
Stuart Jeanne Bramhall's Blog: The Most Revolutionary Act , page 623
December 25, 2021
US Population Migration Patterns Under Covid

these graphics are from longtime gatopal
kbirb who has done so much excellent analysis lo these 21 months. (note this is only thru july 2021 and seems to be ongoing and is likely larger by now)
el gato malo – bad cattitude – december 24, 2021
Via Aletho News

big winners: the free states of florida, texas, arizona
big losers: the karentopias of california, new york, illinois
this really speaks volumes.
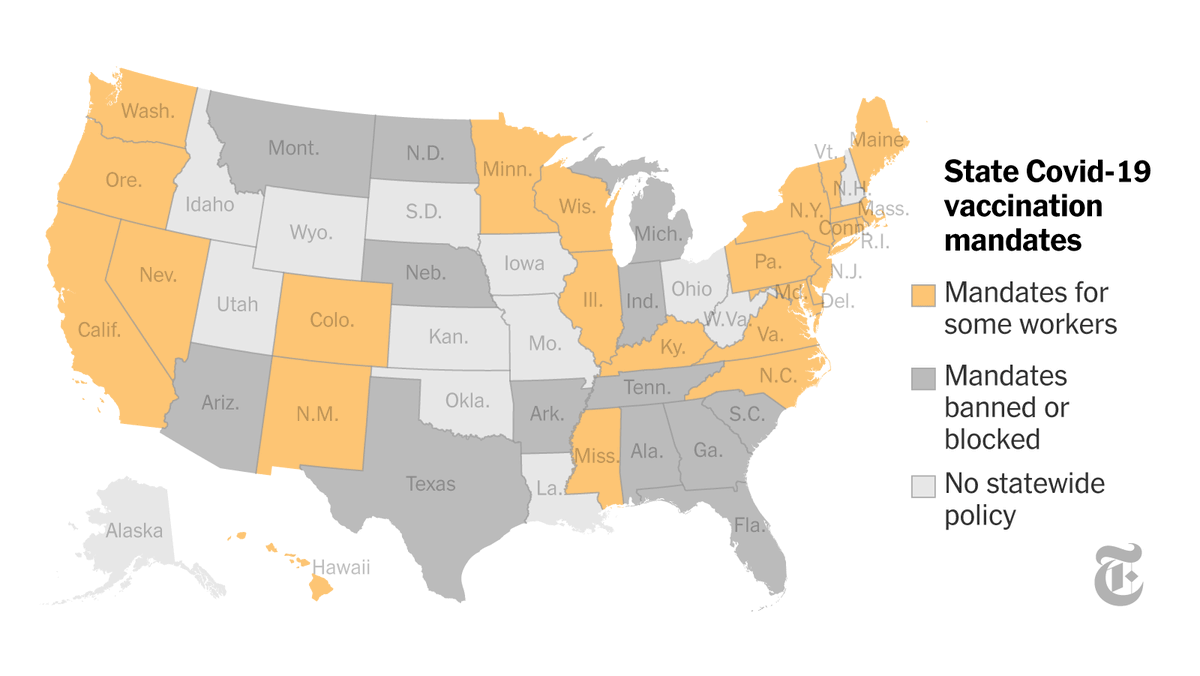
red v blue gets extreme:
Political party look (Governor), stunningly nearly a million fewer people call blue states home, now calling red states home. From July-to-July data, not yet reflecting recent mandate, freedom restriction & passport ideologies most common in BLUE states. May now be higher.
3/ pic.twitter.com/p3QF4qhfJA
— KBirb (@birb_k) December 23, 2021
and it sure looks like “access to education” is a major driver.

though this graphic (from NYT ) has interesting overlay too.
 speaking as one who spent the summer in a free state only to return to the assault and dingbattery of a masked up, restricted, and vaxxpassed puerto rico, it is JARRING.
speaking as one who spent the summer in a free state only to return to the assault and dingbattery of a masked up, restricted, and vaxxpassed puerto rico, it is JARRING.
once you see that this is not really a thing, that life is normal in half the country, and that continuing to play this game or even care about it is utterly optional, there is no closing your eyes again.
you cannot go back to a mask mandate grocery store and not see all these people as having mental health issues (or at the very least some sort of societal spinal atrophy that renders them unable to support a republic.)
half the people i know are talking about leaving PR. it’s become intolerable, especially once you have seen the options firsthand. hearing the same about new york, SF, LA, etc.
it’s just endless and capricious and increasingly aimed at deliberately making life miserable for any who refuse to comply. this round feels personal. “all you have to do to make the persecution end is comply!” it’s an oppressively ubiquitous mantra and the “jim covid” laws are entering every phase of life.
but one trip to florida and the spell breaks.
you realize you’re being conned because you see it first hand and remember.
maybe you moved there because you wanted your kids to see the inside of a classroom at some point before 2024.
this derangement is going to seriously redraw some american maps.
the damage is not the pandemic, it’s the policy. that’s why this is divided so starkly by donkey vs elephant. covid has been a political, not an epidemiological crisis and remains one.
and the more we can support state’s rights and thereby create more and more varied choice for people to pursue their happiness, the more this flow will become a torrent.
hopefully the last people out of the karen-capitals will remember to turn off the lights when they leave…
[…]
Via https://alethonews.com/2021/12/24/covidian-migration-patterns/


Fermented Foods May Lower Risk of Death, Probiotics May Ease Depression
 Creamy Sauerkraut with parsley, chives and potatoes
Creamy Sauerkraut with parsley, chives and potatoes
This article was previously published August 6, 2020, and has been updated with new information.
By Dr. Joseph Mercola | December 23, 2021
I’ve written many articles detailing lifestyle and dietary strategies that may decrease your COVID-19 risk by boosting your immune function and general health. Now we can add fermented foods to the list, which shouldn’t come as such a great surprise, considering the influence your gut health has on your immune system.
The study,1 posted July 7, 2020, on the pre-print server medRxiv, conducted by researchers in Berlin, Germany, looked at whether diet might play a role in COVID-19 death rates. Interestingly, mortality rates tend to be lower in countries where consumption of traditionally fermented foods is commonplace. As reported by News Medical Life Sciences:2
“The researchers say that if their hypothesis is confirmed in future studies, COVID-19 will be the first infectious disease epidemic to involve biological mechanisms that are associated with a loss of ‘nature.’ Significant changes in the microbiome caused by modern life and less fermented food consumption may have increased the spread or severity of the disease, they say.”
Could Fermented Veggie Consumption Lower COVID-19 Mortality?
The researchers obtained data from the European Food Safety Authority (EFSA) Comprehensive European Food Consumption Database and compared consumption levels with COVID-19 mortality statistics (deaths per capita) for each country, obtained from the Johns Hopkins Coronavirus Resource Center.
For each g/day increase in the average national consumption of fermented vegetables, the mortality risk for COVID-19 decreased by 35.4%.The EFSA database includes statistics on countries’ consumption of fermented vegetables, pickled or marinated vegetables, fermented milk, yogurt and fermented sour milk specifically.
They also looked at potential confounders, such as gross domestic product, population density, percentage of the population over the age of 64, unemployment and obesity rates. According to the authors:3
“Of all the variables considered, including confounders, only fermented vegetables reached statistical significance with the COVID-19 death rate per country.
For each g/day increase in the average national consumption of fermented vegetables, the mortality risk for COVID-19 decreased by 35.4%. Adjustment did not change the point estimate and results were still significant.”
Probiotics May Ease Depression
In related news, a review4 of seven small clinical trials has found probiotics and/or prebiotics may be helpful for those struggling with depression and anxiety. While these mental health challenges are epidemics in their own right, the global lockdowns certainly have not made the situation any better.
According to the authors,5 all of the studies “demonstrated significant improvements in one or more of the outcomes” compared with no treatment, placebo, or baseline measurements, leading them to conclude that “utilizing pre/probiotic may be a potentially useful adjunctive treatment” for patients with depression and/or anxiety.
The review builds on earlier studies that have shown people with depression tend to have higher amounts of specific gut bacteria than those who are not depressed.
While it seems the gut microbiome’s role in health is a very recent discovery, as early as 1898 — yes, 122 years ago — a paper6 in The Journal of the American Medical Association proposed that intestinal microbes might play a role in melancholia. As noted in the 2019 paper, “The Microbiome and Mental Health: Hope or Hype?”:7
“The primary tenet of FMT [fecal microbiota transplantation] is that dysbiosis within the human host gut microbiome predisposes an individual to disease. The exact mechanisms through which this occurs have not yet been established, but several potential direct and indirect pathways exist through which the gut microbiota can modulate the gut–brain axis.
These pathways include endocrine (cortisol), immune (cytokines) and neural (vagus and enteric nervous system) pathways, and the assumption is that introducing microflora from a healthy individual will help recolonize the system with a microbial pattern more in keeping with wellness either by establishing the new healthy microbiota or by allowing the host to ‘reset’ their own microflora to a pre-illness state.”
Bacteria Associated With Mental Health and Depression
Two types of gut bacteria in particular, Coprococcus and Dialister bacteria, have been shown to be “consistently depleted” in individuals diagnosed with clinical depression. According to the authors of a study published in the April 2019 issue of Nature Microbiology:8
“Surveying a large microbiome population cohort (Flemish Gut Flora Project, n = 1,054) with validation in independent data sets, we studied how microbiome features correlate with host quality of life and depression.
Butyrate-producing Faecalibacterium and Coprococcus bacteria were consistently associated with higher quality of life indicators. Together with Dialister, Coprococcus spp. were also depleted in depression, even after correcting for the confounding effects of antidepressants.”
The researchers went on to analyze and catalogue the neuroactive potential of these gut bacteria, finding that those associated with good mental health had the ability to synthesize the dopamine metabolite 3,4-dihydroxyphenylacetic acid, while those associated with depression produce γ-aminobutyric acid. Other studies have identified yet other microbial profiles associated with better or worse mental health. For example:
•2016 research9 found the relative abundance of Actinobacteria was increased, and Bacteroidetes was decreased in depressed individuals compared to healthy controls.
•A 2015 study10 found patients diagnosed with major depressive disorder had higher amounts of Bacteroidetes, Proteobacteria and Actinobacteria, and lower amounts of Firmicutes than healthy controls.
“These findings enable a better understanding of changes in the fecal microbiota composition in such patients, showing either a predominance of some potentially harmful bacterial groups or a reduction in beneficial bacterial genera,” the authors wrote.
•A 2014 study11 found depressed individuals had an overrepresentation of Bacteroidales and an underrepresentation of Lachnospiraceae bacteria.
Lachnospiraceae are a family of beneficial bacteria that ferment plant polysaccharides into short-chain fatty acids such as butyrate and acetate.12 The genus Oscillibacter, and one specific clade within Alistipes were also significantly associated with depression.
[…]
South African studies reveal high levels of natural immunity best defense against omicron

Dr Eddy Betterman
Two new studies from South Africa found that the country has a lower hospitalization rate for Wuhan coronavirus (COVID-19) infections caused by the post-vaccine omicron variant. High levels of natural immunity among South Africans stemming from prior COVID-19 infections is likely a contributing factor to this.
Since the appearance of the post-vaccine omicron variant, mainstream media outlets have tried to speculate regarding the variant’s virulence and deadliness. They repeatedly ignored South African health authorities, including Health Minister Joe Phaahla, who said that hospitalizations caused by omicron are “relatively low” and that the world has nothing to worry about.
According to data from South African health authorities, COVID-19 cases in South Africa have skyrocketed in recent weeks, in line with the emergence of the post-vaccine omicron variant. But what has puzzled scientists studying the data is that the country’s hospitalization rate has risen at a significantly slower pace compared to previous waves. (Related: Omicron could actually be the SOLUTION to the entire covid plandemic.)
The data strongly suggests that people diagnosed with omicron in South Africa were around 80 percent less likely to be admitted to the hospital than those diagnosed with any other COVID-19 variant.
Once admitted to the hospital, patients infected with omicron have a lower chance of developing severe disease. They are also hospitalized for fewer days on average than other COVID-19 patients.
In the first 31 days of the current post-vaccine outbreak, the country recorded 164,911 new COVID-19 cases. But just 3,432 patients were admitted to hospitals for additional care. One-hundred and ninety-four died.
In comparison, during the first 31 days of the previous wave, 38,577 COVID-19 cases were recorded and 10,088 were admitted to hospitals. The death rate of that wave was also more than three times higher than the death rate of the current wave, with 668 deaths in the first 31 days.
High vaccination rates unlikely to protect countries against omicron“We believe that the evolution of cell-mediated immunity from prior natural infection … is resulting in the uncoupling of the high case rates seen with the omicron variant and the rates of severe disease,” wrote South African researchers in one of the new studies conducted on the outbreak in the country.
They added that the immunity “is primarily due to natural infection.”
[…]
December 24, 2021
Governments call for crackdown on Telegram because some people are using it to organize protests against covid fascism

NaturalNews.com / Ethan Huff
(Natural News) German bureaucrats have declared the Telegram messaging app to be a threat to “democracy” and a “hotbed of radicalization” because some people use it to organize protests against Wuhan coronavirus (Covid-19) fascism.
Fake news stories from German media outlets such as Tagesschau and Deutsche Welle have been consistently framing Telegram as a gathering place for “dangerous conspiracies, vaccine misinformation, and the driving force behind the ‘violent’ protests” against the country’s lockdowns, mask mandates, and compulsory “vaccination” edicts.
Since the beginning of December, in fact, the fake news media machine in Germany has been going nuts in opposition to Telegram – almost like they are all controlled by the same hidden hand of propaganda.
Thüringen interior minister George Mair, a member of the Social Democrats party in Germany, actually proposed trying to penalize Telegram if the platform refuses to remove “harmful” content that goes against the government’s Fauci Virus tyranny.
Mair says that bureaucrats like himself could set up “geoblocking” protocols to disallow Germans from using the platform. The service could also be disabled from certain regions of the country using IP protocol blocking.
Roland Wöller of the Christian Democrat party echoed Mair’s sentiments, suggesting that more “radicalization” on Telegram will occur if politicians like himself impose mandatory jab policies across Germany.
Wöller has suggested punishing the company behind the Telegram app if any “criminal” acts that occur in Germany can somehow be traced back to the platform’s use.
“Officials are also calling for the deanonymization of users on the platform,” reported The National Pulse.
Wöller further suggested opening criminal investigations into Telegram users after their anonymity is scrapped.
Germany’s tyrant political class says opposing covid fascism is “hate”At no point have any of these corrupt bureaucrats even considered the fact that they are the ones who have been radicalized. Their total lack of self-awareness has led them to the conclusion that their imposition of mass medical fascism is completely normal, and that anyone who opposes it is a “terrorist.”
The truth, of course, is that Mair and Wöller and their kind are the true radicalized terrorists in this whole equation. They are the ones who deserve prosecution and punishment for committing crimes against humanity.
They do not see things this way, though. Nancy Faeser, the new German government’s interior minister, recently announced that her number-one priority is to fight “right-wing extremism” on Telegram.
Faeser believes that all opposition to Wuhan coronavirus (Covid-19) fascism represents “hate speech and aggression,” and that it must be punished with “strict measures” to stamp it out from all of Germany.
“What is happening on Telegram is not only disgusting and inappropriate, but also, in most cases, criminal,” further decreed Marco Buschmann, a member of the German Bundestag and yet another medical fascist leading Germany off a cliff.
“The law is clear on this,” Buschmann further declared. “We have to think about all the possibilities … my wish is not to have a German way … but a European framework, which will allow us to fight against this hate.”
[…]
WHO Blasts Additional Jabs: ‘No Country Can Boost Its Way Out of the Pandemic’

Source: Salvatore Di Nolfi/Keystone via AP
The World Health Organization criticized the rollout of booster programs as many poor nations haven’t even gotten first doses yet and warned that more variants have the potential to develop under these conditions.”Blanket booster programs are likely to prolong the pandemic, rather than ending it, by diverting supply to countries that already have high levels of vaccination coverage, giving the virus more opportunity to spread and mutate,” said WHO Director-General Tedros Adhanom Ghebreyesus. “No country can boost its way out of the pandemic.”The WHO director’s comments echo what some public health experts have also been saying.
“Africa right now is essentially a superincubator,” said Andrea Taylor, assistant director of programs at the Duke Global Health Innovation Center, a leading authority on global vaccine supply.
And the emergence of a new variant “is exactly what experts have been warning about for months,” she said. “We saw what happened with India, which gave rise to the delta variant. And we said, ‘Look, this is going to happen in Africa where there is uncontrolled transmission.’” […]
“While we still need to know more about omicron, we do know that as long as large portions of the world’s population are unvaccinated, variants will continue to appear, and the pandemic will continue to be prolonged,” Dr. Seth Berkley, CEO of Gavi, the Vaccine Alliance, a leading partner in the global vaccine sharing program COVAX, said in an email. (NBC News)
The warning comes as the White House is aggressively pushing booster shots and as Israel announced those over 60 are eligible for a fourth Covid-19 jab.
[…]
Via https://townhall.com/tipsheet/leahbarkoukis/2021/12/24/who-on-boosters-n2601008
The Civilizations of Ancient Africa

Episode 28: African Kingdoms and Trade
The Big History of Civilizations (2016)
Dr Craig G Benjamin
Film Review
This is one of my favorite lectures as African history is so rarely taught in school. Benjamin begins by describing the Mali king Mansa Musa of Mali, who became world famous in 1324 when he undertook the Hajj to Mecca. He was accompanied by thousands of soldiers, attendants and slaves, as well as a hundred camels loaded with sacks of gold. He bestowed lavish gifts on all the kings and nobles who hosted him. He left so much gold behind stopover in Cairo that the global value of gold dropped by 25%.
On his return to Mali, he built mosques and madrassas* and sent students to study with Muslim in North Africa. Under Mansa Musa’s rule, Mali became one of the most famous centers of Muslim learning in the world.
Benjamin divides Africa’s early agrarian civilizations into tropical rainforest and savanna* cultures. Savanna-based societies were almost entirely patrilineal. Approximately 15% of the rainforest cultures were matrilineal. However even in patrilineal cultures, female relatives of chiefs played an important role as public officials, political and religious advisors and even soldiers.
Prior to the advent of Christianity and Islam, African cultures were polytheistic. Although some believed in a higher creator god, most appealed to nature gods or ancestors to protect them against crop failure or illness. In many cases, they relied on female shamans to intercede for them.
Farming first appeared in sub-Saharan Africa around 3000 BC just as the Sahara was desertified (prior to 3000 BC the region’s numerous lakes and rivers sustained tropical rainforests).
According to Benjamin, the first agrarian civilizations appeared around 1500 BC in four independent farming centers: the Ethiopian highlands (growing millet, sesame and mustard seed); the savannas of central Sudan (growing sorghum, millet, rice, peas and nuts); the West African savanna (growing oil palms, peas and yams) and in West African rainforests (growing bananas and coffee).
Around 1000 BC, domesticated cattle, sheep, goats and pigs spread to Africa from Asia. During the 7th century BC, iron metallurgy reached sub-Saharan Africa. Meroë in the Numbian kingdom of Kush became the first sub-Saharan iron works center, followed by Nok (in modern day Nigeria), which produced high quality steel comparable to that of Egypt and Rome. The adoption of steel tools, combined with improved food production, led to a substantial population increase, the development of specialized crafts and complex social structures and robust trade.
Benjamin also credits these changes for what he refers to as “Bantu expansion.” Between 3000 BC and 1000 AD, speakers of Bantu languages spread out from the Cameroon/Nigeria highlands throughout sub-Saharan Africa as hunter gatherer cultures transitioned into sedentary, socially complex societies that traded with Egyptian and Arab merchants.
West African agrarian civilizations included
Aksum – the hub of the Aksumite empire, was established in northern Ethiopia around 400 BC. By the 8th century AD it had been taken over by Muslim traders.Nok (500 BC – 200 AD) – the first culture to appear in modern day Nigeria, initially interacted peaceably with Berber*** nomads in the Sahara desert. It collapsed in 200 AD after continual Berber attacks caused it to lose control of the gold, salt and slave trade.Malentu (modern day Ghana) – regained control of the gold trade and created the Mali empire In the 13th century AD. When gold replaced silver as the main currency of Europe, Mali became the world’s largest supplier of gold, exporting several tons annually.Songhai empire – replaced the Mali empire in the 15th century and built magnificent mosques and madrassas in Timbuktu. It was the largest west African empire until they were defeated by the Moroccans (who had gunpowder) in the late 16th century.Jenne-Jeno – an 80 acre city in the fertile Niger Delta around 250 BC. It’s success related largely to its easy access to salt and minerals from the Sahara and animals, plants and gold from southern cities. For many centuries it controlled all trans-Sahara trade.Ghana (named after its first warrior king) – founded in the 4th century AD, it monopolized the sub-Saharan trade in gold, salt and slaves**** for four centuries.In East Africa, Swahili speaking people had formed hundreds of city-states prior to the arrival of Portuguese explorers and soldiers in the 15th century. Most of their rulers converted to Muslim, created classic Muslim palaces, mosques and fountains and traded gold, ivory and slaves.
In central Africa, agrarian civilizations included
Mapungubwe – great city stated founded around 1075 AD. Its rulers amassed great power by assembling giant cattle herds and using them to trade with Swahili coastal cities. Mapungubwe ultimately became greater Zimbabwe (“houses of stone,” named after the magnificent stone palaces their elites lived in).Kongo (just north of greater Zimbabwe) – founded in 1390 AD. In 1665, it became a Portuguese colony after Portuguese troops killed their king in battle.*Savanna is a mixed woodland-grassland ecosystem where trees are widely spaced, allowing sufficient sunlight for abundant grassland.
**In patrilineal kinship systems, the line of descent (inheritance and property rights) derives from the father’s lineage. In matrilineal systems the line of inheritance is traced through the mother.
***Muslims referred to Libyans as “barbars” (from the Greek word for barbarian) because they were extremely hard to conquer. This was later bastardized to Berber.
****Between the 8th and early 20th century, roughly one million slaves were transported 1200 miles across the Sahara desert to be shipped to distant regions. This number excludes the Transatlantic slave trade.
https://pukeariki.kanopy.com/video/african-kingdoms-and-trade
December 23, 2021
Hospitals Choosing Patient Death Over Ivermectin
Seriously ill patients facing death from late stage COVID infection increasingly face hospital protocols that have a terrible record of saving lives. In fact, nearly all such patients die. This explains why over 1,200 Americans are dying everyday from COVID. In a week, more people die from late stage COVID than died in the 9/11 attacks. Yet this is not major news on mainstream media outlets. Getting used to COVID deaths has produced complacency rather than rage.
As we approach 800,000 COVID related deaths in the US it is important to note that many and probably most of these occur in a hospital. The evidence clearly shows that approved hospital protocols for seriously ill COVID patients in ICUs are ineffective.
Patients suffer on a ventilator, getting oxygen, perhaps a steroid, often with pneumonia and in an induced coma, and worst of all being given remdesivir that has a terrible track record, does not save lives and has deadly side effects.
Some may ask why doctors are not standing up and fighting for these patients, fighting to save their lives. A physician in Hawaii who I greatly respect, has first-hand experience with successful use of IVM and recounted how he wanted to help a family. They had a love one in a hospital on induced sedation with a ventilator for 3 weeks. He tried to get IVM used. The doctor at the hospital said they had their own protocol, the usual government one and would not consider using IVM. The family could not get local lawyers to put in the paperwork for a court action. Nor could they find a local independent doctor. And the doctor who told me about this situation worked for a big organization that would not allow him to intervene.
He discovered the reality that no doctors were brave enough to stand up against the entire medical establishment to administer IVM to a dying patient. The patient died a few days later without ever getting a dose. My doctor said it was “Heart breaking. I am afraid the successful stories are the exception. Sad.”
His story is true for almost all US physicians in hospitals. They have capitulated to the evil, ineffective public health system. They rather let their COVID patients die than truly follow the science and save their lives. So, below is the science case for this use of IVM.
The behavior of hospitals themselves is even worse. Attorneys working for families trying get a hospital to allow use of IVM face awful legal tactics to defeat or just delay favorable court decisions until the deathbed patient succumbs. They file endless motions and sometimes go to an appeals court. Anything to fight use of IVM and nothing really effective to save lives. Many weeks in an ICU means big hospital bills.
Late stage COVID disease uses one especial feature of IVM
Patients and their families desperate for a better outcome often find evidence for using IVM. This usually happens after they see their relative getting worse and worse in the ICU as the hospital keeps using the government approved protocol.
In fact, there is some solid medical research that supports using IVM for late stage COVID disease. Peter McCollough, the preeminent medical expert on COVID agrees there is a valid scientific explanation of why IVM works in late stage COVID infection. Beyond its anti-viral character, it is also an anti-inflammatory medicine.
Here is the title of an April 2021 medical research study: “Anti-inflammatory activity of ivermectin in late-stage COVID-19 may reflect activation of systemic glycine receptors.” It noted that “the clinical utility of ivermectin in the cytokine storm phase of COVID-19 reflects, at least in part, an anti-inflammatory effect.”
An earlier study was “Ivermectin may be a clinically useful anti-inflammatory agent for late-stage COVID-19” It noted: “it is reasonable to suspect that, in doses at or modestly above the standard clinical dose, ivermectin may have important clinical potential for managing disorders associated with life-threatening respiratory distress and cytokine storm—such as advanced COVID-19.
[…]
Via https://thebluestateconservative.com/2021/12/22/hospitals-choosing-patient-death-over-ivermectin/
US Approves First Injury Claim for COVID “Countermeasure,” as Backlog Grows to 4,000+ Claims
 By Michael Nevradakis, Ph.D.
By Michael Nevradakis, Ph.D. The U.S. government program that processes claims for COVID vaccine- and countermeasures-related injuries, the Countermeasures Injury Compensation Program, will issue compensation for its first claim. It’s unknown if the claim is related to a vaccine or some other medication or device related to the diagnosis or treatment of the virus.
The U.S. government program that processes claims for COVID vaccine- and countermeasures-related injuries will issue compensation for its first claim.According to the Countermeasures Injury Compensation Program (CICP) website, “[o]ne COVID-19 claim has been determined eligible for compensation and is pending a review of eligible expenses.”
The website cites data aggregated by the CICP as of Nov. 1, the most recent date for which information regarding such claims is available as of this writing.
CICP did not reveal the terms of the compensation.
Confirmation of the claim comes almost a year after distribution of the vaccines began and after 965,843 reports of adverse events following COVID vaccines were submitted to the Vaccine Adverse Event Reporting System (as of Dec. 10).
However, it is unclear whether the claim that will be compensated pertains to a reaction to a COVID vaccine, or to some other COVID-related treatment, The Epoch Times reported.
The CICP was established under the aegis of the Public Readiness and Emergency Preparedness (PREP) Act of 2005. The PREP Act was developed to coordinate the response to a “public health emergency.”
The law is scheduled to remain in place until 2024.
The CICP program focuses on countermeasures, such as “a vaccination, medication, device or other item recommended to diagnose, prevent or treat a declared pandemic, epidemic or security threat.”
The CICP allows individuals to claim compensation for lost wages and for medical expenses not fully reimbursed by insurance or government programs, such as Medicaid.
Individuals also can claim death benefits for someone who died as a result of a countermeasure.
The program is run by the Health Resources & Services Administration (HRSA), an agency of the U.S. Department of Health and Human Services.
It is separate from the National Vaccine Injury Compensation Program (VICP), which covers injuries related to vaccines that are routinely administered to children and pregnant women.
The CICP is known for its cumbersome claims process and low likelihood of success for claimants. To date, under 4% of petitioners have been compensated under the program.
A total of $500 million reportedly was appropriated to the CICP for COVID-related claims.
Approval of a single claim magnifies CICP backlog
According to the HRSA’s own figures, from fiscal year 2010 until Nov. 1, a total of 5,242 claims were filed with the CICP.
Of these, 4,751 pertain to COVID, including 2,297 claims related to COVID vaccines, and 2,454 for other countermeasures.
[…]
Via https://childrenshealthdefense.org/defender/injury-covid-countermeasure-backlog-grows/
Pfizer Clinical Trials Poorly Designed from the Start

The Canadian COVID Care Alliance assembled a presentation that demonstrates how Pfizer’s purported randomized placebo-controlled, double-blinded study veered away from methodologies that would have definitively answered questions about the vaccine’s safety and efficacy.
The disagreements around whether COVID-19 vaccinations are “safe and effective” stem not only from the subjective nature of such descriptors but also from the lack of consensus around the data used to substantiate or refute such a claim.The Centers for Disease Control and Prevention’s (CDC) Morbidity and Mortality Weekly Reports (MMWR) often draw from limited observations, and their assessment of vaccine effectiveness is based on relatively small subsets of our population.
Their conclusions are sometimes reflective of outdated data and conflict with their own recommendations.
For example, here the CDC’s latest estimation of vaccine effectiveness is upwards of 80% in preventing COVID-19 (i.e. the risk of becoming infected is 5 times less if vaccinated). Why then the recommendation for boosters?
Note that this latest metric is based on the CDC’s most recent data from more than one month ago and represents data drawn only from 27 jurisdictions.
Eric Topol, a professor of molecular medicine at Scripps Research, is a former advisory board member of the Covid Tracking Project, a team that worked to collect and synthesize local COVID-19 during the peak of the pandemic.
Politico recently quoted Topol:
“I think we’ve done a horrible job from day one in data tracking for the pandemic. We’re not tracking all the things that we need to to get a handle on what’s going on. It is embarrassing.”
Meanwhile, vaccine injuries continue to accumulate in the Vaccine Adverse Event Reporting System (VAERS) and go unacknowledged, making any constructive discussion around risk impossible.
In order to find common ground, it is perhaps most appropriate to focus on published data from the vaccine trials themselves.
Was Emergency Use Authorization justified? Was the current confusion around vaccine effectiveness and safety predictable from the beginning?
A presentation by the Canadian COVID Care Alliance
Canadian COVID Care Alliance (CCCA) is a group of “Independent Canadian doctors, scientists and healthcare professionals committed to providing top quality and balanced evidence-based information to the Canadian public about COVID-19 so that hospitalizations can be reduced, lives saved and our country restored as safely as possible.”
CCCA assembled a presentation that comprehensively demonstrates how Pfizer’s purported randomized placebo-controlled, double-blinded study veered away from methodologies that would have answered the safety and efficacy questions definitively.
In this concise slide deck with an explanatory video, CCCA powerfully summarized why Pfizer’s trial was not designed to adequately demonstrate its product’s safety and efficacy.
Here are a few key points from the CCCA presentation:
Initial data demonstrated a high relative risk reduction of infection yet this amounted to an absolute risk reduction of only 0.84%. It is the absolute risk reduction that determines the risk-benefit ratio required to make informed decisions around inoculation.Early unblinding: Several months before publishing six-month observational results Pfizer opted to offer its product to those participants who received the placebo. By eliminating nearly all participants in the placebo wing Pfizer effectively closed the curtain on its experiment because long-term comparisons can no longer be made.All-cause mortality and morbidity, the only sensible outcomes to use in determining efficacy and risk, were not considered. Indeed, all-cause mortality was higher in the vaccinated group after six months.Severe adverse events outnumbered cases of severe COVID prevented after six months of observation.Trial participants were not reflective of the most vulnerable members of our population — more than 50% of people dying from COVID are 75 years of age or older. This age group made up only 4.4% of trial participants. Also, 95% of those who have died from COVID had one or more comorbidities. Nearly 80% of trial participants had none.Not every trial participant was tested for COVID. Asymptomatic or paucisymptomatic (presenting few symptoms) cases were missed.[…]
Via https://childrenshealthdefense.org/defender/pfizer-vaccine-clinical-trials-poorly-designed/
December 22, 2021
Why I’m Pro-Vaccine but Anti-Vaccine Mandate

Ryan T. Anderson
Newsweek
Last Thursday, the University of California fired my good friend and new colleague, Aaron Kheriaty, for refusing vaccination. The next day, a federal circuit court allowed President Joe Biden‘s OSHA vaccine mandate to take effect throughout the United States, meaning many other citizens may soon be penalized. But we should not treat conscientious objectors to the vaccine like this.
Dr. Kheriaty, a physician and psychiatrist, has taught and treated patients at the UC-Irvine Hospital and Medical School for 15 years. He has also directed the medical school’s bioethics program.
When COVID hit, Dr. Kheriaty helped the hospital develop ethics guidelines. He treated COVID patients throughout the pandemic, including when everyone was most concerned about the virus’ lethality. As a result, he caught the virus and developed natural immunity.
When vaccines became available earlier this year, Dr. Kheriaty declined to be vaccinated, arguing that his natural immunity provided more protection. In his calculation, the added risks of a novel vaccine were not justified for his personal situation. Rather than respect his medical judgment, UC-Irvine fired him. Now, he directs the Bioethics Program at the research institute I run, the Ethics and Public Policy Center in Washington, D.C.
[…]
Via https://www.newsweek.com/why-im-pro-vaccine-anti-vaccine-mandate-opinion-1661402
The Most Revolutionary Act

- Stuart Jeanne Bramhall's profile
- 11 followers

