
William Davis's Blog: Dr. Davis Infinite Health Blog, page 57
January 3, 2019
Re-post: Make L. reuteri yogurt
People seem to be having a tough time locating the Wheat Belly Blog post in which I summarized how we make the L. reuteri yogurt, so I’m re-posting it. Remember: It’s NOT about yogurt; it’s about a means of amplifying the counts of a specific bacteria that possesses unique properties. To maximize bacterial counts, the recipe to make the yogurt therefore includes a prebiotic fiber and prolonged fermentation, very different from conventional yogurt. And, no, NONE of these benefits come from consuming conventional yogurt.
We make the yogurt with two strains of Lactobacillus reuteri ATCC PTA 6475 and DSM 17938, based on the detailed studies conducted at MIT and elsewhere, both experimental animal and human, that have suggested dramatic effects. Those effects include:
Complete shut-down of appetite, an “anorexigenic” effect, that can be used to facilitate intermittent fasting or break a weight loss plateau. This, along with an increase in metabolic rate, explain why weight loss results.
Dramatic increase in skin thickness and skin collagen, along with acceleration of skin healing, a surrogate for overall youthfulness and health. I’m a big fan of dietary collagen, such as those provided by collagen hydrolysates, bone broths/soups, slow-cooking meats, eating the skin on chicken and fish, etc. This L. reuteri strategy amplifies this effect considerably.
Increased oxytocin–A doubling of oxytocin blood levels was observed in mice, the effect responsible for the extravagant skin benefits, reduced insulin resistance, dramatic increases in testosterone in males, increased estrogen in females (magnitude unclear), thicker and more plentiful hair (though the consistency of this effect is not yet clear).Other studies have demonstrated substantial weight loss, especially from visceral fat, increased muscle mass, and increased bone density (protection from osteoporosis/osteopenia).
Put all these effects together—caloric reduction, increased skin health, increased bone density, fat loss, muscle gain, reduced insulin resistance, etc.—and you have one of the most powerful anti-aging, youth-preserving strategies I have ever come across.
Because the most robust data were generated using the ATCC PTA 6475 strain of L. reuteri and, to a lesser extent, the DSM 17938 strain, I have been confining my efforts to these strains. Other L.reuteri strains may mimic these effects, but we simply don’t know that for certain, as the studies have not been performed. Strain specificity can be a crucial factor. After all, all of us have several strains of E. coli in our intestines that live quietly and don’t bother anyone. But, get exposed to strains of E. coli from contaminated produce and you develop life-threatening diarrhea and kidney failure that can be fatal, especially in children. Same species (E. coli), different strains—strain specificity can be a critical factor.
So we start with L. reuteri ATCC PTA 6475 and DSM 17938 provided by the Swedish company, BioGaia, who has locked these species up with patents. Their product is called Gastrus. (Just Google “BioGaia Gastrus” to find a retailer.) Problem: There are only 100 million CFUs (live organisms) of each strain per tablet. I have not observed any substantial health benefits by ingesting the tablets.
So I have been amplifying bacterial counts by making yogurt. The counts are further increased by performing fermentation in the presence of prebiotic fibers. Just as ingesting prebiotic fibers increases bacterial counts in your intestines, so it goes in making yogurt, as well. It also yields a thicker, richer end-product. (I don’t know why EVERY commercial yogurt maker doesn’t adopt this practice, as the results are so much superior both in bacterial counts and in taste/texture.)
The yogurt is thick, delicious, and contains a marked increase in bacterial counts. (We are in the process of performing formal counts). Given the extraordinary thickness of the end-product, it is likely that trillions of CFUs are present, sufficient to convert the soupy liquid of your starting milk, half-and-half, cream, coconut milk or other starter to rich, thick yogurt, sometimes thick enough to stand up on a plate. People who consume 1/2 cup per day of this preparation (mixed with blueberries, strawberries, etc.) are reporting the effects listed above. And this yogurt is so much richer and better tasting than products you buy in grocery stores.
There are probably many ways to make this yogurt and yield the bacterial counts you desire. But this is how I do it:
1 quart of organic half-and-half (or cream, whole milk, canned coconut milk, goat’s milk/cream, sheep’s milk/cream)
2 tablespoons inulin or unmodified potato starch or other prebiotic
10 tablets of BioGaia Gastrus, crushed
The probiotic tablets can be crushed using a mortar and pestle or other hard object (clean stone, bottom of a thick drinking glass, rolling pin, etc.). Don’t worry: The end-product should have little remaining sugar, as it is fermented to lactic acid. (If in doubt, just let it ferment a few more hours.) Just as the cucumbers you grow in your garden were fertilized with cow manure but ripe cucumbers contain no cow manure, so the final fermented yogurt product should contain little to no sugar.
(Coconut milk is tougher to work with. If you use coconut milk, you will need to add sugar, e.g., one tablespoon, to the prebiotic or use more sugar in place of the prebiotic, as there is no lactose to ferment in coconut milk. You will also need to preheat the coconut milk in a saucepan to 180 degrees F; add 3 tablespoons powdered gelatin and stir until dissolved; cool to 100 degrees F, then use a stick blender for 30-40 seconds to emulsifying the oil; add crushed tablets or two tablespoons of a prior batch.)
In large glass/ceramic bowl, combine 2 tablespoons of liquid with the inulin or other prebiotic and the crushed probiotic tablets (or two tablespoons of yogurt from a prior batch). We start by making a slurry, as inulin or potato starch will form hard clumps if added to the entire volume. Mix thoroughly by hand and make sure the prebiotic and sugar are dissolved. Then add the remaining liquid and stir.
Maintain the mixture at 100 degrees F. This can be accomplished with a yogurt maker, Instant Pot, sous vide device, rice cooker, or any other device that allows maintaining a continual temperature in this range. I use my oven: Turn onto any temperature, e.g., 300 degrees, for about 60-90 seconds, just until a desert-hot temperature is reached. Turn off the oven; repeat every 4-6 hours—not precise, but it works fine when using dairy for fermentation. I used a yogurt maker and sous vide with good results. Of all your choices, the sous vide is the easiest and most foolproof. (Some other devices have too high a temperature setting that kills L. reuteri that is not as heat tolerant as some other microbes used to ferment yogurt.)
The first batch tends to be a bit thinner with curdles, but subsequent batches tend to be thicker and smoother. To make subsequent batches, reserve a few tablespoons from the prior batch and use in place of crushed tablets, since your yogurt should contain plentiful microbes.
We then consume 1/2 cup per day. I have mine with fresh or frozen blueberries and a squirt of stevia. The end-result should be thick and delicious, better than anything store-bought.
If you give it a try, be sure to come back and report your experience. If you are encountering difficulty, see this troubleshooting guide.
The post Re-post: Make L. reuteri yogurt appeared first on Dr. William Davis.


December 29, 2018
The Next Wheat Belly 10-Day Grain Detox Begins Wednesday, January 9th

Put it off no longer: We are planning our next Wheat Belly 10-Day Grain Detox Challenge that starts on Wednesday, January 9th. This is your opportunity to seize control over health and weight, maybe even turn the clock back 10 or 20 years, look and feel better, be freed of numerous, if not all, prescription drugs.
In addition to our Wheat Belly 10-Day Grain Detox Private Facebook page that provides videos, success stories, and plenty of feedback and answers to your questions, the next Detox Challenge will also include:
1) LIVE Facebook sessions with Dr. Davis and April Duval, our main Facebook page administrator. I will personally kick off the Detox Challenge on Jan 9th. And because April is herself an example of a fabulous Wheat Belly Detox success, she knows the ins and outs of this lifestyle like the back of her hand.
2) Free access to the Suggestic smartphone app for the first 7 days of the Detox— The Suggestic iPhone app helps you navigate the Wheat Belly Detox with even more recipes, daily suggested recipes, a restaurant locator to identify eating places consistent with our lifestyle with suggested menu items, the ability to track health measures such as water intake and sleep, and all personally customizable. It is your chance to get acquainted with the useful Suggestic app while helping you succeed on your Wheat Belly 10-Day Grain Detox.
Here’s what you do:
Visit wheatbelly.suggestic.com/challenge by Jan 9th
Sign up to get 7-day free access to my challenge on the Suggestic app
On Jan 9th, go to the app’s homepage and tap “start program” so we can start the challenge together
Our goal: to help you succeed in turning around your life and health and achieve all your health goals including weight loss, getting off prescription medications, and turning back the clock 10 or 20 years.
Why the Detox Challenge?
Through my New York Times bestseller, Wheat Belly, millions of people learned how to reverse years of chronic health problems by removing wheat from their daily diets. But, after reading the original Wheat Belly or the Wheat Belly Total Health book, or even using the recipes from the Wheat Belly Cookbook and Wheat Belly 30-Minute Cookbook, people still said: “I’ve read the books, but I’m still not sure how to get started on this lifestyle.”
That’s why I wrote the Wheat Belly 10-Day Grain Detox and now help readers along in this Wheat Belly 10-Day Grain Detox CHALLENGE. This is the quickest, most assured way to get started on regaining magnificent health and slenderness by adopting the Wheat Belly lifestyle.
We are kicking off the next Wheat Belly 10-Day Grain Detox Challenge on Facebook LIVE on Day 1: Wednesday January 9th, 12pm EST/11 am CST/10 am MT/9 am PT. Come join us on the private Wheat Belly 10-Day Grain Detox Facebook page: https://www.facebook.com/groups/52751...
You will also be given free access to the Wheat Belly 10-Day Grain Detox Suggestic smartphone app for the first 7 days of the Detox!

The Wheat Belly 10-Day Grain Detox supplies you with carefully designed meal plans and delicious recipes to fully eliminate wheat and related grains in the shortest time possible. Perfect for those who may have fallen off the wagon or for newcomers who need a jump-start for weight loss, this new addition to the Wheat Belly phenomenon guides you through the complete 10-Day Detox experience. And we will kick off this next Challenge with a live Facebook session with Dr. Davis!
In addition to this quick-start program, I’ll teach you:
How to recognize and reduce wheat-withdrawal symptoms,
How to avoid common landmines that can sabotage success
How to use nutritional supplements to further advance weight loss and health benefits
The Wheat Belly 10-Day Grain Detox also includes:
Inspiring testimonials from people who have completed the program (and have now made grain-free eating a way of life)
Exciting new recipes to help get your entire family on board
To join the Detox Challenge:
Step 1
Get the book. And read it (at least the first 5 chapters).
Detox Challenge participants should be informed and active in order to get the most out of the challenge and private Facebook group. READING THE WHEAT BELLY DETOX BOOK IS REQUIRED TO PARTICIPATE. PLEASE DO NOT PARTICIPATE IF YOU HAVE NOT READ THE BOOK or else the conversations will not make sense and you will not enjoy full benefit. It is a very bad idea to try and piece the program together just from our conversations. (Note that the Wheat Belly Detox program is NOT laid out in the original Wheat Belly book.)
Amazon: http://amzn.to/1JqzMea
Barnes & Noble: http://bit.ly/wheatbelly10daygraindetox-bn
Indiebound: http://bit.ly/1KwcFTQ
Step 2
Come join the Private Facebook Group.
http://bit.ly/WheatBelly-PrivateFBGroup
Step 3
Head back to the Private Facebook Group starting Tuesday, January 8th (the day before the official start of the Challenge) and onwards for tips, videos, and discussions to help you get through your detox and reprogram your body for rapid weight loss and health. Dr. Davis and site administrator, April Duval, will be posting video instructions and answers to your questions.
The post The Next Wheat Belly 10-Day Grain Detox Begins Wednesday, January 9th appeared first on Dr. William Davis.
December 28, 2018
Reduce HIGH TRIGLYCERIDES naturally and safely . . . without scam products

High triglyceride levels are as common as muffin tops and man breasts. You will find a triglyceride level among the four values on any standard cholesterol panel. High triglycerides are either ignored by most doctors or reflexively “treated” with drugs, such as fibrates (Lopid, fenofibrate), prescription fish oil (Lovaza, Vascepa) and, of course, statins. But buried in this single triglyceride value is tremendous insight into diet, metabolic efficiencies, and cardiovascular risk, with control using natural, non-medication means easy to accomplish with absolute NO need for overpriced Big Pharma scam products.
Why are triglycerides important? Triglyceride levels of 60 mg/dl or higher will:
Block insulin, thereby adding to weight gain and higher blood sugars
Cause formation of small LDL particles. Triglycerides occur in the bloodstream mostly as Very Low-Density Lipoproteins, VLDL, that interact with other lipoprotein particles. Abundant triglycerides in VLDL encounter LDL particles and make them triglyceride-rich. This leads to yet another process that leads to formation of small LDL particles that causes coronary heart disease and heart attack. Key point: It’s triglyceride availability that drives cardiovascular risk.
At triglyceride levels above normal, pancreatic beta cells that produce insulin are subject to lipotoxicity, irreversible damage from triglycerides that can lead to inadequate insulin production by the pancreas over time.
At very high triglyceride levels above 1000 mg/dl, triglycerides cause pancreatitis, pancreatic inflammation that damages delicate pancreatic tissues.
The higher the triglycerides, the higher the cardiovascular risk. Labs typically quote 150 mg/dl or higher as the cutoff for “normal,” but this is not true: a level of 150 mg/dl is associated with a substantial quantity of the above metabolic distortions. Only at 60 mg/dl or below do all unhealthy triglyceride-related abnormalities revert to normal or ideal.
What causes triglycerides to rise?
First of all, dietary fats are triglycerides by definition. Fat on pork or beef, olive oil, coconut oil, and butter are all triglycerides. When we consume fats and oils, there is therefore a modest and nearly immediate rise in blood triglycerides as particles called chylomicrons, large particles formed by the intestinal tract to “package” fats for digestion. Chylomicrons are cleared rapidly and efficiently by the liver over several hours. In most people, fat intake is—counterintuitively—only a minor contributor to blood triglyceride levels, a non-contributor to high fasting triglycerides.
There are two processes that are much larger determinants of both fasting and after-meal (“postprandial” or “non-fasting”) triglyceride levels:
Carbohydrates in the diet are converted to triglycerides by the process of liver de novo lipogenesis, the creation of fat from carbohydrates. This is also the process that leads to fatty liver, as some of the triglycerides manufactured remain in the liver.
Whenever the liver has fatty acids delivered to it, it manufactures triglycerides (each triglyceride molecule contains 3–tri–fatty acids). Visceral fat–deep abdominal fat in the abdomen–is resistant to insulin and thereby provides a continual flow of fatty acids to the liver, a process that runs 24 hours a day.
These last two processes yield much greater rises in both fasting and postprandial triglycerides than that provided by dietary fat. These two processes explain why, for example, someone has a triglyceride level of 210 mg/dl fasting, 400 mg/dl 6 hours after eating.
Understanding these phenomena thereby lead us to practical dietary and natural methods to reduce triglycerides to a level of an ideal level of 60 mg/dl or less:
Eliminate grains and sugars—Contrary to the conventional advice to reduce fat and eat plenty of “healthy whole grains,” the amylopectin A carbohydrate unique to grains provides dietary carbohydrates that fuel liver de novo lipogenesis. High blood sugars that result from grain amylopectin A also lead to insulin resistance. The result: high triglycerides. Eliminate grains and sugars and both processes unwind quickly and dramatically. Most people need to also limit carbohydrate consumption to no more than 15 grams net carbohydrates per meal (net carbs = total carbs – fiber) to further prevent liver de novo lipogenesis from proceeding. Do not reduce dietary fat, as this raises triglycerides substantially. (Personally, when I was an ultra low-fat vegetarian 25 years ago, my triglycerides rose to 350-390 mg/dl; they are now in the 40’s.)
Reverse insulin resistance—Beyond grain and sugar elimination, vitamin D restoration, getting adequate sleep, magnesium, and physical activity all help reverse insulin resistance. A very quick way to reverse insulin resistance is through intermittent fasting, fasting for periods of 15-36 hours (while hydrating more than usual). Salting your food also helps reverse insulin resistance—yes, another natural health practice contrary to prevailing health advice. Reversing insulin resistance reduces visceral fat over time, further amplifying triglyceride-reducing benefits.
Supplement omega-3 fatty acids from fish oil—The EPA and DHA of fish oil activate the enzyme lipoprotein lipase that helps accelerate clearance of both postprandial chylomicrons and VLDL particles. This does not apply to the omega-3 fatty acid, linolenic acid, from chia, flaxseed, or walnuts, nor can it be accomplished by the trivial quantity of EPA and DHA in krill oil; it must come from fish oil. It also requires greater supplemental total daily intakes of 3000-3600 mg EPA + DHA per day (divided into two doses). And not only do you not need the 10-fold more costly prescription fish oil, you can actually purchase fish oil that is superior to prescription fish oil (such as the liquid triglyceride form found in Nordic Naturals). And the prescription form that only contains EPA? What about brain health and protection from dementia that comes mostly from DHA that is not present in an EPA-only product? Use fish oil in the way it occurs in fish: both EPA + DHA and ignore absurd pharmaceutical marketing.
Cultivate healthy bowel flora—“Feeding” bowel microorganisms the fibers they need to convert fiber into butyrate, a fatty acid that yields metabolic effects that include reduction of insulin resistance, reduced blood sugar, reduced LDL values, and reduced triglycerides. This important strategy is discussed further in this Wheat Belly Blog post, as well as a full discussion in Wheat Belly Total Health and Undoctored books.
Fibrate drugs, statins, and prescription fish oil are absolutely not necessary to reduce triglycerides. This is yet another example (among many) of how the pharmaceutical industry manages to persuade gullible physicians to prescribe drugs, not to fix the cause. I managed many complex hyperlipidemias that included many people with high triglyceride levels for years with triglyceride results superior to that achieved with drugs.
The post Reduce HIGH TRIGLYCERIDES naturally and safely . . . without scam products appeared first on Dr. William Davis.
December 23, 2018
ZERO tolerance for hypoglycemia

As more and more type 2 diabetics discover the Wheat Belly and other low-carb lifestyles, they are also discovering how rapidly and easily blood sugars drop.
As diabetics become less diabetic–a process that can occur VERY quickly, often within 24 hours of removing all wheat/grains from their diet–but they are taking insulin or certain diabetes drugs, there is potential for hypoglycemia or low blood sugar. Low blood sugar from diabetes drugs can be dangerous and should be avoided at all costs. (Imagine if a non-diabetic started administering insulin or blood sugar-reducing drugs–it would result in life-threatening low blood sugars.)
Unfortunately, you cannot always rely on your doctor. Most physicians are unschooled in how to cure diabetes and therefore how to manage the hypoglycemia that may develop on your way to cure. (They are very good at CAUSING diabetes, however, prescribing diets like “an 1800-calorie American Diabetes Association diet,” a typical dietary order in the hospital that RAISES blood sugar to sky-high levels.) It is nonetheless important to at least discuss your questions with your doctor. (If you encounter resistance, get a new doctor, preferably one in functional medicine who is more likely to understand nutrition and biochemistry.)
So I reprint a section I wrote for the Wheat Belly Cookbook that details some of the important issues to be aware of if you are diabetic on insulin or diabetes drugs and remove wheat/grains from your diet:
“There is not a shred of evidence that sugar, per se, has anything to do with getting diabetes.”
Richard Kahn, PhD
Retired Chief Scientific & Medical Officer
American Diabetes Association
Dr. Kahn’s comment echoes conventional thinking on diabetes: Eat all the grains and candy you want . . . just be sure to talk to your doctor about diabetes medications.
If you eat foods that increase blood sugar, it increases your need for diabetes medications. If you reduce or eliminate foods that increase blood sugar, then it decreases your need for diabetes medications. The equation for most people with adult, or type 2, diabetes, is really that simple.
But several precautions are necessary if you are diabetic and are taking certain diabetes drugs. The potential danger is hypoglycemia, low blood sugars (e.g., less than 70 mg/dl) . . . as well as the uninformed objections of many doctors who have come to believe that diabetes is incurable, irreversible, and a diagnosis for life.
Some medications, such as metformin (Glucophage), pioglitazone (Actos), rosiglitazone (Avandia), and acarbose (Precose), rarely if ever result in hypoglycemia when taken by themselves. They are effective for preventing blood sugar rises, but tend to not generate blood sugar lows.
However, other medications, especially glyburide (DiaBeta, Micronase), glipizide (Glucotrol), glimepiride (Amaryl), and various insulin preparations can cause severe and dangerous hypoglycemia if taken while reducing or eliminating wheat and carbohydrates. For this reason, many people eliminate these oral drugs or slash insulin doses by 50% at the start, even if it means some temporary increase in blood sugars. The key is to avoid hypoglycemia as you consume less food that increases blood sugar, even if it means higher near-term blood sugars.
Other medications, such as sitagliptin (Januvia), saxagliptin (Onglyza), linagliptin (Tradjenta), exenatide (Byetta) and liraglutide (Victoza) usually do not result in hypoglycemia but occasionally can, especially if taken in combination with other diabetes drugs.
Because of the complexity of these responses, you should ideally work with a healthcare provider adept at navigating these issues as you become less and less diabetic. Problem: Most doctors and diabetes educators have no idea whatsoever how to do this, as they will tell you that, once you have diabetes, you will always have it and trying to get rid of it is fruitless and foolhardy (to the appreciative applause of the diabetes drug industry). So don’t be surprised if you are left on your own. At the very least, you want to check to see if your doctor will work with you and, if not, at least try and find another who will. Also, frequent monitoring of blood sugars is essential. I tell my patients on the path to becoming non-diabetic that high blood sugars (though maintained below 200 mg/dl) are preferable to low blood sugars (below 100 mg/dl) in this transition period. If, for instance, you are obtaining blood sugars in the morning (fasting) of 100 mg/dl, it is time to further reduce or eliminate a medication, such as glipizide or Lantus insulin taken at bedtime.
Even better, adhere to the Wheat Belly No Change Rule, i.e., allow no rise in blood sugar pre-meal and 30-60 minutes after the start of the meal. If there is a rise from, say, 120 mg/dl to 150 mg/dl, then you have eaten something you shouldn’t have eaten. Next time, either eliminate or cut the portion size of the carbohydrate food that you consumed. (This is to be distinguished from the conventional advice to check a 2-hour post-meal blood sugar–this is to assess response to insulin or diabetes drug to assess whether there is a return to baseline, something that we are NOT concerned with.)
Any diabetic who wants to better understand the details of becoming non-diabetic would also benefit from knowing about the resources of Dr. Richard Bernstein, author of The Diabetes Solution. The critical issue here is to understand that many people with diabetes have been told that they have an incurable condition for a lifetime and that a diet rich in “healthy whole grains” is essential—-advice that ensures you remain diabetic. Do the opposite─-eliminate “healthy whole grains,” especially the most dangerous grain of all, wheat─-and limit other carbohydrates, including non-wheat grains like millet and quinoa, and diabetes unwinds itself with reduced fasting blood sugars and HbA1c in the majority.
The post ZERO tolerance for hypoglycemia appeared first on Dr. William Davis.
December 22, 2018
The Perfect Gift

This holiday season we are all in search of the perfect gift. What is the one thing you truly desire for yourself and your family? Don’t you think we all want it? What if you were handed a beautifully wrapped box containing a miraculous tool that caused dramatic weight loss without limiting calories or requiring exercise?
What if this gift reduced appetite, shrunk belly fat, dropped your dress size into the single digits, and accomplished all of this while sparing you from a Biggest Loser sob fest?
What if that same gift freed you from acid reflux, heartburn, bowel urgency, and diarrhea, but also improved mood, increased energy, deepened sleep, and reduced or eliminated joint pain? And all of this makes you look and feel younger and desirable.
What if this gift would make you look & feel younger, desirable, even improved your libido?
What if this gift also reversed skin conditions such as seborrhea, eczema, psoriasis, acne, dandruff and earned you compliments on the smoothness of your skin? What if chronic sinus congestion, sinus infections, and asthma were brought to a halt and you were freed from the repeated need for antibiotics and inhalers?
What if that same little box contained a gift that, if used every day, reversed serious inflammatory conditions such as rheumatoid arthritis, Crohn’s disease, and ulcerative colitis?
What if this gift could also replace cholesterol drugs, blood pressure drugs, diabetes drugs, anti-inflammatory drugs, antidepressants, and acid reflux drugs while reducing cholesterol values, blood sugars, and inflammation— eliminating your need for dozens of prescription medications, not to mention their unwanted side effects?
And, what if this same mysterious gift not only made you feel better than you have in years, but also had the potential to help you achieve a physical makeover that made you look 10, even 20, years younger without Botox, filler injections, surgery, or without any unwanted health consequences?.
This gift is the blueprint for a grain-free life enjoyed in good health.
You can have it and the best part is you can share it as well!
The complete blueprint for a grain-free life is detailed in the Undoctored, Wheat Belly Total Health and Wheat Belly 10-Day Grain Detox books.
Wishing you a happy and healthy holiday season!
Dr. William Davis
PS. The next Wheat Belly 10-Day Detox Challenge begins on January 9th. Details will be available soon.
The post The Perfect Gift appeared first on Dr. William Davis.
December 21, 2018
Health lessons from the last North American hunter-gatherer
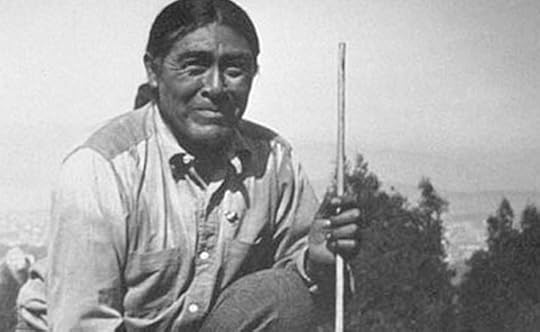
One of the last true hunter-gatherers in North America was believed to be a man called Ishi with a fascinating tale of the clash between indigenous cultures and early 20th century America. A study of this man provides some insights into the lives of people living something close to a pre-Neolithic lifestyle, i.e., a life without agriculture, grains, and processed food.
“An aboriginal Indian, clad in a rough canvas shirt which reached to his knees … was taken into custody last evening by Sheriff Webber and Constable Toland at the Ward Slaughter-house on the Quincy road. He had evidently been driven by hunger to the slaughter-house, as he was almost in a starving condition …
The most plausible explanation seems to be that he is probably the surviving member of the little group of uncivilized Deer Creek Indians who were driven from their hiding place two years ago.
In the Sheriff’s office he was surrounded by a curious throng. He made a pathetic figure crouched upon the floor … His feet were as wide as they were long, showing plainly that he had never worn either moccasins or shoes … Over his shoulder a rough canvas bag was carried. In it a few Manzanita berries were found and some sinews of deer meat. By motions, the Indian explained that he had been eating these.”
The Oroville Register
August 29, 1911
Such was the reception the lone man received upon being trapped by turn-of-the-20th century Californians. As details were pieced together, it appeared that Ishi—-a Yahi Indian word for “man,” a name assigned to him, since it was customary to not use personal names in their culture else risk insult and invite bad magic—-was as close as anyone could come to a true primitive in a modern world, someone entirely unfamiliar with all the modern developments around him, having lived a life of virtually pure hunting and gathering his entire life. Yet the story of Ishi encapsulates many of the same phenomena we witness over and over again in the collision of primitive Homo sapiens with modern diet.
Following Ishi’s recovery, in an unprecedented decision the U.S. Bureau of Indian Affairs acquiesced to a peculiar request made by two University of California anthropologists, Drs. Alfred L. Kroeber and Thomas T. Waterman, to release the “wild man” to the charge of the University’s Museum of Art and Anthropology. Kroeber and Waterman then proceeded to provide Ishi with food, shelter, and protection, while studying his every habit and behavior.
As he learned to speak broken English and his anthropologist attendants learned to understand bits and pieces of Ishi’s native tongue, several details became clear: Ishi was the last surviving member of the Yahi Indian tribe, nearly exterminated during a massacre by marauding settlers eager for land in 1865, leaving only five survivors. Of those five were Ishi, his mother, sister, his sister’s husband, and a child. After many years of living in the wild, Ishi was the lone survivor. He continued to live much as his tribe’s ancestors had by hunting animals and fish and gathering wild vegetation.
Dr. Saxton T. Pope, a physician, recorded a thorough physical examination of Ishi: “He was born probably about 1860 in northern California, consequently is approximately 54 years of age, but appears about 45… Musculature is well developed, with an even distribution of subcutaneous fat. The teeth are all present, strong, colored slightly brown, no evidence of decay or pyorrhea… His breath is sweet and free from the fetor common to the average white man…”
As Ishi’s time in Western society progressed, Dr. Pope made a number of other interesting observations: “He fed at the nearby Hospital and had at least two full meals daily, besides a luncheon of his own preparation. This was greatly in excess of any dietary heretofore possible to him. In consequence he increased in weight rapidly and became ungracefully fat.” Through it all, surely an unsettling shift from his hunter-gatherer origins to that of laboratory specimen, though civilly treated, Ishi was “always calm and amiable — he had the most exacting conscience concerning the ownership of property. He was too generous with his gifts of arms, arrowheads, and similar objects of his handicraft — With those whom he knew and liked he was remarkably talkative, rambling off into stories, descriptions, humorous episodes, and many unintelligible tales.” In short, despite the traumatic excision from his life and culture suffered at the hands of modern people, Ishi maintained a sense of humanity that charmed the people around him until his death from tuberculosis (a disease of the “white man”) in 1916.
The tragic and fascinating tale of Ishi is about as close as we get in our time to viewing what a nearly pure North American hunter-gatherer was like prior to the dietary acculturation that has now come to touch virtually every other human on earth.
Reference:
Ishi: The Last Yahi: A Documentary History. Heizer RF, Kroeber T, eds. Berkeley: University of California Press, 1979.
The post Health lessons from the last North American hunter-gatherer appeared first on Dr. William Davis.
December 19, 2018
The Bovine Guide to Healthy Eating

Grains are seeds of grasses. They, along with the Kentucky bluegrass and rye grass in your lawn, are plants from the family Poaceae, the grasses of the earth. Grasses are so ubiquitous and prolific that creatures have evolved that are able to survive by consuming them as their main source of food.
Ruminants such as cows, goats, sheep, giraffes, gazelle, and antelopes are able to digest grasses because they have undergone extensive evolutionary adaptation over millions of years that allow them to subsist on grasses as a food supply. For instance, ruminants:
Grow teeth continuously to compensate for the wear caused by sand-like particles, or phytoliths, in grass blades. They also lack upper incisors, replaced by a bony dental pad on the top of the mouth to help seize hold of grasses. In contrast, you, a non-ruminant, grow teeth twice in a lifetime, only during childhood and adolescence, and have proud bite-worthy incisors.
Produce copious quantities of saliva. A cow typically produces 100 quarts or more saliva per day, compared to our 1 meager quart.
Have 4-compartment stomachs to break down the cellulose of grasses. You have a 1-compartment stomach.
Regurgitate grasses to chew as a cud. While you may have the urge to chew, it certainly is not for regurgitated wads of grass fiber.
A lengthy spiral colon that provides greater digestive exposure to further break down the components of grasses, unlike our relatively short colon with a couple of 90-degree turns.
Harbor unique microorganisms in their 4-compartment stomachs and spiral colons that express the cellulase enzyme and other enzymes to break down the otherwise indigestible components of grasses. We have a relatively sterile stomach and upper small intestine with virtually no microorganisms that express a cellulase enzyme. While our colons harbor microorganisms, they cannot digest any substantial quantity of cellulose.
If you, proud member of the non-ruminant species Homo sapiens, were to grasp a stalk of 18-inch tall semi-dwarf wheat, you can’t eat the roots, nor the stalk, leaves, or husk. You can, however, isolate the seeds, remove the husk, then dry, pulverize, and heat them. You will then have something–porridge or flour–that can yield something you might view as food. But seeds, just like the rest of the plant, have components that are indigestible, such as wheat germ agglutinin, D-amino acids, gliadin (partially digestible), and trypsin inhibitors, among others. (The one component that is digestible is amylopectin A, accounting for the exceptional glycemic potential of wheat and other seeds of grasses, explaining why two slices of whole wheat bread increase blood sugar higher than 6 teaspoons of table sugar.)
You don’t look or smell like a ruminant. Why would you eat like one? When you try to make like a ruminant, all manner of health disasters result from gastrointestinal distress, to autoimmune diseases, to various forms of allergy, to heart disease, to cancer, to dementia. Humans are not adapted to consumption of grasses, seeds or otherwise.
The post The Bovine Guide to Healthy Eating appeared first on Dr. William Davis.
December 17, 2018
Nutritional Lipidology
The statin drug industry and their willing and eager servants, i.e., doctors, have managed to prop up a drug franchise that has reaped hundreds of billion of dollars over the years while providing little benefit but plenty of harm. Although I’ve discussed these issues many times here in the Wheat Belly Blog, the Wheat Belly books, and more recently in the Undoctored book and Blog, it bears exploring further. I keep on hoping that clarity, logic, evidence, truth and repetition overcome our lack of billions of dollars in marketing that Big Pharma controls, a genuine David-vs-Goliath situation.
I call all the varied causes of coronary heart disease and heart attack that are wonderfully correctable using nutrition “Nutritional Lipidology,” the study of the effects of nutrition on lipids, lipoproteins, and metabolic parameters that, if uncorrected, can lead to cardiovascular disease. It is indeed relevant to the Wheat Belly conversation, as wheat elimination and, even better, grain elimination, yields dramatic effects on lipids, lipoproteins, and the factors that drive cardiovascular risk. And there are other natural strategies that further and dramatically improve factors that could have led to heart diseases. In fact, I have found these simple strategies so powerful that most people obtain values that are superior to that achieved with statin drugs and other prescription agents. No, the world does not need more statin drugs; it needs better unbiased health information that does not result in revenues for deep-pocketed drug companies while genuinely reducing cardiovascular risk.
Big Pharma and my colleagues prefer to talk about “cholesterol.” I call cholesterol the kindergarten version of how to understand how cardiovascular disease is caused: there’s a germ of truth to it, but it vastly oversimplifies real causes, is misleading, and can be subverted into the service of those who are adept at bending the truth, AKA pharmaceutical companies and those who fall for their clever marketing, i.e., practicing physicians. This discussion can get awfully hairy very quickly (I tried to tame it in the chapter called “My particles are bigger than yours” in the original Wheat Belly book), so let me try to distill it down. Follow the nutritional principles laid out in Wheat Belly and Undoctored, incorporate a handful of core strategies to correct common nutritional deficiencies, and cultivate and nourish healthy species of bowel flora, and you have a powerful, do-it-yourself-at-home, and marvelously effective way to correct “cholesterol” values and, more importantly, lipoproteins (lipid-carrying proteins) and metabolic factors such as blood sugar and inflammation, the real currency of cardiovascular disease.
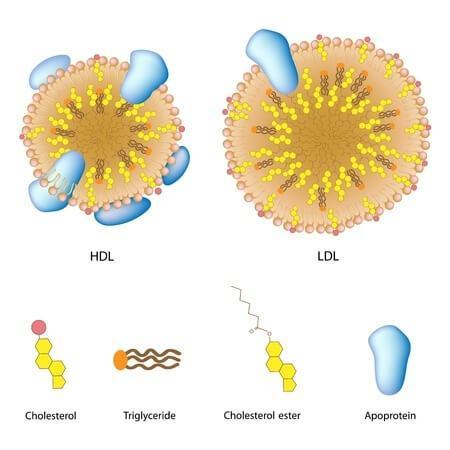
Let’s begin with the overly-simplistic changes that develop on a standard 4-item cholesterol panel. Wheat elimination followed by a handful of simple strategies exert these effects on any cholesterol panel:
HDL cholesterol goes up
Triglycerides drop, often dramatically
LDL cholesterol–remember: a crude calculated value, not a measured value, usually goes down. However, recall that this value is so unreliable that it can do anything, while real measures, such as an actual count of LDL particles (e.g., NMR lipoproteins) goes down.
Total cholesterol–also a confusing issue, because total cholesterol = LDL cholesterol + HDL cholesterol + triglycerides/5. Thus, if HDL goes up–a good thing–total cholesterol also goes up–often interpreted as a bad thing that many doctors mistakenly try to “treat” with statins. Total cholesterol is, in my view, an outdated and totally useless value, useless for application to specific individuals.
While there’s a heck of a lot more to this than my own personal experience, here was my own transformation. When I was vegetarian 25 years ago, eating only “healthy whole grains,” fruits, and vegetables, my values were:
HDL 27 mg/dl
Triglycerides 350 mg/dl
LDL cholesterol 144 mg/dl
Total cholesterol 241 mg/dl
My fasting glucose was 161 mg/dl–I became diabetic on this low-fat, vegetarian program–a metabolic disaster. And I was jogging 3-5 miles a day. (Soon after Mevacor, the first statin cholesterol drug, was approved by the FDA and released, I took it. Within 72 hours, I became acutely ill, thought I was going to die and couldn’t get out of bed for 48 hours. Likewise, Zocor, Lipitor, and Crestor made me sore all over, made me think I had aged 30 years overnight. Needless to say, I stopped playing with them both personally and, over time, learned how to help patients control the situation with almost no reliance on this deeply flawed group of drugs.) I stopped following a vegetarian, grain-based diet over the years, eventually eliminating all grains, eating more fat, correcting my vitamin D deficiency, supplementing omega-3 fatty acids, supplementing iodine and correcting thyroid dysfunction, supplementing magnesium, making efforts to cultivate bowel flora, and my values–on NO drugs–are:
HDL 97 mg/dl
Triglycerides 43 mg/dl
LDL cholesterol 81 mg/dl
Total cholesterol 187 mg/dl
My fasting blood sugar: 84 mg/dl. HbA1c: 4.8%–no more type 2 diabetes, no drugs. If we were to look at the changes in lipoproteins, the real values underlying the crude cholesterol values, we would observe that:
Small LDL particles are gone or dramatically reduced–Because the amylopectin A of grains is the most flagrant trigger for small LDL particles, eliminating wheat and grains results in marked reductions or elimination. The reduction in triglycerides and VLDL achieved with omega-3 fatty acids, coupled with enhanced insulin sensitivity achieved through weight loss, vitamin D, and magnesium add to the effect.
VLDL particles are dramatically reduced–Because there is no amylopectin A to convert (via the liver process of de novo lipogenesis) to triglycerides that fill VLDL particles, the number and composition of VLDL particles are altered and are less able to contribute to unhealthy effects, such as triggering formation of small LDL particles. Omega-3 fatty acids further reduce VLDL particles substantially.
Postprandial lipoproteins, i.e., the after-meal flood of particles into the bloodstream after digestion, are markedly reduced. While fat makes a modest contribution to postprandial lipoproteins, carbohydrates such as amylopectin A make a larger contribution, though delayed for several hours. Eliminate amylopectin A and this effect disappears. Omega-3 fatty acids further blunt the postprandial rise.
The number of LDL particles (e.g., via NMR lipoproteins or apoprotein B, the primary protein of LDL particles), the real measure of LDL particles and not a crude calculated LDL cholesterol value, drops substantially. This develops because of the reduction or elimination of small LDL particles within the total number of LDL particles; the cultivation of Lactobacillus and Bifidobacteria bowel flora species that express the enzyme, bile acid hydrolase, that inhibits resorption of bile acids that would otherwise have been recirculated to create more LDL particles; and correction of thyroid status.
Yes, a bit complicated. But we have to get beyond this ridiculous notion that cutting fat or saturated fat and taking statins reduce “cholesterol.” When you start to understand what really happens with changes in diet, you quickly recognize that, not only is most of the billions of dollars spent annually on statin drugs not necessary, you recognize that astounding improvements in lipids and lipoproteins are achievable by incorporating just a few simple strategies with results dramatically SUPERIOR to that achievable with statins.
The real tragedy of focusing on cholesterol and statin drugs, as you can see, is that it diverts attention away from the factors that really underlie cardiovascular risk, But this is why I say that YOU can do a better job at reducing or eliminating cardiovascular risk than your doctor.
The post Nutritional Lipidology appeared first on Dr. William Davis.
December 15, 2018
Cream of Mushroom Soup with Chives

Here’s a simple oldie-but-goodie belly-warming recipe rom the Wheat Belly 30-Minute Cookbook: Cream of Mushroom Soup with Chives. It’s not just a delicious lunch or dinner side-dish, but can also accompany your holiday meals.
Prep time: 5 minutes Total time: 20 minutes
If dairy avoidance is not an issue for you, the olive oil can be substituted with butter, the coconut milk substituted with cream, half-and-half, or whole milk.
Makes 8 servings
2 tablespoons extra-virgin olive oil
1 medium yellow onion, finely chopped
2 cloves garlic, minced
16 ounces baby bella, cremini, or button mushrooms, chopped coarsely
1 teaspoon sea salt or to taste
1 teaspoon black pepper
3 cups chicken stock
12 ounces coconut milk (preferably thicker canned variety)
2 tablespoons chives, chopped
In large skillet over medium-high heat, heat olive oil. Sauté onions and garlic until onions translucent, then add mushrooms. Reduce heat to medium, add salt and pepper, and cover for several minutes until mushrooms softened.
Stir in chicken stock and coconut milk, cover and simmer for 3-5 minutes.
Ladle or pour mixture into blender and blend until smooth (in batches, if necessary). Serve topped with chopped chives.
The post Cream of Mushroom Soup with Chives appeared first on Dr. William Davis.
December 14, 2018
Don’t toy with glycemic index

Here is a discussion I first posted in my Wheat Belly Total Health book, chapter 7: Grainless Living Day-to-Day.
Glycemic index, or GI, describes how high blood sugar climbs over 90 minutes after consuming a food compared to glucose.
The GI of a chicken drumstick? Zero: No impact on blood sugar. How about three fried eggs? Zero, too. This is true for other meats, oils and fats, seeds, mushrooms, and non-starchy vegetables. You eat any of these foods and blood sugar doesn’t budge, no glycation phenomena follow, no glucotoxic or lipotoxic damage to such things as your pancreas.
There is nothing intrinsically wrong with the concept of GI nor of the related concept, glycemic load, GL, a measure that also factors in the quantity of food. The problem is how the values for GI and GL are interpreted. For instance, categories of GI are arbitrarily broken down into:
High glycemic index: 70 or greater
Moderate glycemic index: 56-69
Low glycemic index: 55 or less
This is like being a little bit more or less pregnant. By this scheme, cornflakes, puffed rice, and pretzels have “high“ GIs above 70, thereby sending your blood sugar through the roof, while whole grain bread, oatmeal, and rice have “low” GIs. A typical non-diabetic person consuming a typical serving of cornflakes, e.g., 1 cup cereal in ½ cup milk, will thereby experience a blood sugar in the neighborhood of 180 mg/dl—very high and more than sufficient to set the process of glycation and glucotoxicity on fire, add to adrenal disruption, cataract formation, destruction of cartilage, hypertension, heart disease, and neurological deterioration or dementia. (Blood sugars will vary, of course, depending on body weight, degree of overweight, insulin sensitivity, time of day, and other factors, but this would be typical. Someone with pre-diabetes or diabetes will have a higher blood sugar.)
How about a low-glycemic index food, such as a bowl of oatmeal, 1 cup cooked, in ½ cup milk? A typical response: blood sugar 170 mg/dl—lower, yes, but still quite awful, triggering all the same undesirable phenomena triggered by the high-glycemic cornflakes. This is why I believe “low” GI is more accurately labeled “less-high” GI, not “low.” Alternatively, we could just recognize that any GI above single digits should be regarded as high because it’s not until you get to single digits or zero that blood sugars no longer range into destructive levels.
The concept of “glycemic load” tries to take this into account by factoring in portion size. Thus the GL of cornflakes is 23, while the GL of oatmeal is 13 and that of whole wheat bread is 10. GL is usually interpreted as:
High glycemic load: 20 or greater
Moderate glycemic load: 11-19
Low glycemic load: 10 or less
Once again, this lulls you into thinking that foods like oatmeal or whole wheat bread don’t raise blood sugar—but they do. They are not low glycemic load; they have less high glycemic loads.
The value that truly appears to count and predict whether or not we will have a blood sugar rise? Grams of carbohydrate. Specifically, “net” grams of carbohydrate calculated by subtracting fiber:
“Net” carbohydrates = total carbohydrates – fiber
Net carbohydrates is a concept popularized by the late Dr. Robert Atkins, who recognized that fiber has no impact on blood sugar despite being lumped together with other carbohydrates. (Fiber is technically a carbohydrate, or polysaccharide, but humans lack the enzymes to digest fibers into sugars.) In other words, there is really no need for manipulations such as glycemic index or glycemic load and their misleading classifications.
If you were to test blood sugars with a common fingerstick glucose meter (as many of us, diabetic and non-diabetic, often do to gauge the effect of different foods) 30-60 minutes after consuming a food, you would see that it takes most of us around 15 grams of net carbohydrates before we begin to see a rise above the starting value. We check blood sugars at 30-60 minutes after consuming a food. The peak can actually occur before or after 30-60 minutes, depending on the mix of protein, fat, fiber, the amount of water or other liquids, pH of the food, and other factors. This is just an approximation of peak blood sugar that allows you to perform a single fingerstick, rather than every few minutes. What we don’t do is check blood sugar two hours after consumption, as advised by most physicians interested in blood sugar control on insulin and other diabetes medications. This seems obvious, but is a common tripping point when discussed with doctors.
Ideally, allow little to no rise in blood sugar. In this way, you have turned off any excess levels of glycation and glucotoxicity, undo the effects of high insulin and insulin resistance, and allow fasting blood sugars to head downward over time, while also accelerating weight loss.
There is another common fiction—or perhaps half-truth might be a better term—prevailing in nutritional thinking offered by the dietary community that tells us that, if a high-glycemic index food is consumed along with proteins, fats, or fiber, i.e., foods with low- or zero- glycemic index, that the net glycemic effect will be much improved. For this reason, dietitians often advise people to consume, say, bread with peanut butter: the high blood sugar potential of the bread is blunted by the low-glycemic protein, fat, and fiber of the peanut butter. As often occurs in the flawed logic of nutrition, this is another example of something being less bad, not necessarily good. For instance, a typical blood sugar in a middle-aged mildly overweight male after consuming two slices of multigrain bread made with whole wheat flour, oats, and millet on an empty stomach might be 170 mg/dl—high enough to provoke insulin, cortisol, insulin resistance, visceral fat accumulation, inflammation, glycation and glucotoxicity, and add to dementia risk. In another session, again starting with an empty stomach, the same male consumes two slices of multigrain bread, but this time with several slices of turkey (mostly protein), mayonnaise (mostly fat), and lettuce (mostly fiber and water). Blood sugar: 160 mg/dl—better, yes, but still pretty awful and more than sufficient to generate all the phenomena generated at a blood sugar of 170 mg/dl, including brain atrophy.
Less bad is not necessarily good. Feel free to count your carbs, but ignore the misleading concepts of glycemic index and glycemic load. Use those tables of glycemic index you might have to line your box of cat litter, but don’t use them to construct a healthy diet.
The post Don’t toy with glycemic index appeared first on Dr. William Davis.
Dr. Davis Infinite Health Blog

Recognize that this i ...more
- William Davis's profile
- 159 followers

