
Aaron E. Carroll's Blog, page 3
February 19, 2025
Another year, another round of Shkreli awards
The Lown institute keeps an eye on fraud, waste, and dysfunction in American healthcare, and every year they present the Shkreli awards, named for infamous pharmabro Martin Shkreli. Here we summarize the top 10 terrible operators of 2024
The post Another year, another round of Shkreli awards first appeared on The Incidental Economist.

February 18, 2025
Your Therapist Doesn’t Accept Insurance? Here’s Why.
Finding the right therapist is hard. Finding one that takes insurance can be even harder.
Insurers are required to cover mental health care under the Mental Health Parity and Addiction Equity Act. Yet, almost a third of therapists still don’t accept insurance at all or limit the number of insured clients they treat. The ongoing therapist shortage, exacerbated by the pandemic, has made the hunt for a provider even more difficult. Therapists that do take insurance are often fully booked.
And accepting insurance has its perks, like widening access to a larger client pool.
So why would a therapist not accept insurance in the first place? It turns out, it doesn’t pay as much and can be a real hassle.
Low pay
A 2023 Government Accountability Office report concluded that low insurance reimbursement rates are one of the main reasons why mental health care has become so inaccessible. Therapists just don’t recoup their costs with insurance, so there isn’t much incentive to accept it.
The national average cost of a psychotherapy session is $100-$200/hour, varying based on state, licensure, specialty, and demand for services. While reimbursement rates aren’t publicly available, we do know that they are low, sometimes only a fraction of the cost to provide care.
For instance, fee-for-service Medicaid rates in 2022 for common psychiatry services, including psychotherapy, were only 81% of Medicare’s rates. And Medicare reimbursement rates for behavioral health are already low, hitting far below what other care providers are reimbursed for.
Providers who work with private insurance have voiced that reimbursement rates can be “insulting.” It also doesn’t help that rates haven’t significantly increased in decades.
Given the overhead costs of maintaining licensure and owning or participating in a private practice, these low rates are unsustainable. What’s more, salaried therapists in community rehabilitation centers often make even less, as little as $30,000 a year.
The end result is that the profession isn’t a financially attractive path to take, contributing to the therapist shortage.
Insurance is a pain to deal with, too.
Beyond the pay, the logistical challenges that come with insurance are another reason why mental health care providers often opt out.
For one, the administrative responsibilities add up. Filing insurance claims and advocating on behalf of a client requires a learning curve, all done in unpaid time. Getting credentialed with an insurance company is also time-consuming, and reimbursement isn’t immediate.
Insurers impact the care provided, too. For example, to receive reimbursement, therapists must make an official diagnosis. This can be problematic because mental health diagnoses are not always helpful for treatment. Clients may not even meet diagnostic criteria, especially during the first few sessions. Yet, diagnoses remain permanent in health records regardless.
Insurers can then also dictate how much care they will pay for, such as the number of sessions or the length of the sessions. Those decisions don’t always align with what the therapist and client know is necessary for healing.
The alternative: paying more out-of-pocket
For these reasons, clients are often left paying cash and seeking reimbursement from their plan for an out-of-network visit, if their plan even offers any out-of-network therapy coverage. Sometimes therapists offer sliding payment scales based on the client’s financial situation, for which an affordable rate is agreed upon by both the therapist and client.
Still, these options often mean higher out-of-pocket costs compared to having in-network insurance coverage or paying to see a primary care provider.
While mental health care parity is the goal, we are clearly far from it. To this day, insurers unlawfully delay and deny coverage, perhaps to encourage patients with chronic mental illnesses – who are more expensive to cover – to drop coverage or switch to another insurer.
We are in the throes of a mental health crisis as a nation. With care out of reach for so many though, solving the crisis feels unattainable. Paying mental health workers more, incentivizing insurance acceptance, and increasing reimbursement rates may alleviate some of the access burden.
Mental health has been undervalued as a profession, a policy priority, and an important part of overall health for far too long. The effects of unaffordable access to care are not going away, especially as demand for care grows and the workforce struggles to keep up. It’s time we listen to the voices of both those providing and receiving care, and treat mental health like any other form of care.
The post Your Therapist Doesn’t Accept Insurance? Here’s Why. first appeared on The Incidental Economist.February 11, 2025
Physician Tenure and Clinical Productivity
Health care systems nationwide face challenges in recruiting and retaining physicians, leading to high turnover and impact on patient care. Research also shows that new employees are often less productive than more experienced colleagues. If newly hired physicians take a long time to reach full productivity, the costs and effects of turnover on patient access may be greater than expected. Health systems may not be doing enough to ensure stable care during these transitions. Little research has examined how physician tenure affects productivity, leaving gaps in workforce planning and patient care strategies.
New Research
A recent retrospective cohort analysis published in the Journal of General Internal Medicine examined the relationship between physician tenure and clinical productivity in the Veterans Health Administration (VHA). The paper explored how tenure length affects productivity (i.e., the number of patient encounters per clinic day) among attending physicians. It also compared productivity trends between internally hired physicians—those who had any residency or fellowship training within the VHA—and externally hired physicians.
Methods
Researchers used the VHA’s Corporate Data Warehouse to collect detailed data on physician employment characteristics, specialty, and monthly patient encounters. Data was analyzed from 34,878 attending physicians across 27 specialties, covering over 1.5 million physician-months of outpatient encounters between October 1, 2017, and August 1, 2023. They used statistical models to examine productivity differences over time, adjusting for factors such as specialty, facility, and time effects, and sensitivity analyses to test the robustness of the results. The analyses were conducted for both the entire sample including all 27 specialties and four specialty subgroups—primary care, psychiatry, large medical specialties, and large surgical specialties.
Main Findings
Newly hired physicians had on average 1.72 fewer patient encounters per clinic day during their first quarter compared to their more experienced colleagues who had worked at VHA for more than two years. However, this productivity gap shrunk over time, with new hires having only 0.44 fewer encounters per clinic day by their eighth quarter. Among the specialty subgroups, medical and surgical specialty new hires reached productivity equivalent to more experienced employees by their eighth quarter. Additionally, physicians who had any residency or fellowship training within VHA (“internal hires”) had higher initial productivity and a quicker adjustment to full productivity than those hired externally, particularly in primary care and large surgical specialties.
Conclusion
These findings suggest that while newly hired attending physicians initially exhibit lower productivity, they experience significant improvement within the first two years. Moreover, those with prior VHA training adapt more quickly, highlighting the potential benefits of internal training programs. These insights are important for health care systems assessing the long-term costs and access implications associated with physician turnover and onboarding. Understanding these dynamics can aid in developing strategies to support new physicians, optimize training programs, and ultimately enhance patient care within VHA and similar health care settings.
The post Physician Tenure and Clinical Productivity first appeared on The Incidental Economist.February 10, 2025
There’s a way to deal with brain injuries in football. It isn’t safety gear.
Tackle football and the National Football League (NFL) are heralded by most Americans as a staple of our country’s culture. It’s no wonder the Super Bowl breaks records for television viewership every year, for the game and the halftime show alike.
Americans also know that football comes with head injuries, concussion, and even fatal illness like chronic traumatic encephalopathy (CTE). It’s a fact many of us have come to accept, sending our kids ourselves into play each season, knowing the risks.
That has seemingly changed in recent years with the slow rise of protective equipment like the Guardian Cap and the Q-Collar. While uptake of this equipment is low so far, the NFL and others are praising its ability to protect athletes and make the game safer. The NFL also celebrated a decrease in concussions in 2024.
But the bottom line is that no piece of equipment can prevent head injury in football. We should try to better respond to injury for both youth and professional athletes alike instead.
TIE contributor Katherine O’Malley wrote about this in Harvard Public Health Magazine last week ahead of the big game.
You can read the full piece here.
The post There’s a way to deal with brain injuries in football. It isn’t safety gear. first appeared on The Incidental Economist.February 5, 2025
Use of High-Risk Medications Among Older Adults Enrolled in Medicare Advantage Plans vs Traditional Medicare
When it comes time to visit a doctor, it’s common to have many priorities. Maybe it’s getting relief for that aggravated pickleball injury, taming a lingering cough or finally having that weird mole checked out [you really should]. Oftentimes the risks associated with our medications are not high on the priority list, but they should be.
While any medication has risks, understanding and managing those risks is more important for some prescription medications than others. High-risk (or high-alert) medications (HRMs) are those that present extreme danger either due to patient characteristics (e.g., age, chronic disease, etc.) or misuse. As such, HRMs require prescribers and health systems to employ a number of practices and tools to evaluate and mitigate risk towards improving patient safety.
Given their prevalence, there is mounting interest about prescribing practices of HRMs and the implications for health care.
Recent Study
In a study published in JAMA Network Open, evaluators from Harvard University and Boston University compared HRM prescribing trends between traditional fee-for-service Medicare (TM) and Medicare Advantage (MA), which are privately managed plans for Medicare eligible individuals that are publicly funded through a capitated payment arrangement.
To complete their analysis, the authors compared over 13.7 million matched pairs of beneficiaries taken from samples spanning 2013-2018. The study relied on several sources to obtain data on the sample population, including the Medicare Master Beneficiary Summary file, Social Vulnerability Index, U.S. Office of Management and Budget, and the Medicare Part D Master Beneficiary Summary File.
For its primary measure, the study relies on the Healthcare Effectiveness Data and Information Set (HEDIS) and its Use of High-Risk Medications in Older Adults (DAE) metric. As a primary outcome, the authors considered the total number of HRMs that were prescribed to the qualified enrollees. As a secondary outcome, the authors looked at the proportion of older enrollees who had been prescribed at least 1 HRM per year. Other outcomes included the proportion of enrollees who had received 2 or more HRMs per year or the same HRM twice in the same year.
In addition to the primary variable of Medicare insurance type (i.e., enrollment in TM vs. MA), the study also examined a number of covariates. The researchers considered age, sex, race and ethnicity, dual-eligibility status, rurality, social vulnerability, eligibility for Medicare’s low-income subsidy, and a patient health indicator that factors the number of non-HRM medications.
The authors first used linear regressions to construct their primary model, and after accounting for covariates and other effects (fixed and random), they plotted the adjusted rate of unique HRM prescriptions. After the secondary outcomes were plotted similarly, sensitivity analyses were completed according to a range of criteria.
Ultimately, the study found that the rate of HRM use decreased in each year of the study period (2013-2018) – this was true for both TM and MA alike. Consistent with previously observed prescribing trends, HRM use in MA was significantly lower than in TM, but the gap between the two had narrowed. In the final year of the study period, the rate of HRM use in TM was still 56.9 HRMs (per 1000 beneficiaries) compared to 41.5 in MA. Similar patterns were observed in the analyses of the secondary outcome of the proportion of enrollees who had been prescribed at least 1 HRM per year. When compared with TM, MA performed better with a lower adjusted proportion of beneficiaries who had been prescribed at least 1 HRM (3.9%) versus 5.3% in TM. Relative to patient characteristics, the study observed higher rates of HRM use for certain population subgroups, including those who were female, American Indian or Alaska Native, or White.
Conclusion
The authors note several key limitations, including limiting analyses to only those medications identified by the DAE measure during the study period. The study was also unable to assess the extent that the HRM prescribing were clinically appropriate. The authors also explain that this work is limited by the use of MA as a single exposure and that only filled prescriptions were included in the analyses.
Despite these limitations, this study has implications for both medical practice and health care policy. As the study found that certain populations (female, American Indian or Alaska Native, and White individuals) received HRMs with greater frequency, there is a need to better understand how prescribers assess clinical presentation of these populations. The study’s findings also highlight how the mechanisms responsible for the overall decrease in HRM use in TM are not entirely known. The authors recommend that the Centers for Medicare & Medicaid Services explore additional avenues (e.g., tying HRM rates to reimbursement models) to narrow the gap between TM and MA relative to HRM rates.
Given their potential for harm, further research into HRM medication management strategies is an essential component of improving patient care and safety for older adults.
The post Use of High-Risk Medications Among Older Adults Enrolled in Medicare Advantage Plans vs Traditional Medicare first appeared on The Incidental Economist.February 3, 2025
Can We Engineer the Environment to Avoid Junk Foods?
Can we change our behavior by changing the environment? A lot of junk food is available in the checkout lanes at grocery stores. Most of us are susceptible to it, and just about everybody impulse buys a candy bar now and again. What happens when we control what’s available in checkouts? Does changing the environment change people’s behavior?
The post Can We Engineer the Environment to Avoid Junk Foods? first appeared on The Incidental Economist.January 29, 2025
Coastal Living May Endanger Your Life
Coastal living is a dream for many Americans, but the growing impacts of climate change are making it increasingly risky. In my recent piece for The Portland Press Herald, I explore how climate change is affecting coastal areas and those residents’ health. I also shed light on the solutions already in progress.
Read the full article here.
The post Coastal Living May Endanger Your Life first appeared on The Incidental Economist.January 23, 2025
Covid Vaccine Misinformation or Disinformation? Which Was Worse?
In May 2024 a set of articles were published in the journal Science that focused on the intersection of misinformation and social media. The results, while preliminary in the grand scheme of things, were really interesting (and maybe a little alarming).
The post Covid Vaccine Misinformation or Disinformation? Which Was Worse? first appeared on The Incidental Economist.Trump’s Return Puts Inflation Reduction Act in Jeopardy
With the rise in prescription drug prices in recent years, many Americans have been forced to choose between paying for medication and other necessities like rent or groceries. The passage of the Inflation Reduction Act in 2022 changed that for those on Medicare, providing some relief by capping costs for beneficiaries.
That progress is now in jeopardy with a new Trump administration that has voiced support for repeal of the Inflation Reduction Act’s protections. Doing so could also squash any hope for extending prescription drug price protections for a much larger portion of Americans: the privately insured.
I wrote about that for Public Health Post. Read the full piece here.
Research for this article was supported by Arnold Ventures.
The post Trump’s Return Puts Inflation Reduction Act in Jeopardy first appeared on The Incidental Economist.January 19, 2025
A Bit More on Physical Pendulum Isochronal Pivot Points
This is a follow-up post to this one, which you should (re)read if this topic is of interest to you and any of the following is unfamiliar. The same warning about mobile viewing applies: all square roots are over both numerator and denominator, despite how it may appear on a mobile device.
A physical pendulum with mass m and center of mass (CM) moment of inertia Icm pivoting at a point d from the CM has period T given by
T=2πIcm+md2mgdT = 2\pi \sqrt{\frac{I_{\text{cm}} + md^2}{mgd}}
with g being the acceleration due to gravity. The last post showed that T has the same value on two circles centered on the pendulum’s CM, one with radius d and one with radius d’, where d’ = L – d and
L=Imd
Here I = Icm+ md2. The CM-centered circles of radius d and d’ are composed of isochronal points. That is, the period is the same no matter which point on these circles the pendulum is pivoted about.
This post explores T as a function of d (or d’) and some properties of d.
How T Behaves as d Varies
T as a function of d has a shape as shown in the figure below, where the horizontal and vertical axes represent d and T, respectively.
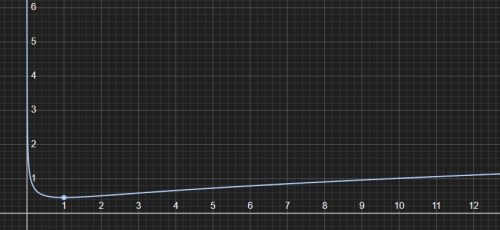
This suggests T approaches infinity as d approaches zero or infinity. This can be shown formally by taking limits, but it’s not hard to see informally by examining the expression for T.
As d approaches zero, the expression for T resembles (or behaves like) a constant times the inverse of the square root of d, which is asymptotic to the T-axis in the above plot and certainly goes to infinity. As d approaches infinity, the expression for T behaves like a constant times the square root of d, which also goes to infinity, as the graph shows.
This behavior of T as d approaches zero or infinity makes sense. As d approaches zero, the pendulum’s pivot point approaches its CM. There is no restoring torque at the CM, and the pendulum would not return from a displacement. Think of turning a disk of uniform density pinned at the center (its CM). If you give it a turn, it won’t turn back. That’s an infinite period.
As d approaches infinity, the situation resembles a simple pendulum, for which the period is proportional to the square root of its length (d), hence T also approaches infinity.
Moving away from these extremes, T strictly monotonically decreases to a minimum. This itself means that the minimum must be where d=d’. If this were not the case, then there would be two isochronal circles, centered on the CM, of minimum T, one of radius d and one of radius d’. This would imply that all pivot points a distance r from the CM such that dhave larger periods, which contradicts the strict monotonicity of T from zero (or infinity) to the minimum.
Or, we could take the derivative of T with respect to d and set it to zero (steps omitted) to find that the minimum T is where
d2=Icmmd^2 = \frac{I_{\text{cm}}}{m}
From the previous post, this is also the expression for dd’. That means that the minimum T is found where d and d’ coincide. This value of d is also the radius of gyration. By definition, this is the radius such that if all of m resided there, the moment of inertia would be the same as the object’s (here the pendulum) with distributed mass.
Plugging this into the expression for T given above, the minimum T (or, for convenience, T2) is
Tmin2=8π2gIcmm
So, when d=0, d’=∞ we have two (degenerate) isochronal circles for which T is infinite. As d moves radially outward from the CM, d’ moves inward, and the circles they define are always composed of isochronal points. As this happens, T drops from infinity toward a unique minimum proportional to the quartic root of Icm/m. The minimum is achieved when d=d’, at the radius of gyration, and the two isochronal circles become one (♥ cue violins ♥).
Where is the Minimum with Respect to the Pendulum?
Where is the d for which T is minimum with respect to the boundary of the pendulum? It’s never outside the boundary of the pendulum. I’ll show this mathematically, below, but it’s intuitive. Lengthening a simple pendulum, for which all the mass is at the end of the (assumed massless) support, increases its period. So, it stands to reason that a pivot point beyond the surface of a physical pendulum would have a larger period than a pivot point on its surface. Also, the definition of radius of gyration makes it pretty clear that it’s within the pendulum.
Let’s do it with math anyway. The pendulum’s CM rotational inertia is, by definition
Icm=∫r2 dmI_{\text{cm}} = \int r^2 \, dm
where r is the perpendicular distance from the CM to a infinitesimal mass element dm. Replacing r with rmax, the largest distance from the CM to the boundary of the pendulum, we get the inequality
Icm=∫r2 dm≤rmax2∫dmI_{\text{cm}} = \int r^2 \, dm \leq r_{\text{max}}^2 \int dm
Or, simply,
Icm≤rmax2 mI_{\text{cm}} \leq r_{\text{max}}^2 \, m
Substituting this into the expression for the T-minimizing d above, d ≤ rmax. Equality is obtained only when all the pendulum’s mass is at a constant radius from the CM (an idealized hoop of zero width). Otherwise, the T-minimizing d is strictly within the pendulum’s boundary. For all practical purposes (assuming there are any), d < rmax. That is, not only is the T-minimizing d not outside the pendulum, it’s not even on the surface (apart from the idealized hoop). It’s somewhere strictly inside the pendulum. That means that both d and d’ are within the boundary of the pendulum for some range.
If the body of the pendulum includes the CM (true for convex shapes like a disk or triangle), then all possible values of T, from its maximum of infinity to its minimum at the d defined above are found at pivot points within it. For all such values of T, there are arcs* of one or two isochronal circles within the body of the pendulum — one when d’ is outside the pendulum’s boundary and two when it is inside, which, as noted above, it will be for some range. In fact, that range is when d’ is between the T-minimizing d (the radius of gyration) and rmax.
If the body of the pendulum does not include the CM (as would be the case for some concave shapes like a uniform density banana or a washer), the maximum T for which a pivot point is inside the body of the pendulum is given by
T=2πIcm+mrmin2mgrminT = 2\pi \sqrt{\frac{I_{\text{cm}} + m r_{\text{min}}^2}{m g r_{\text{min}}}}
where rmin is the distance from the CM to the point within the pendulum closest to it.
Summary
The period of a physical pendulum, T, varies with pivot point from infinity (at pivot points CM and infinity) to a minimum at the radius of gyration.A minimum achieving pivot point is always within the body of the pendulum. If the body of the pendulum includes the CM, then for all possible values of T, from its minimum to infinity, there are arcs of one or two isochronal circles within the body of the pendulum.If the body of the pendulum does not include the CM, there are only isochronal circle arcs for T less then a finite maximum value, an expression for which we found.* I’m talking arcs of circles and not necessarily full circles here because there may be some radial distances from the CM for which the body of the pendulum exists for only some angles. Think of a triangular-shaped pendulum as opposed to a disk-shape one. For the former, there are some CM-centered circles of radius less than the extent of the triangle that aren’t entirely within the triangle. For the latter, this is not true.
The post A Bit More on Physical Pendulum Isochronal Pivot Points first appeared on The Incidental Economist.Aaron E. Carroll's Blog

- Aaron E. Carroll's profile
- 42 followers

