the lecture.
I hear the claim that the threat of fascism justifies violence. While we still have a democracy, this is doubly wrong. On the one hand, violence to inhibit speech is antithetical to democracy. As such, violence communicates exactly the wrong message about who we are on the left. On the other hand, the norms and institutions of free speech are part of our defence against tyranny. In the Trump era, I am astonished that anyone could lose sight of this last point.
Healthcare Triage News: Are Beta-Blockers Useful in the Elderly after a Heart Attack?
Should we use beta-blockers in the elderly after they have a heart attack? It just got more complicated. This is Healthcare Triage News.
March 2, 2017
AcademyHealth: Increasing evidence that sugar-sweetened beverage taxes work
I know I’ve been down on soda bans, but taxes are another story. In Mexico, not only did a sugar-sweetened beverage tax work, it appears to be working more as time goes on.
Go read more about that in my latest post over at the AcademyHealth blog!
March 1, 2017
Healthcare Triage: How to Give Better Medical Advice
Medical scientists and academics must publish their research to advance. Medical organizations must release health recommendations to remain relevant. News organizations feel they must report on research and recommendations as they are released. But sometimes it’s hard to separate what’s truly a medical certainty from what is merely solid scientific conjecture.
That’s the topic of this week’s Healthcare Triage.
This episode was adapted form a column I wrote for the Upshot. Links to sources and further reading can be found there.
Help me learn new skills in 2017 – Meditation!
This post is part of a series in which I’m dedicating two months to learning six new skills this year. The full schedule can be found here. This is month one/two. (tl;dr at the bottom of this post)
I’ve tried to meditate before. Before this year, I’d maybe made it for a few days at most before losing track and giving up. I’d even tried Headspace before but never got past the third day.
I’ve never been opposed to meditation. It’s not that I’ve been disdainful towards it, or thought it was a waste of time. It was just that I didn’t prioritize it or give it enough weight in my day to make sure I did it.
It may surprise many of you, but I am a huge consumer of self-help books. I’ve read many and found a few gems. About a year or two ago, I came across Dan Harris’s book 10% Happier. It was a revelation. He described meditation in a way that I could appreciate. It wouldn’t work miracles. It wouldn’t end my mental neuroses or issues. But it might make me ten percent happier.
It has.
I committed to doing this every day, and one of the great things about this series is that when I commit to the blog, I prioritize making it happen. I started with the Headspace base pack, for 10-minute sessions at a time. When I cleared the first ten, I upped the time to 15 minutes for the second. When I started the final 10-day base pack, I increased the sessions to 20 minutes.
If you had told me months ago that I could somehow sit still and not do anything for 20 minutes, I would have laughed in your face. After that, I tried out the packs on “patience” and “acceptance”. Both were helpful.
I should be clear that I’m pretty clinical about meditation. I don’t feel very spiritual about it. I didn’t have gratitude-moments or any real breakthroughs. I had no out-of-body experiences and didn’t advance to any other planes of existence.
That doesn’t mean I didn’t succeed. I found that the most important thing was committing to 15-20 minutes every day without fail. There have been any number of benefits. These include, but are not limited to:
I have learned that my active, thinking mind is not nearly as helpful as I think. I might have sometimes found it entertaining to have arguments in my head while I shower or drive, but they only seem to rile me up and never lead to resolutions.
I have learned to quiet my mind. By that, I mean I recognize when I’m not present, I can note “that’s thinking”, and I can bring myself back to the moment.
I spend a day or two in Disneyland recently. I found that I could wait in the lines much more easily. I didn’t get impatient. I didn’t get frustrated. I could recognize the symptoms and return my focus to breathing for a minute or two, and that helped a lot.
When I’m on the elliptical machine, the time goes much faster. I can focus more easily on the show I’m watching and not be in my head about the time.
I find it easier not to get into arguments with my kids or with my wife. I’m not perfect, by any means. But I can see when there are potential issues brewing and I can choose not to engage or go there. I’ve noticed a difference even if no one else has.
I can tell when something is upsetting me and decide not to let my mind go down the rabbit hole. I bring my focus back to the moment, to my breathing, and I can see I’m being calmer.
It was incredibly helpful to learn that I am not my thoughts. Arguing with myself makes no sense. While I’m not sure I buy completely into Eckhart Tolle’s “pain body“, I do appreciate that sometimes there is an “other” who is thinking things that aren’t helpful. Meditation has helped me to stop doing that.
I noticed small, subtle changes to my attitude as well. I got through Noah’s Bar Mitzvah with less stress than with Jacob’s because I was more able to quiet things. The time I spent meditating each day would “reset” me and leave me calmer overall. I found myself focusing on my breath even without really thinking about it at times to avoid getting lost in thought.
I think 10% happier is a decent way to look at this. I may go back to 15 minutes because 20 is often harder to schedule, but I’m not sure yet. I plan to continue Headspace, because I find it to be a useful guide, and I paid for the full year. I also find that using good noise canceling headphones helps.
I’m also convinced that it took this kind of commitment to get the behavior change I needed to do this consistently. It will be interesting to see whether I can maintain that as I start to focus on other skills, but I believe I will. It was that helpful.
On to knitting!
tl;dr: You may enjoy Dan Harris’s book 10% Happier. You may find Headspace helpful. Either way, you should really consider meditating. I found it to be quite valuable.
Where is the Democratic ACA replacement bill?
David Leonhardt says that the Republicans are “unable to agree on a [health care] policy” and “don’t have the votes to pass [an ACA replacement] plan.” OK, but what I want to know is, what is the Democratic alternative?
On the face of things, this is a strange question, because the Democrats cannot pass a bill in this Congress. Nevertheless, the Democrats should think about what they want to see in a replacement. There is a chance that the Republicans will fail to pass a bill that replaces the ACA without harming lots of Americans, including Republican voters. Here’s why:
As Nicholas points out, the Republican’s draft bill that recently leaked showed that they are not close to coming up with a coherent plan. Their current draft could lead to higher costs for insurance, or loss of insurance, for many people currently covered under the ACA. This isn’t playing well.
The far-right House Freedom Caucus has announced that it will oppose any bill that does not fully repeal the ACA. If all 32 HFC members took this view, the remaining House Republicans would not hold a majority. The leader of the larger but less conservative House Republican Study Group has also said that he “couldn’t support the party’s existing Obamacare replacement strategy.”
There are only 52 Republicans in the Senate and a few of them are moderates on the ACA. So it’s not clear that a bill acceptable to the radical right in the House can pass the Senate.
Let’s put this gently: President Trump lacks well-formed views about health care policy. He may not be willing or even able to coordinate the Republican factions.
We don’t know what will happen if no bill is passed or if the ACA is repealed without a replacement. But the Women’s March, the flash protests in response to the Travel Ban, and the uptick in support for the ACA suggest that the Republicans will face well-mobilized opposition if they screw up. If so, the GOP could be looking at the 2018 election with a deeply unpopular president and chaos in the health care system for less affluent Americans. If there is a prospect of losing their majorities, the Congressional Republican leadership might be willing to work with Democrats to pass a bipartisan ACA replacement.
As I described here, there is a left argument that Democrats should refuse any compromise and let the Republicans reap the consequences of their policies. A centrist counter-argument is that a lasting change in health care institutions requires bipartisan legislation, and the best time to get a deal is when Republicans are desperate.
Do I think that it’s likely that the Republicans will be willing to negotiate with Democrats about an ACA replacement? No. The lesson of 2016, however, is that anything is possible. So if the opportunity to negotiate arrives, the Democrats will need to have thought through what compromises they would be willing to accept.
If Obamacare exits, some may need to rethink early retirement
The following originally appeared on The Upshot (copyright 2017, The New York Times Company). It also appeared on page A10 of the February 28, 2017 print edition.
Here’s another possible consequence of repealing the Affordable Care Act: It would be harder for many people to retire early.
Americans reaching 65 become eligible for Medicare. Before reaching that age, some can get retiree coverage from their former employers. But not very many companies, especially small ones, offer medical insurance to retirees. If early retirees are poor enough, they could turn to Medicaid. To retire early, everybody else would need to turn to the individual health insurance market. Without the subsidies and protections the A.C.A. put in place, health care coverage would be more difficult to obtain, cost consumers more where available, and provide fewer benefits than it does today.
That means that if the A.C.A. is repealed, retiring early would become less feasible for many Americans.
This consequence is called job lock — the need to maintain a job to get health insurance. One of the arguments in favor of the A.C.A. was that it would reduce or eliminate job lock. With repeal of the law on the agenda of Congress and President Trump, there is renewed concern about how health insurance could affect employment and retirement decisions.
These relationships have been examined extensively by scholars. Though not all studies have found evidence of job lock in the pre-Obamacare era, a majority of high-quality studies have. That’s the conclusion of systematic reviews conducted by the Government Accountability Office and several health economists.
Because people approaching retirement age are more prone to illness and high health care costs, employment-based insurance is particularly valuable to older workers — so much so that many studies document that it influences retirement decisions. One study found that workers whose employers offered retiree health benefits were 68 percent more likely to retire early than those who lack employer-based retiree coverage.
Another study found a smaller effect, 47 percent. But that study also found that workers in poor health who had retiree health benefits were 88 percent more likely to retire early compared with similar workers lacking retiree health benefits. Both those studies used data that are now several decades old. But a 2014 study that incorporated more recent data — though still pre-A.C.A. — also found that retiree health benefits encourage early retirement. The inference from these studies is that coverage options in the A.C.A. marketplaces would similarly encourage early retirement.
Deferring retirement because of health benefits is just one form of job lock. Another example: Many studies show that spouses are much more likely to work if their partners do not have employer-based family coverage. Other studies show that workers with cancer are more likely to continue working if that’s how they get health insurance.
Two studies led by Cathy Bradley of Virginia Commonwealth University examined working women with breast cancer diagnoses. Both studies found that those who depended on their employment for coverage were more likely to remain working.
If not for job lock, we’d probably see greater job mobility and entrepreneurship. According to one analysis, two million more people would change jobs if it weren’t for job lock — presumably finding work that makes them happier or to which they are better suited. One study found that 25-to-55-year-old married men with no other coverage options are 22.5 percent less likely to switch jobs compared with those who have alternatives. Another study, examining 24-to-35-year-old married men, estimated smaller effects, between 10 and 15 percent.
The evidence of sticking with jobs instead of starting a business is mixed, but the preponderance of it suggests this kind of “entrepreneurship lock” exists, affecting up to four million people. Workers without coverage from a spouse — therefore, more reliant on their own employers’ coverage — are a few percentage points less likely to become self-employed, according to one study. Similarly, self-employment spikes when workers turn 65 and obtain Medicare coverage.
From the late 1980s to the early 2000s, tax deductibility of policies for self-employed workers was phased in, making those policies more affordable. Two studies provide evidence that this change increased self-employment. One found that it rose 10 percent among women without health coverage from a spouse versus those with such coverage. Another found that the tax change explained as much as half the total increase in self-employment between 1999 and 2004.
All of these studies suggest that job lock would be alleviated by more available and affordable coverage outside work. Whether Obamacare did that is less clear. Many policy experts expected the A.C.A. to reduce job lock. An analysis by the Urban Institute, conducted before the health insurance reforms were implemented, estimated that the self-employed would increase by about 1.5 million individuals as a result of the law. In 2014, the Congressional Budget Office anticipated that the A.C.A. would reduce the size of the labor force by at least two million people by 2024.
One post-A.C.A. study found that the prohibition of pre-existing condition exclusions for children increased job mobility for their parents. And in the months after the insurance market reforms rolled out, voluntary part-time work increased and the growth in the number of workers over age 55 slowed, both consistent with alleviation of job lock. But more rigorous studies of part-time work did not find an impact from the A.C.A.
According to a review of scientific papers by the economists Jean Abraham and Anne Royalty, for the University of Pennsylvania’s Leonard Davis Institute of Health Economics, few other studies have found solid evidence that the A.C.A. reduced job lock or had other effects on the labor market. For instance, studies have not found that allowing children to stay on their parents’ insurance until age 26 has influenced the labor market choices of young adults. Nor have they found that the A.C.A. increased early retirement or employment more generally.
One reason studies might not have found an impact on job lock could be because the law is relatively new, and there isn’t enough data available to researchers to tease out all its effects. It could also be because the law has been under siege on multiple fronts since passage, rendering its status uncertain. This may have raised doubts in workers’ minds about the wisdom of relying on it as a substitute for employer-offered coverage.
But it is clear that with A.C.A. repeal on the table, people contemplating early retirement may need to reconsider.
February 28, 2017
The health care system treats patients like garbage
I started and stopped writing this post many times because it’s mostly whining. But, dammit, it’s a consumer’s right to whine, so here it is: in my experience (YMMV) — and that of many others I know — the health care system largely treats patients like garbage.
I was reminded of this fact during my recent experience dealing with my daughter’s broken arm. It started well enough. Our pediatrician has late hours and an X-ray machine, so we were able to skip the Friday night (and more expensive) emergency department visit for our initial diagnosis, and therefore missed all the attendant waiting and frustration.
Upon viewing the X-rays, the pediatrician conveyed that it was not a bad break and didn’t need to be addressed immediately. A brace, which she provided, was good enough for now. Fair enough. But what was our next step? “The X-rays need to be examined by a radiologist before I can tell you that,” my wife was told. OK …
I wonder how long we would have waited for that to happen. By the middle of Saturday, we became too uncomfortable to find out, so I called the pediatrician’s office. Now, and with no further consideration of the X-rays, they were wiling to give us some recommendations for orthopedic clinics. Why couldn’t those have been given to us on Friday?
Naturally, one clinic was closed on the weekend. But, the other, hospital-based one, had Sunday hours. Great! A call to that clinic got me a voice-mail. I left a message. I have never gotten a call back, but I didn’t wait for one. I called again later and got a person who told me they had 7AM walk-in hours. Just go to the main hospital entrance and ask for the walk-in orthopedic clinic, I was told.
This was bad advice. After dragging my broken-limbed daughter through every door that plausibly seemed like the main entrance, we finally found someone who said we should go through the ED entrance. That was the right answer, but not what we were told on the phone.
After waiting and registering, we finally saw the orthopedist. He was great. It was, in fact, not a bad break. Now it is safely casted. All is well. But not before we had to do a lot of legwork — and received a lot of wrong answers, promises of follow-ups that didn’t happen, etc. Meanwhile, our pediatrician has not (yet) checked in on her patient.
I get it. She’s busy with more urgent matters. It makes sense, but it sucks, and all the more knowing that we spend a fortune for such treatment. No other business would treat customers this way. In health care, inconvenience, uncertainty, lost records, lack of follow-up and coordination, the necessity of self-advocacy, and lots and lots of waiting is the norm.
Of course, there are some examples of good customer service in health care. I’ve even experienced them. But every tasty crumb I’m tossed just reminds me how awful the rest of the meal is.
In his most recent article, Atul Gawande related an example of good customer service in health care. The patient, Haynes, had experienced a lifetime of frequent, debilitating migraines. None of the more standard treatments worked, so his doctor, Loder, got creative.
The most exotic thing they tried was Botox—botulinum-toxin injections—which the F.D.A. had approved for chronic migraines in 2010. She thought he might benefit from injections along the muscles of his forehead. Haynes’s insurer refused to cover the cost, however, and, at upwards of twelve hundred dollars a vial, the treatment was beyond what he could afford. So Loder took on the insurer, and after numerous calls and almost a year of delays Haynes won coverage.
That’s what I’m talking about! This should be standard, but it isn’t. More typically, the patient is left holding the bag. You want the treatment you need, go fight your insurer for it. The health system is not going to help you, because it is not in most stakeholder’s interest to do so. It also should be noted that such inconvenience keeps health spending down — and I completely appreciate the need to be prudent with spending — but it still sucks for patients.
Perhaps concierge medicine is the answer, or paying more for your own care. We’ll see, because we’re running that experiment right now. I’m not seeing a lot of movement, but maybe it’s too early or I’m unlucky. I could just be a whiner.
Aaron E. Carroll's Blog

- Aaron E. Carroll's profile
- 42 followers

