
Mark Sisson's Blog, page 372
September 3, 2012
Dear Mark: Why Do We Procrastinate and How Do We Beat It?
 Do you procrastinate? If you’re an actual human being – not a replicant, nor an android, nor an AI – and you’re being honest, then you should probably be nodding your head. But what’s odd about a ubiquitous behavior like procrastination is that it’s almost unanimously regarded as being detrimental to our success, our happiness, and our progress as human beings, and yet we still put things off until later. Counterintuitive yet persistent behaviors fascinate me to no end, because they suggest (at least to me) an evolutionary incongruence at hand. They suggest that in another context, another environment, the counterintuitive was anything but.
Do you procrastinate? If you’re an actual human being – not a replicant, nor an android, nor an AI – and you’re being honest, then you should probably be nodding your head. But what’s odd about a ubiquitous behavior like procrastination is that it’s almost unanimously regarded as being detrimental to our success, our happiness, and our progress as human beings, and yet we still put things off until later. Counterintuitive yet persistent behaviors fascinate me to no end, because they suggest (at least to me) an evolutionary incongruence at hand. They suggest that in another context, another environment, the counterintuitive was anything but.
Is procrastination just such a behavior? Let’s explore:
Dear Mark,
I have noticed that procrastination is a huge problem for many of my friends and colleagues. I know that I too will make myself miserable by putting a project off until the very last minute, yet even though I recognize the misery and it’s very avoidable cause, I continue to do it anyway.
Do you think there is a primal solution to this issue? Why do you think we feel the need to put off our to do lists? I cannot imagine that this attitude would have served our ancestors well. Why is it such a struggle for so many people?
I have read up on this topic a bit. There are different theories, but two of the most prevalent are the theory that procrastination is due to perfectionism and the theory that procrastination is caused by impulsivity. I would love to get your perspective on this issue and how rampant procrastination might be caused by a misalignment of our modern world with our primal selves.
Thank you!
Sarah
As you mention, there are competing ideas about the cause of procrastination.
The “procrastination as perfectionism” idea says that procrastinators are actually perfectionists who are paralyzed with fear at failing to do things absolutely perfectly. They continue to put things off to avoid the chance of doing something less than perfectly. On its face, this seems limited. Sure, you could argue that the English student with an essay to write procrastinates because she can’t come up with a good, defensible thesis, but what about the guy who waits til the last minute to do his taxes or pay the water bill? How does perfectionism enter into those situations?
A 2007 meta-analysis concluded that perfectionism was likely not at the heart of procrastination (PDF). In fact, perfectionists are actually slightly less likely to be procrastinators. It’s just that perfectionists who are procrastinators were more likely to seek professional help (because, being perfectionists, they wanted to beat procrastination), and this created a self-selection phenomenon in which clinicians would report a preponderance of procrastinating perfectionists and thus skew their perception. They’re not seeing all the procrastinators who aren’t perfectionists, because, well, “I’ll just make the appointment another day.”
Piers Steel (author of that meta-analysis and bearer of a romance novel protagonist name) thinks that we procrastinate partly because the task at hand simply isn’t pleasant to do and partly because we’re not confident in our abilities to perform it – common sense factors that, I think, we can all agree on. If something is boring and hard to do, we’re less likely to do it right away and more likely to wait until the last minute. Makes sense, right? But at the “nickel-iron” core of procrastination, says Steel, lies impulsivity. We don’t like waiting for rewards, and, according to Steel’s research, we’re even inclined to take the lesser reward (say, $1000) instead of the greater reward (say, $2000) if the former is available immediately and the latter is available only a year from now.
As far as procrastination being yet another manifestation of the modern world’s misalignment with our Primal selves? I think there’s something to it. Consider the possibility that daily life in the millenia past was more “check to check” (without the checks, of course). Most tasks we had to complete literally could not wait – gathering the day’s water (or else have none), building or finding shelter (or else be exposed to the elements) . These were tasks that, upon completion, provided immediate, tangible rewards. I think we’re built for these short-range tasks with immediate rewards, but we live in a society of lists and goals and projections and commitments and schedules which don’t always offer noticeable rewards upon completion.
I’m of the mind that many of the things we’re “supposed to do” are alien concepts to our ancient brains. What is paying bills, really? You scribble some stuff on a slip of paper (or go online and clack on some keys) that represents a portion of your hard earned money and send it off to some faceless entity? We understand why we need to pay the water bill, but do we really get it? Nothing happens when we pay it. Nothing really changes. If we hadn’t done it that day, the water would still flow, probably for at least a month. Or how about waking up early and trudging into the office to shuffle some papers for eight hours? Many of us are so disconnected from the bigger picture at our jobs, and work for such large companies, that the immediate effect of the work we do is tough to judge. And thus, to our Primal mind’s eye, the work is meaningless and unfulfilling. Perhaps this accounts for some of the burnout seen in the corporate world.
What are the hardest tasks to put off? The ones that choose you, that pop up without much warning, the ones to which you must react and respond immediately. The easiest? The far-off decisions, the “safely at a distance” ones that sound good and necessary and completely rational from afar, until the day actually approaches and you realize you’re going to have to do the thing – and then you don’t do it, or agonize for hours and days before doing it. On one extreme, it’s a falling tree branch headed straight for your head – you don’t procrastinate about moving your head out of the branch’s path. On the other extreme, it’s deciding to go hunting when you’ve just nabbed a 600-pound elk cow the day before. The muscle meat is sliced and hung to dry over the smoke pits, the bones and trimmings are being processed into grease, and you’re eating last night’s organ-stuffed intestines for breakfast. Your people have enough meat for at least a week or two, but another kill would keep you stocked for perhaps a month. You could head out and spend the day trying to nab another animal and be set for awhile if you succeed, or you could chill out by the fire, sip some fermented honey, and enjoy what you have.
What can you do, though, when you live in a world of deadlines and commitments, schedules and calendars?
Victor Hugo would strip off his clothes, give them to his butler, and have him hide them until he finished writing. That way, he’d be stuck indoors with no other option but to write. A Primal solution might be to take the tasks that you find yourself putting off and break them up into smaller, manageable chunks with deadlines, more akin to what our ancestors would have dealt with. I briefly detailed the Seinfeld method of productivity in this post, which involves making a calendar for each task with goals and deadlines on each day; take a look and see what you think. Think of it as tricking your brain into thinking a large, sprawling task is several small ones with immediate rewards.
Another option is to set things up so that you are penalized for not doing a task. Try one of the productivity tools mentioned above, or just give a friend a hundred bucks and tell him not to give it back unless you write the paper. Grok often completed tasks because his life and livelihood literally depended on their completion; you’re probably gonna stick around regardless of your procrastination, so give your mind something tangible (not) to look forward to. Create a meaningful penalty for yourself so that your Primal brain notices and “fears” it enough to get you to do it.
In related news, the Primal Blueprint 21-Day Challenge is coming next week, so if you’re a chronic procrastinator in regards to health, fitness, or you’re just lagging on going Primal in general, stay tuned for the antidote: tangible rewards! Thanks for reading, guys, and be sure to leave a comment about your experience with procrastination.
Grab a Copy of The Primal Blueprint 21-Day Total Body Transformation and Start Getting Primal Today!



September 2, 2012
Weekend Link Love
 Research of the Week
Research of the WeekCaloric restriction has been shown to increase longevity in worms, fruit flies, and certain strains of mice, but new research shows that this is not the case for rhesus monkeys. Here’s the link to the study.
Everyone’s always known that babies are incredibly nutritious, but they take too long to grow (plus, it’s illegal). A recent study shows that microgreens – young tender week-old baby greens from spinach, pea, beet, and purple mustard (just to name the specific greens in the study) – contain more vitamins and phytonutrients than their adult versions. Plus, they’re easy and quick to grow at home.
People who engaged in moderate aerobic exercise – walking and slow jogging (at a 10 or 11 minute mile pace) – lived longer than people who engaged in intense endurance exercise and people who engaged in none at all.
Interesting Blog Posts
Frank Forencich wrote a highly opinionated opinion piece about the sometimes bitterly opposed opinions we hold on health and nutrition. What do you think?
Nom Nom Paleo just finished a 5-part series on packing healthy lunches for kids that kids will actually eat. If you want your kids to hold a strong bartering chip (that’s not actually a chip) in the lunchtime economy, check out the series, starting with part 1.
Media, Schmedia
This is the beginning of the end: CrossFit got mentioned on TMZ.
Jimmy Moore reveals that his reader poll reveals that, for whatever reason, his readership considers me to be a pretty trustworthy source of information. Thanks, Jimmy and readers!
Everything Else
Recipe Corner
Since stone fruit season is winding down and I’m a sucker for a good nectarine, I’ve been incorporating them into my Big Ass Salads as of late. Here’s a good example.
A few years ago, I told you of the wonders of the mackerel. Here’s a nice way to cook it (plus, how to pickle jalapeño peppers).
Time Capsule
One year ago (September 2 – September 8)
Urban Hiking: Exploring Your Local Terrain – Like it or not, our modern urban habitats are here to stay, and there’s no need to save your hiking solely for the wilderness.
GERD: Symptoms, Causes and Remedies – How to beat heartburn.
Comment of the Week
Two of us, the two I think were most enthusiastic about climbing the tree up to a platform someone had built, discussed as we were climbing how we felt like the tree was helping us climb and that we felt connected to its spirit and through it, the living earth below. We ended up hugging the tree on the platform. Climbing down I did some *slightly* risky maneuvers that probably required a lot of energy but it felt practically effortless and very smooth like the tree was controlling me and all I had to do was go with its flow. And I was bare foot for all this, which added to the experience. It definitely made me feel more grounded.
- Now that’s how you cultivate intermittent euphoria, Animanarchy.
Grab The Primal Blueprint Cookbook Today and Receive Free S&H and a Free Primal Blueprint Poster

September 1, 2012
Shakshuka (Eggs Poached in Spicy Tomato Sauce)
 Whether you’re looking for a new breakfast idea or are fond of serving breakfast for dinner, shakshuka fits the bill. Instead of calling the dish shakshuka you can also just call it “Eggs Poached in Spicy Tomato Sauce” because that’s exactly what this straightforward but surprisingly delicious meal is.
Whether you’re looking for a new breakfast idea or are fond of serving breakfast for dinner, shakshuka fits the bill. Instead of calling the dish shakshuka you can also just call it “Eggs Poached in Spicy Tomato Sauce” because that’s exactly what this straightforward but surprisingly delicious meal is.
Especially popular in Israel, shakshuka is loved around the world for its comforting flavor and simple preparation. Although the sauce is often sopped up with pita bread, it’s thick enough that you can skip the bread and eat it with a spoon (or spread extra sauce over a hunk of grilled meat for a really fantastic meal.)
Most recipes for shakshuka call for canned (or boxed) tomatoes, but you shouldn’t hesitate to use plump, super-ripe fresh tomatoes if you can find them. Tomatoes are the main ingredient in shakshuka and some say that little else, besides eggs and garlic, should be added. However, this version leans in the direction of spicing things up with more flavor and variety. Onion, bell pepper, jalapeno, cumin and paprika make the meal more than just a pot of simmered tomatoes.
The eggs are added at the end and then cooked until just set. The contrasting flavors and textures in your bowl – creamy, soft eggs swimming in thick, spicy sauce – is what shakshuka is all about.
Servings: 4
Ingredients:

1/4 cup olive oil
1 to 3 jalapeno peppers, (depending on how spicy you like it) seeded and finely chopped
1 green bell pepper, cut into thin strips
1 white or yellow onion, finely chopped
4 cloves of garlic, finely chopped
1/2 teaspoon ground cumin
2 teaspoons paprika
28-ounces whole peeled tomatoes in their juice or 2 pounds fresh tomatoes, chopped
4 to 6 eggs
1/4 cup roughly chopped parsley
Optional: crumbled feta cheese
Salt to taste
Instructions:
Preheat the oven to 400 degrees Fahrenheit.
Heat olive oil over medium-high heat in a deep skillet. Add peppers and onion and sauté until onion is lightly browned, about five minutes.

Add garlic, cumin and paprika and sauté one minute more.

Add tomatoes. Break them apart with a large spoon or spatula as they cook. Reduce heat slightly and simmer 15-20 minutes (longer if tomatoes are fresh), stirring occasionally, until sauce has thickened and most of the liquid is gone. Add salt to taste.

Crack the eggs evenly around the skillet. Place the skillet in the oven and cook until the egg whites are set, 6-8 minutes.

Garnish with parsley (and feta). Serve warm.

Grab The Primal Blueprint Cookbook Today and Receive Free S&H and a Free Primal Blueprint Poster

August 31, 2012
The Perfect Storm (a.k.a. How I Lost Those Last 10 lbs)
It’s Friday, everyone! And that means another Primal Blueprint Real Life Story from a Mark’s Daily Apple reader. If you have your own success story and would like to share it with me and the Mark’s Daily Apple community please contact me here. I’ll continue to publish these each Friday as long as they keep coming in. Thank you for reading!
 Female, age 45, 5’ 2”
Female, age 45, 5’ 2”
Starting weight: Flirting with 130 lbs
Goal weight: 120 lbs
Current weight: 117 lbs
I’ve always eaten a fairly “healthy” diet (according to the latest conventional wisdom) and exercised regularly (cycling, hiking and BodyPump™twice a week), but as the years were going by my weight was creeping up. I was still at the high range of “normal”, but I was puffy and didn’t feel like my efforts with BodyPump™ were showing.


In April 2011 I stumbled upon Mark’s Daily Apple. It just clicked for me. I adopted the Primal way of eating immediately and had no trouble giving up grains and sticking to the 80/20 rule. In 2 months I had lost 5 lbs without even “trying”. My husband was skeptical.
In June 2011 my husband was diagnosed with Leukemia. He was in the hospital for 6 months. I stopped working and was by his side the entire time. This would have been an easy time to abandon the Primal lifestyle, but it was just what I needed. A little project to keep my mind busy. I read everything I could…books and online about Primal/paleo. My food choices were limited at the hospital cafeteria…hard-boiled eggs and bacon for breakfast was easy. For lunches and suppers I usually walked to a grocery store to hunt and gather. It gave me a purpose and reason to get out of the hospital, move slowly and clear my mind. Despite the stress of the situation the Primal Blueprint kept me sane and healthy. I continued to lean out and people started worrying that I wasn’t eating. I told them I was eating more than usual, but they didn’t believe me. My staples included avocados, mini cukes, cherry tomatoes, berries, tinned sardines and salmon, nuts, full-fat cheese, smoked chicken thighs, liver pate, coconut water, coffee with heavy cream, dark chocolate and plenty more! My occasional treat…good quality vanilla ice cream (and it’s still my weakness).


My husband had a stem cell transplant in November 2011. I’m thrilled to report that he has completely recovered from his illness. He’s back to work and we’re cycling again. Although he thinks I’m a little extreme on following “the cult”, he’s totally supportive. He’s even started to adopt some of the Primal ways (although it will be a while before he gives up his muesli for breakfast before work and his sandwich at lunch). Between us we have 3 “normal weight” teenagers. I feed them healthy meals at supper time, but for the rest of the day they make their own choices…often not very smart ones. As they get older I hope they become more aware of the connection between their diet and their health. In the meantime, I love it when they ask me, “Is this Primal?”
Stephanie Turner
Grab The Primal Blueprint Cookbook Today and Receive Free S&H and a Free Primal Blueprint Poster

August 30, 2012
The Straight Dope on Cholesterol: 10 Things You Need to Know – Part 2
 This is a guest post by Peter Attia and is a summary based on a 10-part series of the same name that you can find at The Eating Academy.
This is a guest post by Peter Attia and is a summary based on a 10-part series of the same name that you can find at The Eating Academy.
To read The Straight Dope on Cholesterol: 10 Things You Need to Know – Part 1 click here.
To start at the beginning of Peter’s 10-part series click here.
Now, Peter…
6. Inflammation makes it worse, but the inciting event is the LDL particle getting past the endothelium.
Because there is no experiment or clinical trial we can carry out to unambiguously resolve the exact role of inflammation in this process (and, by extension, the role of LDL particles), we rely on so-called “natural experiments.”
Such “natural experiments,” which help elucidate this role, are those of people with genetic alterations leading to elevated or reduced LDL-P. Let’s consider an example of each:
Cohen, et al. reported in the New England Journal of Medicine in 2006 on the cases of patients with mutations in an enzyme called proprotein convertase subtilisin type 9 or PCSK9. Normally, this proteolytic enzyme degrades LDL receptors on the liver. Patients with mutations (“nonsense mutations” to be technically correct, meaning the enzyme is somewhat less active) have less destruction of hepatic LDL receptors. Hence, they have more sustained expression of hepatic LDL receptors, improved LDL clearance from plasma, and therefore fewer LDL particles. These patients have very low LDL-P and LDL-C concentrations (5-40 mg/dL) and very low incidence of heart disease. Note that a reduction in PCSK9 activity plays no role in reducing inflammation.
Conversely, patients with familial hypercholesterolemia (known as FH) have the opposite problem. While there are several variants and causes of this disease, the common theme is having decreased clearance of apoB-containing particles, often but not always due to defective or absent LDL receptors, leading to the opposite problem from above. Namely, these patients have a higher number of circulating LDL particles, and as a result a much higher incidence of atherosclerosis.
So why does having an LDL-P of 2,000 nmol/L (95th percentile) increase the risk of atherosclerosis relative to, say, 1,000 nmol/L (20th percentile)? In the end, it’s a probabilistic game. The more particles – NOT cholesterol molecules within the particles - you have, the more likely the chance a LDL-P is going to ding an endothelial cell, squeeze into the sub-endothelial space, and begin the process of atherosclerosis.
7. LDL particles (LDL-P), not LDL cholesterol content (LDL-C), is what drives sterols into artery walls – Don’t confuse the “boats” and the “cargo.”
There are several examples of long-term studies examining the predictive power of LDL-C versus LDL-P with respect to cardiovascular disease. This study followed a Framingham offspring cohort of about 2,500 patients over a median time period of almost 15 years in each of the four possible groups (i.e., high-high, high-low, low-high, and low-low) and tracked event-free survival. In this analysis the cut-off points for LDL-P and LDL-C were the median population values of 1,414 nmol/L and131 mg/dL, respectively. So, “high” implies above these values; “low” implies below these values. Kaplan-Meier survival curves are displayed over a 16 year period – the steeper the slope of the line the worse the outcome (survival).
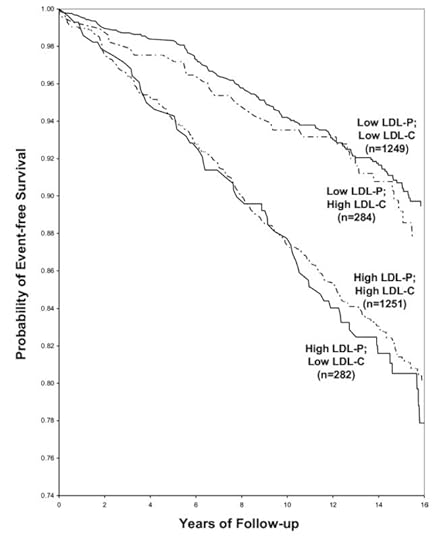
The same patterns observed in the other studies are observed here:
High LDL-P is the best predictor of adverse cardiac events.
LDL-C is only a good predictor of adverse cardiac events when it is concordant with LDL-P; otherwise it is a poor predictor of risk.
Interestingly the persons with the worst survival had low (below median) LDL-C but high LDL-P. The patients most likely to have high LDL-P with unremarkable or low LDL-C are those with either small LDL particles, or TG-rich/cholesterol poor LDL particles, or both (e.g., insulin resistant patients, metabolic syndrome patients, T2DM patients). This explains why small LDL particles, while no more atherogenic on a per particle basis than large particles (see point #9), are often a marker for something sinister.
8. People with metabolic syndrome are at even greater risk of LDL-C/LDL-P discordance.
Concordance is a statistical term that refers to variables that predict the same thing. Conversely, discordance refers to variables that do not predict the same thing. When LDL-C (what most doctors measure in your blood test) and LDL-P (what most doctors do not measure in your blood test) predict the same risk, they are said to be concordant. When they do not, they are said to be discordant. In the latter case, LDL-P is the one to follow.
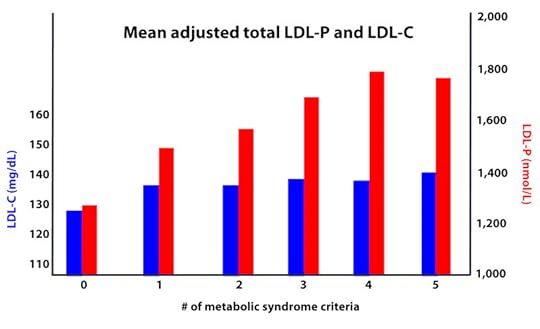
To illustrate the prevalence of discordance between LDL-C and LDL-P, consider the figure below.
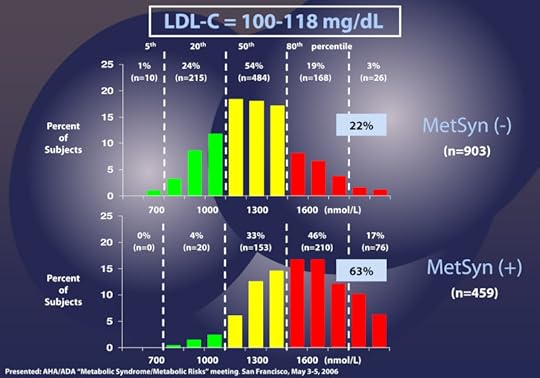
This figure shows data from patients with LDL-C between 100 and 118 mg/dL (i.e., second quartile of risk: 25th to 50th percentile) without metabolic syndrome (top) and with metabolic syndrome (bottom). In the patients without metabolic syndrome, LDL-C under-predicts cardiac risk 22% of the time. However, when you look at the patients with metabolic syndrome, you can see that 63% of the time their risk of cardiac disease is under-predicted.
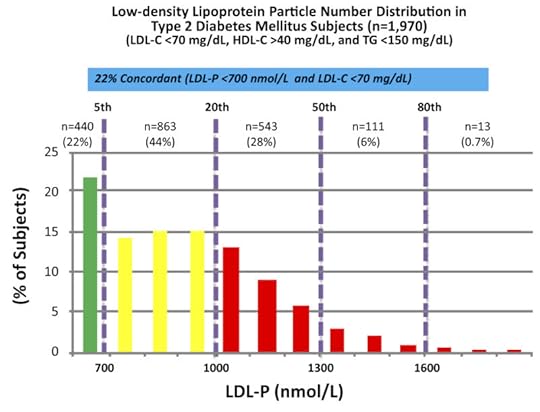
The data above were collected from nearly 2,000 patients with diabetes who presented with “perfect” standard cholesterol numbers: LDL-C < 70 mg/dL; HDL-C > 40 mg/dL; TG <150 mg/dL. However, only in 22% of cases were their LDL-P concordant with LDL-C. That is, in only 22% of cases did these patients have an LDL-P level below 700 nmol/L.
Remember, LDL-C < 70 mg/dL is considered VERY low risk – the 5th percentile. Yet, by LDL-P, the real marker of risk, 35% of these patients had more than 1,000 nmol/L and 7% were high risk. When you do this analysis with the same group of patients stratified by less stringent LDL-C criteria (e.g., <100 mg/dL), the number of patients in the high risk group is even higher.
As a general rule, the more “metabolically deranged” an individual is, the greater this discordance between LDL-C and LDL-P, as shown in the figure below. The axis of this figure is adjusted so that the red bars and the blue bars should be of the same height when LDL-C and LDL-P are concordant.
9. A smaller LDL particle is no more or less atherogenic than a large one – a particle is a particle.
Particle size is something many folks fixate on, and there is no doubt that smaller LDL particles are associated with greater risk. But, on a particle-by-particle basis are they, in fact, more atherogenic? Let’s find out.
This figure (one of the most famous in this debate) is from the Quebec Cardiovascular Study, published in 1997, in Circulation. You can find this study here.

This is kind of a complex graph if you’re not used to looking at these. It shows relative risk – but in 2 dimensions. It’s looking at the role of LDL size and apoB (a proxy for LDL-P). What seems clear is that in patients with low LDL-P (i.e., apoB < 120 mg/dl), size does not matter. The relative risk is 1.0 in both cases, regardless of peak LDL size. However, in patients with lots of LDL particles (i.e., apoB > 120 mg/dl), smaller peak LDL size seems to carry a much greater risk – 6.2X.
If you just looked at this figure, you might end up drawing the conclusion that both size and number are independently predictive of risk. Not an illogical conclusion…
What is not often mentioned, however, is what is in the text of the article:
“Among lipid, lipoprotein,and apolipoprotein variables, apo B [LDL-P] came out as the best and only significant predictor of ischemic heart disease (IHD) risk in multivariate stepwiselogistic analyses (P=.002).”
“LDL-PPD [peak LDL particle diameter] – as a continuous variable did not contribute to the risk of IHD after the contribution of apo B levels to IHD risk had been considered.”
What’s a continuous variable? Something like height or weight, where the possible values are infinite between a range. Contrast this with discrete variables like “tall” or “short,” where there are only two categories. For example, if I define “tall” as greater than 6 feet, the entire population of the world could be placed in two buckets: Those who are “short” (i.e., less than 6 feet tall) and those who are “tall” (i.e., those who are 6 feet tall and taller). This figure shows LDL size like it’s a discrete variable – “large” or “small” – but obviously it is not. It’s continuous, meaning it can take on any value, not just “large” or “small.” When this same analysis is done using LDL size as the continuous variable it is, the influence of size goes away, and only apoB (i.e., LDL-P) matters.
This effect has been observed subsequently, including the famous Multi-Ethnic Study of Atherosclerosis (MESA) trial, which you can read here. The MESA trial looked at the association between LDL-P, LDL-C, LDL size, IMT (intima-media thickness – the best non-invasive marker we have for atherosclerosis), and many other parameters in about 5,500 men and women over a several year period.
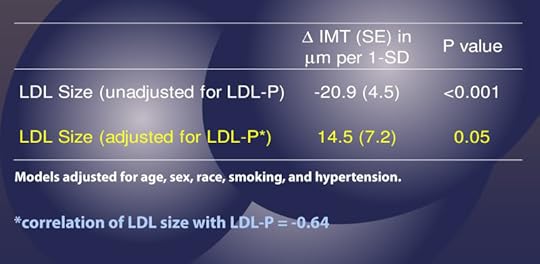
This study used the same sort of statistical analysis as the study above to parse out the real role of LDL-P versus particle size, as summarized in the table above.
This table shows us that when LDL-P is NOT taken into account (i.e., “unadjusted” analysis), an increase of one standard deviation in particle size is associated with 20.9 microns of LESS atherosclerosis, what one might expect if one believes particle size matters. Bigger particles…less atherosclerosis.
However, and this is the important part, when the authors adjusted for the number of LDL particles (in yellow), the same phenomenon was not observed. Now an increase in LDL particle size by 1 standard deviation was associated with an ADDITIONAL 14.5 microns of atherosclerosis, albeit of barely any significance (p=0.05).
Let me repeat this point: Once you account for LDL-P, the relationship of atherosclerosis to particle size is abolished (and may even trend towards moving in the “wrong” direction – i.e., bigger particles…more atherosclerosis).
10. The greatest way to reduce your risk of atherosclerosis is to make sure your boats are carrying the right cargo – that way you’ll need fewer of them.
LDL particles traffic not only cholesterol ester but also triglycerides. Each and every LDL particle has a variable number of cholesterol molecules which, because of constant particle remodeling, is constantly changing. In other words, of the several quadrillion LDL particles floating in your plasma, no two are carrying the exact same number of cholesterol molecules. It takes many more cholesterol-depleted LDL particles than cholesterol-rich LDL particles to traffic a given cholesterol mass (i.e., number of cholesterol molecules) per volume of plasma (i.e., per dL). Core cholesterol mass is related to both LDL particle size (the volume of a sphere is a third power of the radius – it can take 40-70% more small particles than large LDL particles to traffic a given cholesterol mass) and the number of TG molecules per LDL particle.
TG molecules are larger than cholesterol ester molecules, so as the number of TG molecules per particle increases, the number of cholesterol molecules will be less – in a very non-linear manner. Regardless of size, it takes many more TG-rich LDL particles (which are necessarily cholesterol-depleted) to traffic a given cholesterol mass than TG-poor LDL particles. The persons with the highest LDL particles typically (though not always) have small LDL particles that are TG-rich. These are incredibly cholesterol-depleted LDL particles.
Let’s start with what we know, then fill in the connections, with the goal of creating an eating strategy for those most interested in delaying the onset of cardiovascular disease.
There are several short-term studies that have carefully examined the impact of sugar, specifically, on cardiovascular risk markers. Let’s examine one of them closely. In 2011 Peter Havel and colleagues published a study titled Consumption of fructose and HFCS increases postprandial triglycerides, LDL-C, and apoB in young men and women. If you don’t have access to this journal, you can read the study here in pre-publication form. This was a randomized trial with 3 parallel arms (no cross-over). The 3 groups consumed an isocaloric diet (to individual baseline characteristics) consisting of 55% carbohydrate, 15% protein, and 30% fat. The difference between the 3 groups was in the form of their carbohydrates.
Group 1: received 25% of their total energy in the form of glucose
Group 2: received 25% of their total energy in the form of fructose
Group 3: received 25% of their total energy in the form of high fructose corn syrup (55% fructose, 45% glucose)
The intervention was relatively short, consisting of both an inpatient and outpatient period, and is described in the methodology section.
Keep in mind, 25% of total energy in the form of sugar is not as extreme as you might think. For a person consuming 2,400 kcal/day this amounts to about 120 pounds/year of sugar, which is slightly below the average annual sugar consumption in the United States. In that sense, the subjects in Group 3 can be viewed as the “control” for the U.S. population, and Group 1 can be viewed as an intervention group for what happens when you do nothing more in your diet than remove sugar, (which was the first dietary intervention I made in 2009).
Despite the short duration of this study and the relatively small number of subjects (16 per group), the differences brought on by the interventions were significant. The figure below shows the changes in serum triglycerides via 3 different ways of measuring them. Figure A shows the difference in 24-hour total levels (i.e., the area under the curve for serial measurements – hey, there’s our integral function again!). Figure B shows late evening (post-prandial) differences. Figure C shows the overall change in fasting triglyceride level from baseline (where sugar intake was limited for 2 weeks and carbohydrate consumption consisted only of complex carbohydrates).
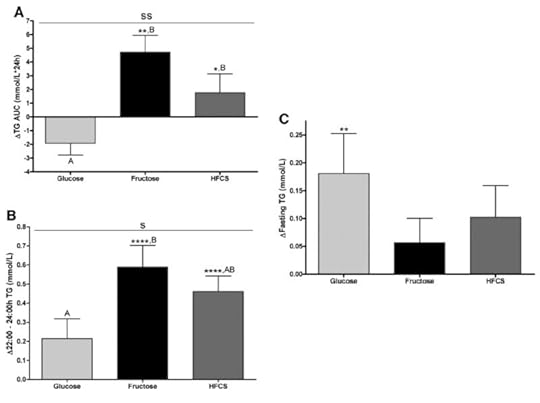
The differences were striking. The group that had all fructose and HFCS removed from their diet, despite still ingesting 55% of their total intake in the form of non-sugar carbohydrates, experienced a decline in total TG (Figure A, which represents the daily integral of plasma TG levels, or AUC). However, that same group experienced the greatest increase in fasting TG levels (Figure C). Post-prandial TG levels were elevated in all groups, but significantly higher in the fructose and HFCS groups (Figure B). The question this begs, of course, is which of these measurements is most predictive of risk?
Historically, fasting levels of TG are used as the basis of risk profiling (Figure C), and according to this metric glucose consumption appears even worse than fructose or HFCS. However, recent evidence suggests that post-prandial levels of TG (Figure B) are a more accurate way to assess atherosclerotic risk, as seen here, here, and here.
The figure below summarizes the differences in LDL-C, non-HDL-C, apoB, and apoB/apoA-I (remember, apoB and apoA-I are good surrogates for LDL-P and HDL-P, respectively).

Again, the results were unmistakable with respect to the impact of fructose and HFCS on lipoproteins, and by extension the relative lack of harm brought on by glucose in isolation. [Removal of glucose and fructose/HFCS would have been a very interesting control group.]
In just a short period of time these dietary interventions had a profound impact on the markers of cardiovascular risk.
So, there you have it – everything you need to know about cholesterol in the length of time it takes to go to the grocery store, buy some high-cholesterol bacon and eggs, cook it, eat it, and savor it. Now it’s your turn to be the judge. Is the conventional wisdom about cholesterol being bad really true?
Visit The Eating Academy for Customized Eating Solutions Based on Real Science

August 29, 2012
The Straight Dope on Cholesterol: 10 Things You Need to Know – Part 1
This is a guest post by Peter Attia and is a summary based on a 10-part series of the same name that you can find at The Eating Academy.
To put this summary post and, more importantly, this 10-part series in perspective, let’s examine one of the most pervasive pieces of dietary advice given to people worldwide:
“Eating foods that contain any cholesterol above 0 mg is unhealthy.”
- T. Colin Campbell, PhD, author of The China Study.
No summary of this length can begin to fully address a topic as comprehensive as cholesterol metabolism and the pathogenesis of atherosclerosis. In fact, those of us who challenge conventional wisdom often find ourselves needing to do exactly what Frederic Bastiat suggested:
“We must admit that our opponents in this argument have a marked advantage over us. They need only a few words to set forth a half-truth; whereas, in order to show that it is a half-truth, we have to resort to long and arid dissertations.”
So, at the risk of trying to minimize the “long and arid” part of this process, below are the 10 things you need to know to be the judge – for yourself – if the conventional advice about cholesterol is correct.
1. The sine qua non of atherosclerosis is the presence of a sterol in an artery wall. How it gets there is the only thing we should be worrying about.
Contrary to popular belief, atherosclerosis is not caused by many of things we think of, such as smoking, high blood pressure, diabetes, high LDL (the so-called “bad” cholesterol), or low HDL (the so-called “good” cholesterol). Some of these are certainly markers of risk – low HDL, for example – while others accelerate the process – smoking, for example – but none of these are the direct cause of atherosclerosis.
The sine qua non of atherosclerosis is the presence of sterols (cholesterol or phytosterol) in arterial wall macrophages. Sterols are delivered to the arterial wall by the penetration of the endothelium by an apoB-containing lipoprotein, which transport the sterols. In other words, unless an apoB-containing lipoprotein particle violates the border created by an endothelium cell and the layer it protects, the media layer, there is no way atherogenesis occurs. If this is a bit confusing, don’t worry. It’s all made clear below.
2. Cholesterol is vital for life; no cholesterol = no life.
Cholesterol is a 27-carbon molecule shown in the figure below. Each line in this figure represents a bond between two carbon atoms. That’s it. Mystery over.
All this talk about “cholesterol” and most people don’t actually know what it is. So, there you have it. Cholesterol is “just” another organic molecule in our body.
I need to make one distinction that will be very important later. Cholesterol, a steroid alcohol, can be “free” or “unesterified” (“UC” as we say, which stands for unesterified cholesterol) which is its active form, or it can exist in its “esterified” or storage form which we call a cholesterol ester (“CE”). The diagram below shows a free (i.e., UC) molecule of cholesterol. An esterified variant (i.e., CE) would have an “attachment” where the arrow is pointing to the hydroxyl group on carbon #3, aptly named the “esterification site.”

One of the biggest misconceptions is that cholesterol is “bad.” This could not be further from the truth. Cholesterol is very good! In fact, there are (fortunately rare) genetic disorders in which people cannot properly synthesize cholesterol. One such disease is Smith-Lemli-Opitz syndrome (also called “SLOS,” or 7-dehydrocholesterol reductase deficiency) which is a metabolic and congenital disorder leading to a number of problems including autism, mental retardation, lack of muscle, and many others.
Cholesterol is absolutely vital for our existence. Every cell in our body is surrounded by a membrane. These membranes are largely responsible for fluidity and permeability, which essentially control how a cell moves, how it interacts with other cells, and how it transports “important” things in and out. Cholesterol is one of the main building blocks used to make cell membranes (in particular, the ever-important “lipid bilayer” of the cell membrane).
Beyond cholesterol’s role in allowing cells to even exist, it also serves an important role in the synthesis of vitamins and steroid hormones, including sex hormones and bile acids. Make sure you take a look at the picture of steroid hormones synthesis and compare it to that of cholesterol (above). If this comparison doesn’t convince you of the vital importance of cholesterol, nothing I say will.
One of the unfortunate results of the eternal need to simplify everything is that we (i.e., the medical establishment) have done the public a disservice by failing to communicate that there is no such thing as “bad” cholesterol or “good” cholesterol. All cholesterol is imperative for life to exist!
The only “bad” outcome is when cholesterol ends up inside of the wall of an artery, most famously the inside of a coronary artery or a carotid artery, AND leads to an inflammatory cascade which results in the obstruction of that artery (make sure you check out the pictures in the links above). When one measures cholesterol in the blood we really do not know the final destination of those cholesterol molecules!
3. The cholesterol we eat has little to do with the cholesterol we measure in our bloodstream.
We ingest (i.e., take in) cholesterol in many of the foods we eat and our body produces (“synthesizes”) cholesterol de novo from various precursors. About 25% of our daily “intake” of cholesterol – roughly 300 to 500 mg – comes from what we eat (called exogenous cholesterol), and the remaining 75% of our “intake” of cholesterol – roughly 800 to 1,200 mg – is made by our body (called endogenous production). To put these amounts in context, consider that total body stores of cholesterol are about 30 to 40 gm (i.e., 30,000 to 40,000 mg) and most of this resides within our cell membranes. Nearly every cell in the body can produce cholesterol, and thus very few cells actually require a delivery of cholesterol. Cholesterol is required by all cell membranes and to produce steroid hormones and bile acids.
Of this “made” or “synthesized” cholesterol, our liver synthesizes about 20% of it and the remaining 80% is synthesized by other cells in our bodies. The synthesis of cholesterol is a complex four-step process (with 37 individual steps) that I will not cover here, but I want to point out how tightly regulated this process is, with multiple feedback loops. In other words, the body works very hard (and very “smart”) to ensure cellular cholesterol levels are within a pretty narrow band (the overall process is called cholesterol homeostasis). Excess cellular cholesterol will crystalize and cause cellular apoptosis (programmed cell death). Plasma cholesterol levels (which is what clinicians measure with standard cholesterol tests) often have little to do with cellular cholesterol, especially artery cholesterol, which is what we really care about. For example, when cholesterol intake is decreased, the body will synthesize more cholesterol and/or absorb (i.e., recycle) more cholesterol from our gut. The way our body absorbs and regulates cholesterol is really amazing, so I want to spend a bit of time discussing it.

The blue circle in this figure represents something called a Niemann-Pick C1-like 1 protein (NPC1L1). It sits at the apical surface of enterocytes and it promotes active influx (i.e., bringing in) of gut luminal unesterified cholesterol (UC) as well as unesterified phytosterols into the enterocyte. Think of this NPC1L1 as the ticket-taker at the door of the bar (where the enterocyte is the “bar”); he lets most cholesterol (“people”) in. However, NPC1L1 cannot distinguish between cholesterol (“good people”) and phytosterol (“bad people” – for reasons I won’t discuss here) or even too much cholesterol (“too many people”).
The pink circle in this figure represents a structure called the adenosine triphosphate (ATP)-binding cassette (ABC) transporters ABCG5 and ABCG8. This structure promotes active efflux (i.e., kicking out) of unesterified sterols (cholesterol and plant sterols – of which over 40 exist) from enterocytes back into the intestinal lumen for excretion. Think of ABCG5/G8 as the bouncer at the bar; he gets rid of the really bad people (e.g., phytosterols, as they serve no purpose in humans) you don’t want in the bar who snuck past the ticket-taker (NPC1L1). Of course, in cases of hyperabsorption (i.e., where the gut absorbs too much of a good thing) they can also efflux out un-needed cholesterol. Along this analogy, once too many “good people” get in the bar, fire laws are violated and some have to go. The enterocyte has “sterol-excess sensors” (a nuclear transcription factor called LXR) that do the monitoring, and these sensors activate the genes that regulate NPC1L1 and ABCG5/G8.
There is another nuance to this, which is where the CE versus UC distinction comes in:
Only free or unesterified cholesterol (UC) can be absorbed through gut enterocytes. In other words, cholesterol esters (CE) cannot be absorbed because of the bulky side chains they carry.
Much (> 50%) of the cholesterol we ingest from food is esterified (CE), hence we don’t actually absorb much, if any, exogenous cholesterol (i.e., cholesterol in food).
Furthermore, most of the unesterified cholesterol (UC) in our gut (on the order of about 85%) is actually of endogenous origin (meaning it was synthesized in bodily cells and returned to the liver), which ends up in the gut via biliary secretion and ultimately gets re-absorbed by the gut enterocyte. The liver is only able to efflux (send out via bile into the gut) UC, but not CE, from hepatocytes (liver cells) to the biliary system. Liver CE cannot be excreted into bile. So, if the liver is going to excrete CE into bile and ultimately the gut, it needs to de-esterify it using enzymes called cholesterol esterolases which can convert liver CE to UC.
4. The cholesterol in our bloodstream has little to do with the cholesterol in our artery walls (i.e., atherosclerosis).
To understand how cholesterol travels around our body requires some understanding of the distinction between hydrophobic and hydrophilic. A molecule is said to be hydrophobic (also called nonpolar) if it repels water, while a molecule is said to be hydrophilic (also called polar) if it attracts water. Think of your veins, arteries, and capillaries as the “waterways” or rivers of your body. Cholesterol is precious “cargo” that needs to move around, but it needs a “boat” to carry it.
The proteins that traffic collections of lipids are called apoproteins. Once bound to lipids they are called apolipoproteins, and the protein wrapped “vehicle” that transports the lipids are called lipoproteins. Many of you have probably heard this term before, but I’d like to ensure everyone really understands their important features. A crucial concept is that, for the most part, lipids go nowhere in the human body unless they are a passenger inside a protein wrapped vehicle called a lipoprotein. As their name suggests, lipoproteins are part lipid and part protein. They are mostly spherical structures which are held together by a phospholipid membrane (which, of course, contains free cholesterol). The figure below shows a schematic of a lipoprotein.
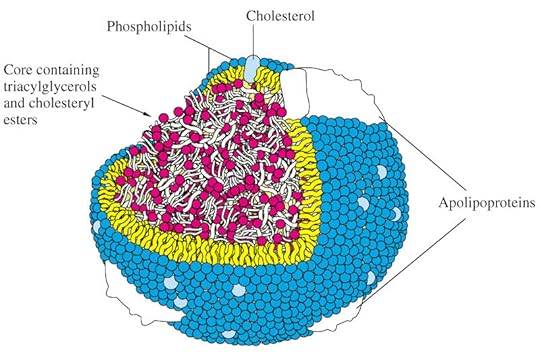
You will also notice variable-sized proteins on the surface of the lipid membrane that holds the structure together. The most important of these proteins are called apolipoproteins, as I alluded to above. The apolipoproteins on the surface of lipoprotein molecules serve several purposes including:
Assisting in the structural integrity and solubility of the lipoprotein;
Serving as co-factors in enzymatic reactions;
Acting as ligands (i.e., structures that help with binding) for situations when the lipoprotein needs to interact with a receptor on a cell.
Apolipoproteins come in different shapes and sizes which determine their “class.” Without getting into the details of protein structure and folding, let me focus on two important classes: apolipoprotein A-I and apolipoprotein B. ApoA-I is the apolipoprotein that wraps HDL particles. ApoB is the apolipoprotein that wraps VLDL, IDL, and LDL particles.
5. The only way sterols end up in artery walls – the one place we don’t want them to be – is if the sterols are carried there by an apoB-containing lipoprotein particle.
So what drives a LDL particle to do something as sinister as to leave the waterway (i.e., the bloodstream) and “illegally” try to park at a dock (i.e., behind an endothelial cell)? Well, it is a gradient driven process which is why particle number is the key driving parameter.
As it turns out, this is probably a slightly less important question than the next one: what causes the LDL particle to stay there? In the parlance of our metaphor, not only do we want to know why the boat leaves the waterway to illegally park in the dock with its precious cargo, but why does it stay parked there? This phenomenon is called “retention” in lipidology-speak.
Finally, if there was some way a LDL particle could violate the endothelium, AND be retained in the space behind the cell (away from the lumen on the side aptly called the sub-endothelial space) BUT not elicit an inflammatory (i.e., immune) response, would it matter?
I don’t know. But it seems that not long after a LDL particle gets into the sub-endothelial space and takes up “illegal” residence (i.e., binds to arterial wall proteoglycans), it is subject to oxidative forces, and as one would expect an inflammatory response is initiated. The result is full blown mayhem. Immunologic gang warfare breaks out and cells called monocytes and macrophages and mast cells show up to investigate. When they arrive and find the LDL particle, they do all they can to remove it. In some cases, when there are few LDL particles, the normal immune response is successful. But, it’s a numbers game. When LDL particle invasion becomes incessant, even if the immune cells can remove some of them, it becomes a losing proposition and the actual immune response to the initial problem becomes chronic and maladaptive and expands into the space between the endothelium and the media.
The multiple-sterol-laden macrophages or foam cells coalesce, recruit smooth muscle cells, induce microvascularization, and before you know it complex, inflamed plaque occurs. Microhemorrhages and microthrombus formations occur within the plaque. Ultimately the growing plaque invades the arterial lumen or ruptures into the lumen inducing luminal thrombosis. Direct luminal encroachment by plaque expansion or thrombus formation causes the lumen of the artery to narrow, which may or may not cause ischemia.
Check back tomorrow for Part 2 of The Straight Dope on Cholesterol: 10 Things You Need to Know

August 28, 2012
20 Ways to Cultivate IE in Your Life
 Recently, I caught up with an old friend of mine. He’d just returned home from a trip to the Northern Midwest, where they rented a cabin on one of the Great Lakes with family. He showed me pictures of his kids. Being used to a landlocked existence, his 6-year-old daughter had been wholly enthralled by the vastness of the lake, which she referred to as the ocean throughout the entire trip. One afternoon as their younger child napped, he took his older daughter to a nearby park reserve for a bit of exploration. She was mesmerized by a river gorge and more so by the brave, unruly souls who were hurling themselves off a rock ledge into the borderline hypothermic water hole below. What ultimately drew her in that afternoon, he explained, was a sandy beach cove lined with enough tall jagged boulders to make a dramatic show of the temperamental lake’s waves. She ran along that beach all afternoon, he said, scrambling up rocks, dancing along the shore, teasing the waves to catch her bare feet, and squealing at the cold and sheer exhilaration. In one picture, we stood looking out across the lake with outstretched arms, “commanding the sea,” as her dad described laughingly. When you’re six, after all, that’s entirely within the realm of possibility…. My friend’s eyes reflected a deep, parental sense of awe as he showed me the pictures and told me about that afternoon, his favorite time of the entire trip. He clearly marveled at his daughter’s innocent, wild wonder in the same way she marveled at the “ocean” that day.
Recently, I caught up with an old friend of mine. He’d just returned home from a trip to the Northern Midwest, where they rented a cabin on one of the Great Lakes with family. He showed me pictures of his kids. Being used to a landlocked existence, his 6-year-old daughter had been wholly enthralled by the vastness of the lake, which she referred to as the ocean throughout the entire trip. One afternoon as their younger child napped, he took his older daughter to a nearby park reserve for a bit of exploration. She was mesmerized by a river gorge and more so by the brave, unruly souls who were hurling themselves off a rock ledge into the borderline hypothermic water hole below. What ultimately drew her in that afternoon, he explained, was a sandy beach cove lined with enough tall jagged boulders to make a dramatic show of the temperamental lake’s waves. She ran along that beach all afternoon, he said, scrambling up rocks, dancing along the shore, teasing the waves to catch her bare feet, and squealing at the cold and sheer exhilaration. In one picture, we stood looking out across the lake with outstretched arms, “commanding the sea,” as her dad described laughingly. When you’re six, after all, that’s entirely within the realm of possibility…. My friend’s eyes reflected a deep, parental sense of awe as he showed me the pictures and told me about that afternoon, his favorite time of the entire trip. He clearly marveled at his daughter’s innocent, wild wonder in the same way she marveled at the “ocean” that day.
Last week I introduced the Primal principle of IE – intermittent euphoria – to re-prioritize the peaks of life – the thrill, wonder, and amazement possible in this existence of ours. Thriving, after all, isn’t about accomplishing an inventory of “healthy” behaviors each day. It’s about living out the full measure of your humanity – in all its depth, vigor, and vitality. Euphoria, of course, isn’t something you can summon at will. It doesn’t lend itself to a handy checklist. In fact, it most often catches us unaware. Nonetheless, we can cultivate a mindset and lifestyle conducive to euphoria – one that seeks adventure, values awe, and relishes discovery.
Euphoria comes when we venture ourselves in some way. We give it space when we let go of our self chatter, inner list making, and task orientation. We open ourselves to it when we release the tendency, as author Paul Pearsall puts it, to be “too self conscious to be fully conscious.” In prioritizing IE, we can pursue experiences with the power to elicit deep feeling (e.g. fear, awe, connection) and simply cultivate a mindset open to wonder. Here you’ll find some modestly proposed ideas to galvanize a good Primal life with some intermittent opportunity. I hope you’ll add your own ideas to the conversation.
Witness the wonder others experience. Seeing your child filled with awe is undoubtedly one of the most rewarding moments of parenting. You can encounter it, however, in your aging parents, close friends, your partner, nieces/nephews, and complete strangers. Seeing that unmistakable look in others’ eyes inevitably unlocks something in ourselves. We can be deeply moved witnessing another person’s awe.
Make your own list of “natural wonders” you want to see. Make #1 your next vacation destination.
Find – and regularly enjoy – music that sends chills running through you. If you can, see it performed live.
Spend an entire day noticing things you know you otherwise overlook in a typical hurried day. Observe puddle reflections. Examine the trees in your neighborhood. Watch your children’s myriad expressions throughout an afternoon hike.
Read books that make you feel you’re living inside the story.
Watch (or attend!) events that evoke a sense of connectedness and wonder. It’s little surprise I’m a fan of the Olympics. To this day, I relish the moment in the opening ceremonies of the Barcelona Summer Games when the archer lit the cauldron with that flaming arrow. How many hundreds of millions – or perhaps billions – of people around the world hung on the arc of that arrow’s trajectory?
Go for a long night walk in the woods, through the fields, along a beach. No flashlights.
Invest in experiences.
Volunteer on the front line of need. You may feel intimidated or maybe awkward. You won’t know the perfect thing to say handing out dinner to a young family in a soup kitchen. You will come away each time, however, having done something meaningful and having been changed in the process.
Take up an “extreme” sport (it’s all relative here, folks) you’ve been pondering (e.g. deep sea diving/snorkeling, mountain climbing/tree climbing, trail running/trail hiking). Take a lesson. Sign up for an outing. If you’re already an extreme enthusiast, find a new destination or variation of your sport to challenge yourself.
Indulge in nostalgia. Reread old letters or watch family videos. Getting wistful over memories can enhance our feeling of connectedness.
Recall past experiences of euphoria. What have been the most thrilling, most meaningful hours of your life? What would’ve inspired you as a kid? Bring that fascination to whatever happens this day.
Spend a day doing a novel kind of exploring. Go caving, map a trail, or set out on a hike with an artistic (e.g. photographic journal) or scientific (e.g. bird cataloging) goal in mind.
Take an adventure vacation – as a personal retreat or a family project. Bike across the state, climb a triad of mountains, run a lighthouse for a week. It will be much more memorable than a hotel pool or standing in line at Orlando.
Do something that scares you. (Anyone?) Revel in the sharp awareness that overtakes you. It’s a poignant dimension of being fully alive.
Take on a creative project unlike anything you’ve committed to before. What do you want your opus to be? Begin it today.
Spend a day in a busy public place (e.g. train station, popular coffee shop) and people watch. See how much you can learn or ascertain about the characters you encounter. Imagine their stories.
Borrow a telescope or visit an area planetarium for their late night star gazing program.
Find a beautiful vista-side or secluded outdoor “sit spot” and see what reveals itself in an afternoon.
Put on a 6-year-old’s mindset for the day. Go out into the world – preferably the natural world. “Command” the waves, conquer the squirrels, orchestrate the clouds, hang from the tree branches, journey an animated path full of risk and marvel.
Thanks for reading today, everyone. Share what moves you to experience IE in life these days. Have a great week!
Get the Primal Blueprint Fitness eBook, Free Health Tips and Primal Recipes Delivered to Your Inbox

August 27, 2012
Dear Mark: Does Eating a Low Carb Diet Cause Insulin Resistance?
 Despite all the success you might have had with the Primal way of life, doubts can still nag at you. Maybe it’s something you read, or something someone said to you, or a disapproving glance or offhand comment from a person you otherwise respect, but it’s pretty common when you’re doing something, like giving up grains, avoiding processed food, or eating animal fat, that challenges deeply-and-widely held beliefs about health and wellness. It doesn’t really even matter that you’re losing weight or seem to be thriving; you may still have questions. That’s healthy and smart, and it’s totally natural.
Despite all the success you might have had with the Primal way of life, doubts can still nag at you. Maybe it’s something you read, or something someone said to you, or a disapproving glance or offhand comment from a person you otherwise respect, but it’s pretty common when you’re doing something, like giving up grains, avoiding processed food, or eating animal fat, that challenges deeply-and-widely held beliefs about health and wellness. It doesn’t really even matter that you’re losing weight or seem to be thriving; you may still have questions. That’s healthy and smart, and it’s totally natural.
A question I’ve been getting of late is the effect of reducing carb intake on insulin sensitivity. It’s often bandied about that going low carb is good for folks with insulin resistance, but it’s also said that low carb can worsen insulin resistance. Are both true and, if so, how do they all jibe together? That’s what the reader was wondering with this week’s question:
Hi Mark,
I’ve been Primal for a few months now and love it. Lowering my carbs and upping my animal fat helped me lose weight and gain tons of energy (not too shabby for a middle-aged guy!). However, I’m a little worried. I’ve heard that low carb diets can increase insulin resistance. Even though I’ve done well and feel great, should I be worried about insulin resistance? Do I need to increase my carb intake? I always thought low carb Primal was supposed to improve insulin function.
Vince
Going Primal usually does improve insulin sensitivity, both directly and in a roundabout way. It improves directly because you lose weight, you reduce your intake of inflammatory foods, you lower systemic inflammation (by getting some sun, smart exercise, omega-3s, and reducing or dealing with stress), and you eat a wide variety of plants, animals, and herbs with anti-inflammatory and/or insulin-sensitizing effects. It improves indirectly because you are removing the thing that exacerbates the condition – large amounts of carbohydrates – and thus avoiding the negative effects. You might still be insulin resistant, but since you aren’t cramming your face with carbs anymore, you don’t notice it.
And sure enough, the weight loss studies indicate that during weight loss, very low carb diets improve insulin sensitivity:
In overweight women, a diet with less than 10% of calories as carbs improved insulin sensitivity, while a 30% fat, low-fat diet reduced it.
In obese, insulin-resistant women, both high-fat and high-protein low-carb diets reduced insulin resistance, while the high-carb diet was not as effective.
In obese kids, a very low carb diet was able to reduce indices of insulin resistance along with bodyweight and body fatness.
However, going very low carb – to around or below 10% of calories, or full-blown ketogenic – can induce ”physiological” insulin resistance. Physiological insulin resistance is an adaptation, a normal biological reaction to a lack of dietary glucose. As I’ve said in the past, the brain must have glucose. It can use ketones and lactate quite effectively, thus reducing the glucose requirement, but at the end of the day it still requires a portion of glucose. Now, in a low-glucose state, where the body senses that dietary glucose might not be coming anytime soon, peripheral insulin resistance is triggered. This prevents the muscles from taking up “precious” glucose that the brain requires. The brain’s sensitivity to insulin is preserved, allowing it to grab what glucose it needs from the paltry – but sufficient – levels available to it.
It appears that weight loss is the deciding factor, and since low carb diets tend to be more effective at inducing weight loss in subjects, they also tend to be better at reducing insulin resistance in insulin-resistant, overweight people. Once you’re lean and weight stable, though, very low carb diets (less than 10% of calories from carbs) can reduce insulin sensitivity. This is normal and totally necessary in the context of a very low carb diet. If we didn’t become insulin resistant while eating very low carb, our brain wouldn’t be able to get the glucose it needed to keep us alive.
Okay, but what about dietary amino acids? If our tissues are insulin resistant on very low carb, and insulin also promotes muscle protein synthesis, doesn’t that mean the amino acids from the protein we eat have a harder time getting into our muscles? You might think that, but that’s not how it plays out in the real world. In actual clinical trials, low carb diets are consistently linked with preservation of lean mass during weight loss. People on low carb diets lose more fat and less lean mass.
Muscle glycogen stores may be depleted, but if you want to fill those back up, you can do so quite effectively post workout, even when you’re low carb and otherwise physiologically insulin resistant. A bout of weight lifting, sprints, or even just regular walking can improve your ability to tolerate and handle glucose by making you more insulin-sensitive. This holds true even for the otherwise insulin-resistant.
In the end, insulin resistance on very low carb appears to be a physiological adaptation to spare glucose for the brain and prevent your muscles from gobbling it up. I see no reason to think it’s a pathological problem, especially given the droves of success stories on this site and others from people who have lost weight, torn up prescriptions, boggled the minds of doctors, and reclaimed their once-failing health through a low-carb Primal way of eating and living. I could be wrong, and time will tell, I suppose, but I doubt it.
Besides, there are far more pressing potentially negative influences on insulin sensitivity that we can be addressing, like:
Sedentary lifestyles. And I’m not just talking about strength training and high-intensity sprints; simple, basic low-level physical activity, like walking on a daily basis, can have a powerful effect on insulin resistance.
Unchecked and out-of-control appetites. Weight gain and an excess of energy (that the mitochondria can’t handle for whatever reason) are potent causes of insulin resistance.
Environmental pollutants and toxins like BPA and various fungicides can have negative effects on insulin sensitivity.
To sum up, I don’t think you need to worry about insulin resistance as long as you’re still losing weight – which you appear to be doing – since weight loss exerts a powerful effect on insulin sensitivity. However, once you’re lean, or have stalled without changing anything, moving back toward the 100-150 Primal carb gram range will keep your insulin receptors “honest” without causing weight gain (and it may even jumpstart weight loss again). Lifting heavy things, sprinting every once in awhile (in a manner suitable for your physical limitations), and doing lots of slow moving will also keep you insulin-sensitive, particularly after the physical activity.
Thanks for reading, folks, and I hope I cleared this up for you without raising too many more questions. Let me know your experience in the comment section.
Grab The Primal Blueprint Cookbook Today and Receive Free S&H and a Free Primal Blueprint Poster

August 26, 2012
Weekend Link Love
Research of the WeekEarly usage of antibiotics appears to predispose kids to obesity later on in life.
Does a low-carb diet simulate the beneficial effects of exercise? Michael Eades weighs in on a new study.
Interesting Blog Posts
Eating healthy, even organic stuff from Whole Foods, doesn’t have to be expensive. It just takes a little effort.
Beth over at Weight Maven has a nice roundup of AHS-related posts and pics.
Andrew Badenoch of Evolvify talks about building an intentional paleo community. What do you think? Would you join?
Media, Schmedia
Look who’s decided to start promoting the use of lard!
Sauerkraut is dangerous stuff.
Everything Else
Should you be icing your injured tissues? First, hear what K-Starr has to say, then head over to 70′s Big for Justin Lascek’s take on it. Oh, and be sure to seriously, seriously consider pre-ordering the upcoming MWOD book, Becoming a Supple Leopard, for a chance to win some sweet raffle prizes.
Are you a budding “watermelon student”? I know I am. Learn how to eat a watermelon in this video tutorial by Tom Willett.
Recipe Corner
Here’s my blatant attempt to attract followers of Ray Peat: sour gummy stars. Reduce the honey if you’re Primal, sub orange juice and powdered aspirin if Peat-inspired.
Gazpacho with gusto. To be honest, though, the gusto is optional.
Time Capsule
One year ago (Aug 26 – September 1)
The Role of Fighting in a Primal Life – Does controlled, mutually-agreed upon violence have a role in Primal living?
How to Eat Meat: Transitioning Away From Vegetarianism – How’s a vegetarian supposed to do it?
Comment of the Week
I’ve been discussing the “dumbocity” of the egg study with our hens this week to reassure them that they are doing a good job. They were getting a little paranoid there for a while, but once I explained to them that their brains were bigger than the brains of the scientists, they relaxed and went back to chasing bugs.
- Decaf Debi, I’d love to try their eggs.
Grab The Primal Blueprint Cookbook Today and Receive Free S&H and a Free Primal Blueprint Poster

August 25, 2012
Pork-Stuffed Jalapeño Peppers
 A fresh jalapeño pepper is the perfect delivery vehicle for meat or seafood. When the pepper is cut open, there’s just enough room to stuff a nibble of ground meat, sausage, shrimp or crab. The delicious edible package is sealed with a strip of bacon that drips fatty flavor into the pepper. A stuffed jalapeño can be eaten with your fingers in one or two bites (it’s delicious either hot or cold) and the addictive spicy flavor keeps you coming back for more.
A fresh jalapeño pepper is the perfect delivery vehicle for meat or seafood. When the pepper is cut open, there’s just enough room to stuff a nibble of ground meat, sausage, shrimp or crab. The delicious edible package is sealed with a strip of bacon that drips fatty flavor into the pepper. A stuffed jalapeño can be eaten with your fingers in one or two bites (it’s delicious either hot or cold) and the addictive spicy flavor keeps you coming back for more.
Italian pork sausage is especially good in the pepper, if you want to go all out with pork flavor. Or, you can lighten things up a little by finely chopping raw shrimp in a food processor and stuffing that inside the pepper instead.
These bite-sized, savory treats are definitely popular appetizers, but why not serve them for breakfast too? Alongside a plate of eggs a stuffed jalapeño pepper is ridiculously good.
Servings: 20 stuffed jalapeños
Ingredients:

10 fresh jalapeños, sliced in half lengthwise, white membrane and seeds removed
10 slices of bacon, cut in half
1/2 pound (230 g) of loose pork sausage or other seasoned ground meat
Instructions:
Heat oven to 400 ºF (205 ºC)
Use your fingers to stuff meat into each jalapeño half.
Snugly wrap a piece of bacon around the pepper. Secure it with a toothpick.

You can put the peppers directly on baking sheet or pan, but the fat that drips off the bacon will make them a little greasy. To avoid this, set a cooling rack on top of a baking pan and put the pepper on the rack.

Bake for 25 minutes, until bacon is crispy.
Grab The Primal Blueprint Cookbook Today and Receive Free S&H and a Free Primal Blueprint Poster

Mark Sisson's Blog

- Mark Sisson's profile
- 199 followers


{kind=link}