
Yu-Han Chao's Blog, page 4
November 28, 2019
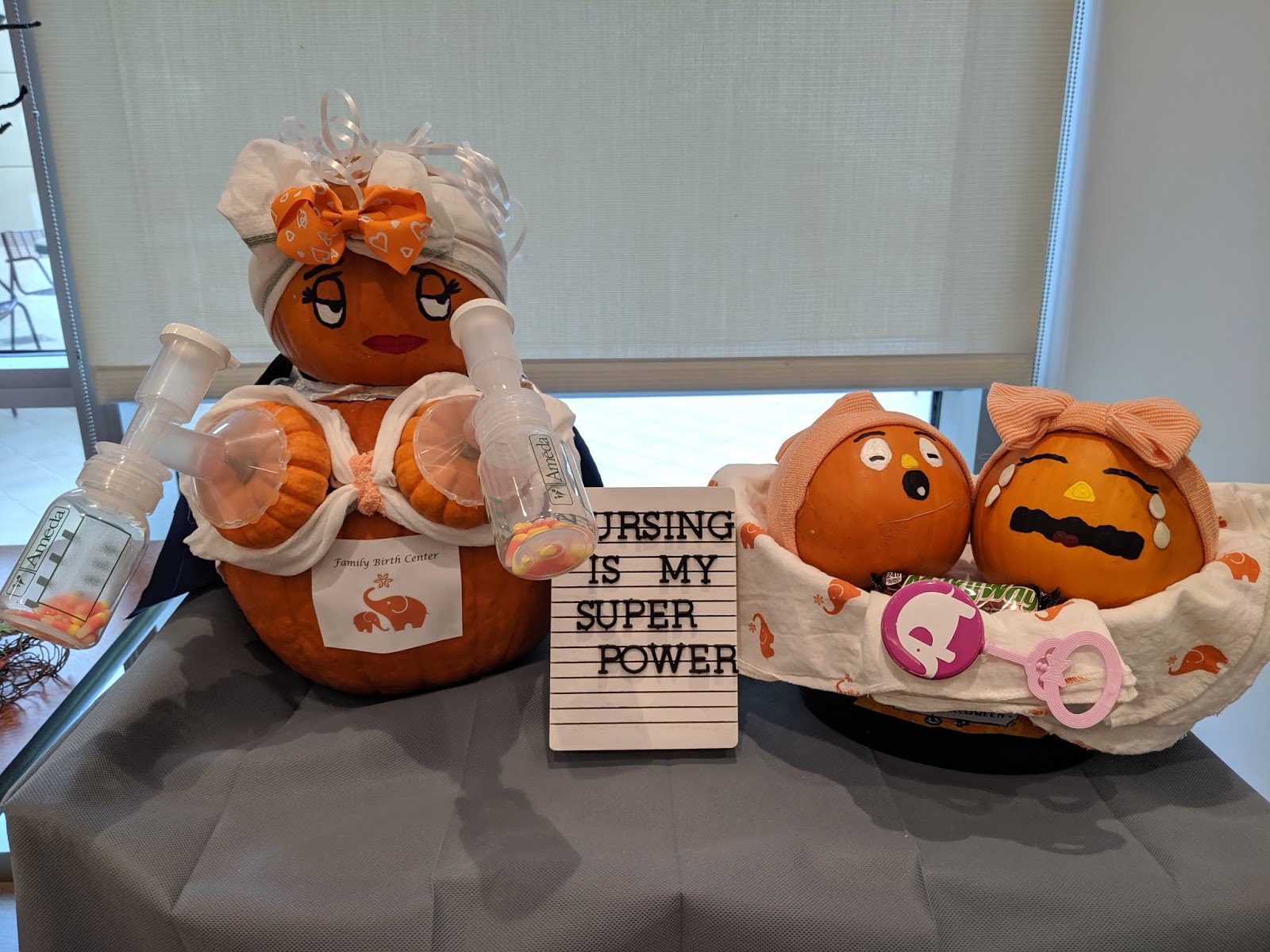
Baby Nurse
There are many parallels between motherhood and nursing, puns not withstanding. Both are caring and giving professions, though motherhood is an eternal job, while nurses can at least retire...one day.
 From Mercy's pumpkin contest. Really wanted this one to win.
From Mercy's pumpkin contest. Really wanted this one to win.
As it turns out, there are parallels between babies and being a nurse, at least when one happens to be a baby nurse.
A newborn baby communicates through cries and sees best 8-12 inches away, like a new nurse with tunnel vision, looking for where to chart which of 100 things in the computer system.
A 1-month-old has fully-developed hearing, responds to familiar sounds, and can tell the difference between her mother's breastmilk and random people's breastmilk (?) One month into her position, a new RN develops a better ear for all the heart and lung sounds, and continues to hear all the call lights and IV poles beeping and phones ringing long after going home. She can also sniff out coffee from a distance.
A two month-old begins to lift her head and recognizes faces. Two months in, a nurse finally feels slightly head-above-water, and recognizes familiar faces on the floor and in the rooms, because: readmissions.
A three-month baby makes eye contact. After her 90-day observation, a new nurse can remove her "new employee" badge so she can stand slightly taller, look people in the eye in the elevator and smile, knowing they're not about to comment on the new employee badge.
A baby at five months sees colors better and listens to voices. A nurse, five months in, may be better at intuiting how patients "look" and interpreting subtle changes in heart and lung sounds.
A six-month baby is learning to sit up unassisted. Off orientation, a new nurse is "on her own," but not quite, because she has a team of nurses, and an interdisciplinary team working with her on the floor.
A ten-month-old picks up things with thumb and pointer finger. Ten months in, maybe a nurse can find invisible veins for an IV through touch alone, no vein-finder or tournequette required (we'll see about that...)
By one year, a baby can look and listen at the same time. By then a nurse should be able to assess and chart, help patients to the restroom, call the doctor, answer call lights, troubleshoot equipment, and help out her colleagues, all at the same time. We'll see about that, too.
 From Mercy's pumpkin contest. Really wanted this one to win.
From Mercy's pumpkin contest. Really wanted this one to win.
As it turns out, there are parallels between babies and being a nurse, at least when one happens to be a baby nurse.
A newborn baby communicates through cries and sees best 8-12 inches away, like a new nurse with tunnel vision, looking for where to chart which of 100 things in the computer system.
A 1-month-old has fully-developed hearing, responds to familiar sounds, and can tell the difference between her mother's breastmilk and random people's breastmilk (?) One month into her position, a new RN develops a better ear for all the heart and lung sounds, and continues to hear all the call lights and IV poles beeping and phones ringing long after going home. She can also sniff out coffee from a distance.
A two month-old begins to lift her head and recognizes faces. Two months in, a nurse finally feels slightly head-above-water, and recognizes familiar faces on the floor and in the rooms, because: readmissions.
A three-month baby makes eye contact. After her 90-day observation, a new nurse can remove her "new employee" badge so she can stand slightly taller, look people in the eye in the elevator and smile, knowing they're not about to comment on the new employee badge.
A baby at five months sees colors better and listens to voices. A nurse, five months in, may be better at intuiting how patients "look" and interpreting subtle changes in heart and lung sounds.
A six-month baby is learning to sit up unassisted. Off orientation, a new nurse is "on her own," but not quite, because she has a team of nurses, and an interdisciplinary team working with her on the floor.
A ten-month-old picks up things with thumb and pointer finger. Ten months in, maybe a nurse can find invisible veins for an IV through touch alone, no vein-finder or tournequette required (we'll see about that...)
By one year, a baby can look and listen at the same time. By then a nurse should be able to assess and chart, help patients to the restroom, call the doctor, answer call lights, troubleshoot equipment, and help out her colleagues, all at the same time. We'll see about that, too.


November 8, 2019
Bills
You can pay a bill, date a Bill (and/or kill him), bill someone, or support a bill such as AB3087, which addresses California's health care cost, quality, and equity.
 While many healthcare facilities oppose AB3087 as it puts the state of California in charge of setting prices for hospital stays, doctor’s visits, and other services covered by commercial insurers, the high cost of healthcare has a far greater correlation with insurance and pharmaceutical companies rather than hospital or provider billing practices.
While many healthcare facilities oppose AB3087 as it puts the state of California in charge of setting prices for hospital stays, doctor’s visits, and other services covered by commercial insurers, the high cost of healthcare has a far greater correlation with insurance and pharmaceutical companies rather than hospital or provider billing practices.
AB3087 aims to reduce costs to consumers by limiting the amounts hospitals/providers are allowed to bill for services, which on the surface appears to strain already-impacted human resources and providers in the area. However, another way of viewing the issue is that if healthcare billing is capped or restricted, insurance costs and pharmaceutical company upcharges should by association be restricted as well. Healthcare should not be a for-profit endeavor for commercial insurers and the pharmaceutical industry, especially not in a state with a high number of homeless, uninsured, and undocumented clients.
Many hospitals are non-profit facilities that turn no patients away. Rather than making healhcare facilities and their personnel “take the cut” from AB3087, which is a common assumption of what might result from the bill, ideally, changes in billing should be negotiated with insurance companies that charge high premiums to “cover” hospital stays and pharmaceutical companies overcharging for newer variations of standard medications, while many uninsured patients receive no preventative care and end up in emergency rooms with severe, costly complications for which the hospital then receives limited, if any, compensation.
Many scholars have attempted to explain the complicated finances of the U.S. healthcare industry. In his article, “Healthcare Spending: Plenty of Blame to Go Around,” Prof. Gary Branner at Rutgers Graduate School of Business states, “The United States is the only profit-motivated healthcare system in the world, and perhaps it is no coincidence that this country also has the most expensive healthcare of any nation.” He continues, “Politicians point fingers at pharmaceutical manufacturers, who in turn blame health insurers and pharmacy benefit managers.” This is a complex issue and playing the blame game benefits no one, especially not the people of California.
Language in AB3087, such as that it “would prohibit a health care provider from billing or collecting an amount other than the applicable cost sharing from an individual” may be amended to be less biased in its implication that health care providers are (over)billing when the increasing healthcare costs are associated with various levels of insurance and pharmaceutical costs.
Having grown up in Taiwan, which boasts universal healthcare for all its residents, I also dream of a day when the likes of Senate Bill 562, which proposes universal state-financed healthcare, might come to pass, but for now, it seems that at the very least, the hospitals and healthcare workers who are overworked, understaffed, and paying high insurance premiums and student loans themselves should not be villainized in a well-meaning bill intended to benefit the public.
 While many healthcare facilities oppose AB3087 as it puts the state of California in charge of setting prices for hospital stays, doctor’s visits, and other services covered by commercial insurers, the high cost of healthcare has a far greater correlation with insurance and pharmaceutical companies rather than hospital or provider billing practices.
While many healthcare facilities oppose AB3087 as it puts the state of California in charge of setting prices for hospital stays, doctor’s visits, and other services covered by commercial insurers, the high cost of healthcare has a far greater correlation with insurance and pharmaceutical companies rather than hospital or provider billing practices.AB3087 aims to reduce costs to consumers by limiting the amounts hospitals/providers are allowed to bill for services, which on the surface appears to strain already-impacted human resources and providers in the area. However, another way of viewing the issue is that if healthcare billing is capped or restricted, insurance costs and pharmaceutical company upcharges should by association be restricted as well. Healthcare should not be a for-profit endeavor for commercial insurers and the pharmaceutical industry, especially not in a state with a high number of homeless, uninsured, and undocumented clients.
Many hospitals are non-profit facilities that turn no patients away. Rather than making healhcare facilities and their personnel “take the cut” from AB3087, which is a common assumption of what might result from the bill, ideally, changes in billing should be negotiated with insurance companies that charge high premiums to “cover” hospital stays and pharmaceutical companies overcharging for newer variations of standard medications, while many uninsured patients receive no preventative care and end up in emergency rooms with severe, costly complications for which the hospital then receives limited, if any, compensation.
Many scholars have attempted to explain the complicated finances of the U.S. healthcare industry. In his article, “Healthcare Spending: Plenty of Blame to Go Around,” Prof. Gary Branner at Rutgers Graduate School of Business states, “The United States is the only profit-motivated healthcare system in the world, and perhaps it is no coincidence that this country also has the most expensive healthcare of any nation.” He continues, “Politicians point fingers at pharmaceutical manufacturers, who in turn blame health insurers and pharmacy benefit managers.” This is a complex issue and playing the blame game benefits no one, especially not the people of California.
Language in AB3087, such as that it “would prohibit a health care provider from billing or collecting an amount other than the applicable cost sharing from an individual” may be amended to be less biased in its implication that health care providers are (over)billing when the increasing healthcare costs are associated with various levels of insurance and pharmaceutical costs.
Having grown up in Taiwan, which boasts universal healthcare for all its residents, I also dream of a day when the likes of Senate Bill 562, which proposes universal state-financed healthcare, might come to pass, but for now, it seems that at the very least, the hospitals and healthcare workers who are overworked, understaffed, and paying high insurance premiums and student loans themselves should not be villainized in a well-meaning bill intended to benefit the public.
October 12, 2019
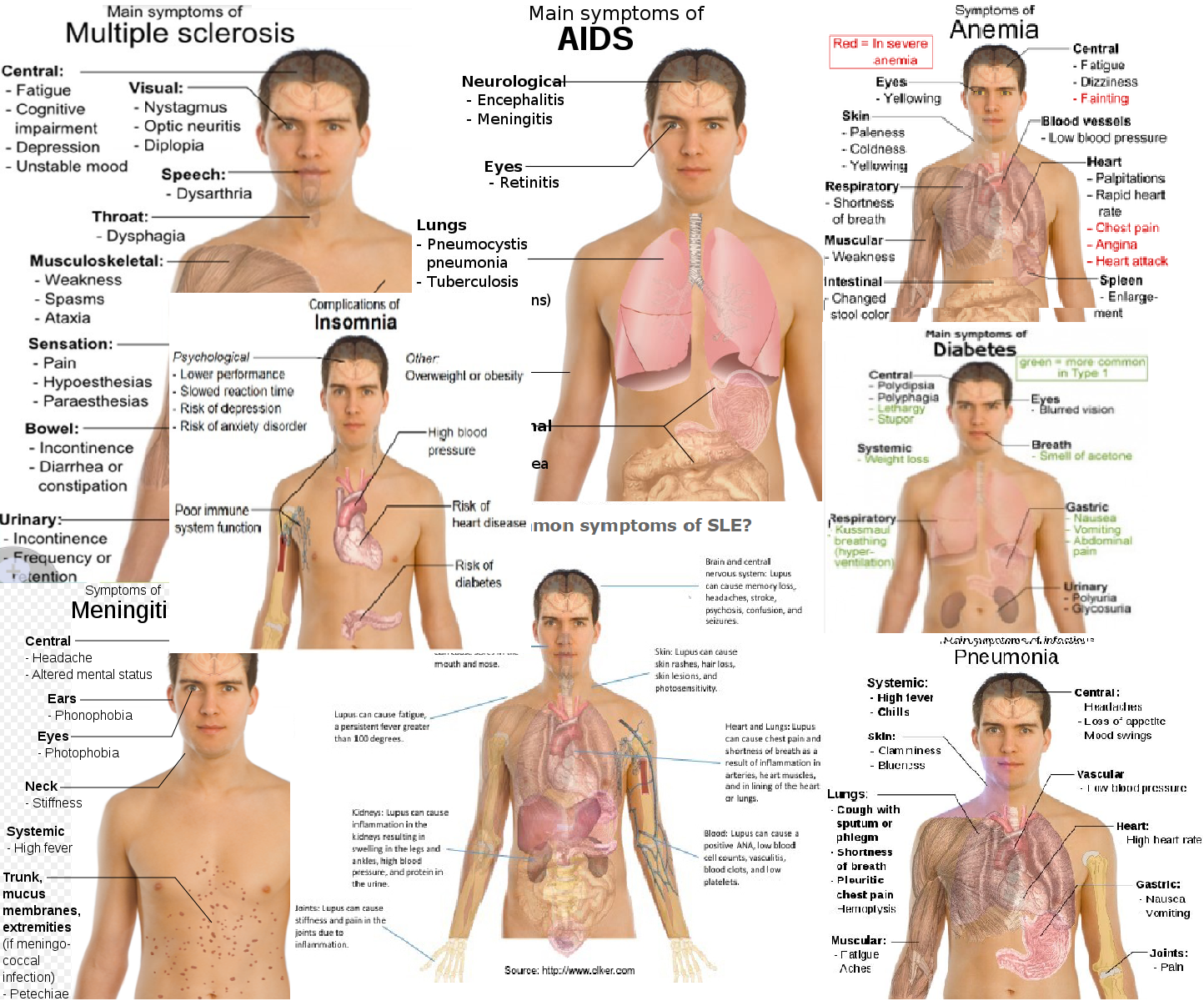
Everyman
If you're a nursing student, you've probably seen this guy before. Let's call him Everyman. (You may know Jenny, the 22-year-old nursing student, too. Poor Jenny.)
Seriously though, poor Everyman has Everything, and this isn't even a comprehensive sampling. (How are COPD and heart failure not on the list?)
 Results of a brief Google Image search
Results of a brief Google Image search
If you're an English major, you probably know that Everyman is a 15th century morality play, author unkown, and loads of fun (by fun, we mean moralizing).
At the beginning of the play, God tells Death to go tell Everyman that God's about to pull the plug on him. Death tells him just that, and reminds him by the way to not forget his account book (of good and bad deeds). Everyman begs for more time, and for a companion to "go" with him (what is this, ancient Egypt?) Death says sure, if you can find someone brave enough to die with you.
Fellowship, a new character, runs for his life, literally, when Everyman asks him to accompany him into death (perfectly normal response). So do Kindred, Cousin, and Goods (as in material goods, which they specifically point out is the opposite of love of God).
Good Deeds, who is obviously very nice, wants to go with Everyman, but she is too weak. Her sister, Knowledge, says if Everyman goes to confession and shows penance it will help. Everyman does, then scourges (uses a terrifying medieval whip on) himself, which magically makes Good Deeds strong enough to walk, no Physical Therapy required. Other friends join and then abandon Everyman on his journey to his grave: Discretion, Strength, Beauty, etc.
As Everyman disappears into his grave with Good Deeds, a doctor appears to give a diagnosis/pronounce time of death, I mean, give the epilogue. He tells the audience to forsake Pride, Beauty, Strength, and so on, because they forsake every man (and woman and child and everyone in the gray area in between--abandonment knows not gender or age) in the end.
We get the message. We don't take anything with us, not our worldly possessions, not our strength, beauty, knowledge, even, though hopefully our families will be with us until the very end. And a nurse.
If I'm for sure imminently on my way out, I want an LVN or RN, maybe a CNA, too (if one can be spared) at bedside, not an MD. I want bedside reports, pain assessment and reassessment, all the morphine, all the Ativan, and none of the heroic measures down my throat or crushing my ribs (advanced directive alert).
Life is suffering enough.
Seriously though, poor Everyman has Everything, and this isn't even a comprehensive sampling. (How are COPD and heart failure not on the list?)
 Results of a brief Google Image search
Results of a brief Google Image searchIf you're an English major, you probably know that Everyman is a 15th century morality play, author unkown, and loads of fun (by fun, we mean moralizing).
At the beginning of the play, God tells Death to go tell Everyman that God's about to pull the plug on him. Death tells him just that, and reminds him by the way to not forget his account book (of good and bad deeds). Everyman begs for more time, and for a companion to "go" with him (what is this, ancient Egypt?) Death says sure, if you can find someone brave enough to die with you.
Fellowship, a new character, runs for his life, literally, when Everyman asks him to accompany him into death (perfectly normal response). So do Kindred, Cousin, and Goods (as in material goods, which they specifically point out is the opposite of love of God).
Good Deeds, who is obviously very nice, wants to go with Everyman, but she is too weak. Her sister, Knowledge, says if Everyman goes to confession and shows penance it will help. Everyman does, then scourges (uses a terrifying medieval whip on) himself, which magically makes Good Deeds strong enough to walk, no Physical Therapy required. Other friends join and then abandon Everyman on his journey to his grave: Discretion, Strength, Beauty, etc.
As Everyman disappears into his grave with Good Deeds, a doctor appears to give a diagnosis/pronounce time of death, I mean, give the epilogue. He tells the audience to forsake Pride, Beauty, Strength, and so on, because they forsake every man (and woman and child and everyone in the gray area in between--abandonment knows not gender or age) in the end.
We get the message. We don't take anything with us, not our worldly possessions, not our strength, beauty, knowledge, even, though hopefully our families will be with us until the very end. And a nurse.
If I'm for sure imminently on my way out, I want an LVN or RN, maybe a CNA, too (if one can be spared) at bedside, not an MD. I want bedside reports, pain assessment and reassessment, all the morphine, all the Ativan, and none of the heroic measures down my throat or crushing my ribs (advanced directive alert).
Life is suffering enough.
October 8, 2019
Babel
Babel is a biblical tower, a metaphor for breakdowns in communication, a javascript compiler, and a 2006 movie starring Cate Blanchett and Brad Pitt.
Several cultures, from Christian, Sumarian to African, tell legends from the past of hubris (excessive human pride) involving tower-building, perhaps a symbol of how ambitious humans believe we can build and build until we've conquered the earth as well as the sky.

Humans have built skyscrapers, dams, entire islands and spacecraft. Our hubris has extended as far as outer space, and stretched thin our energy and planetary resources.
Sometimes we may wonder, how long can all of this possibly last? We do not have to wait for divine intervention to strike us with a myriad of new, foreign tongues or even for the sun to devour the earth in its red giant flames...we will run out of some thing or other first--clean air, water, energy, possibly peace and good will.
The 2006 psychological thriller, Babel, set in Morroco, United States, Mexico, and Japan, highlights how people fall short and fail to communicate, with heartbreaking results. Each culture, whether deaf, American, Morrocan, Mexican, or Japanese, is portrayed with empathy, depicting the characters' good intentions, innocence, and unfortunately, fear. Mistrust leads to fear and animosity until that classic cinematic moment where everything in the intersecting plot-lines goes to hell. The lesson here is absolutely applicable to real life: that misunderstandings and lack of trust can lead to the worst possible outcomes, which better communication may have prevented.
In a healthcare setting, lack of communication and miscommunication can lead to death. Whether it's a critical lab result, listening to a patient's concerns, assessing and reporting changes in condition, or making sure all the different specialists collaborate on the plans of care, communication is critical. It is as important as ever even as brain death occurs, because here come difficult decisions to make, delicate news to share, and all the stages of grief at once.
Yet we speak in different languages, and even in the same language, with different styles and nonverbal expressions. Assessment, asking someone their needs and preferences, is key, but also more easily said than done, because trust takes time to build, as do communication skills. A lifetime, it seems.
Several cultures, from Christian, Sumarian to African, tell legends from the past of hubris (excessive human pride) involving tower-building, perhaps a symbol of how ambitious humans believe we can build and build until we've conquered the earth as well as the sky.

Humans have built skyscrapers, dams, entire islands and spacecraft. Our hubris has extended as far as outer space, and stretched thin our energy and planetary resources.
Sometimes we may wonder, how long can all of this possibly last? We do not have to wait for divine intervention to strike us with a myriad of new, foreign tongues or even for the sun to devour the earth in its red giant flames...we will run out of some thing or other first--clean air, water, energy, possibly peace and good will.
The 2006 psychological thriller, Babel, set in Morroco, United States, Mexico, and Japan, highlights how people fall short and fail to communicate, with heartbreaking results. Each culture, whether deaf, American, Morrocan, Mexican, or Japanese, is portrayed with empathy, depicting the characters' good intentions, innocence, and unfortunately, fear. Mistrust leads to fear and animosity until that classic cinematic moment where everything in the intersecting plot-lines goes to hell. The lesson here is absolutely applicable to real life: that misunderstandings and lack of trust can lead to the worst possible outcomes, which better communication may have prevented.
In a healthcare setting, lack of communication and miscommunication can lead to death. Whether it's a critical lab result, listening to a patient's concerns, assessing and reporting changes in condition, or making sure all the different specialists collaborate on the plans of care, communication is critical. It is as important as ever even as brain death occurs, because here come difficult decisions to make, delicate news to share, and all the stages of grief at once.
Yet we speak in different languages, and even in the same language, with different styles and nonverbal expressions. Assessment, asking someone their needs and preferences, is key, but also more easily said than done, because trust takes time to build, as do communication skills. A lifetime, it seems.
September 27, 2019
ERAS = Enhanced Recovery After Surgery
After my C section in 2012, I experienced some but not all of the "enhanced recovery after surgery" recommendations at the hospital.
1. Nursing care
Daily CHG Bath: sponge bath with antibacterial wipes--thank goodness they didn't do this to me--it's probably a new guideline to kill germs and make people cold.
Incentive Spirometer: never saw one of these suckers until nursing school, where I also learned I'm supposed to suck air in through it, not blow, to make the blue thingy go up.

Incentive Spirometer, use 10 times /hr
Day 0 take out nasogastric tube: didn't have one
Day 1 take out urinary catheter: I was so sad when they took mine out, because not only did I have to get out of bed now, I was pretty sure my bladder didn't work anymore since it hardly worked during pregnancy.
2. IV
Saline lock IV when tolerating clear liquids: I have zero recollection of what was going on with my IV.
3. Pain Management
Day 0 IV/epidural if needed: I had a morphine pump initially, but they took that away and threatened a cardiology consult because my heart rate was in the 40s (normal is 60-100).
Day 1 IV and oral meds: I was in so much pain I was in spasms and crying. IV toradol helped--still remember how it felt going in--cold, pain-relieving.
After Day 2 oral pain meds only: House, MD is a liar becuase Vicodin barely took the edge off and made me nauseous but Vicodin and Motrin were all I could get from the pharmacy for home, even though my uneven C-section scar was oozing grape jelly and hurting (not as much as my spirit, which was gone).
4. Post-op nutrition
Day 0 gum, ice chips, water: after the surgery even though I was parched they would not give me water, only ice chips, which if anyone knows about Chinese medicine, is literally the worst thing you can give someone who is weak from just being cut open, giving birth, etc. Kill all my chi, why don't you.
Day 1 full liquid diet, no carbonated drink / Day 2 soft, chopped diet / Day 3 regular diet: they advanced me pretty fast since I wasn't choking on food.
5. Early mobilization
Day 0 walk at least 150 ft: when they took out my catheter I was forced to walk my broken body to the bathroom, which I kept to a minimum, definitely <150 feet.
Day 1 walk at least 300 ft (a little more than one lap around the floor): I was in a ton of pain, and when asked to go walk around the hallway for my own good (mobility is medicine, lol), I said, "No."
Day 2 walk at least 500 ft (2 laps): still no. I was barely 30 and probably not going to get a blood clot, nauseous, in pain, and didn't feel like leaving the baby alone in the room (plus she was pretty much on me continuously).
However hard people say nursing is, I don't believe it's harder than being the patient, especially if the patient has to "work through the pain" after an ortho proecdure or feed and take care of a newborn (again, what's up with that?)
1. Nursing care
Daily CHG Bath: sponge bath with antibacterial wipes--thank goodness they didn't do this to me--it's probably a new guideline to kill germs and make people cold.
Incentive Spirometer: never saw one of these suckers until nursing school, where I also learned I'm supposed to suck air in through it, not blow, to make the blue thingy go up.
Incentive Spirometer, use 10 times /hr
Day 0 take out nasogastric tube: didn't have one
Day 1 take out urinary catheter: I was so sad when they took mine out, because not only did I have to get out of bed now, I was pretty sure my bladder didn't work anymore since it hardly worked during pregnancy.
2. IV
Saline lock IV when tolerating clear liquids: I have zero recollection of what was going on with my IV.
3. Pain Management
Day 0 IV/epidural if needed: I had a morphine pump initially, but they took that away and threatened a cardiology consult because my heart rate was in the 40s (normal is 60-100).
Day 1 IV and oral meds: I was in so much pain I was in spasms and crying. IV toradol helped--still remember how it felt going in--cold, pain-relieving.
After Day 2 oral pain meds only: House, MD is a liar becuase Vicodin barely took the edge off and made me nauseous but Vicodin and Motrin were all I could get from the pharmacy for home, even though my uneven C-section scar was oozing grape jelly and hurting (not as much as my spirit, which was gone).
4. Post-op nutrition
Day 0 gum, ice chips, water: after the surgery even though I was parched they would not give me water, only ice chips, which if anyone knows about Chinese medicine, is literally the worst thing you can give someone who is weak from just being cut open, giving birth, etc. Kill all my chi, why don't you.
Day 1 full liquid diet, no carbonated drink / Day 2 soft, chopped diet / Day 3 regular diet: they advanced me pretty fast since I wasn't choking on food.
5. Early mobilization
Day 0 walk at least 150 ft: when they took out my catheter I was forced to walk my broken body to the bathroom, which I kept to a minimum, definitely <150 feet.
Day 1 walk at least 300 ft (a little more than one lap around the floor): I was in a ton of pain, and when asked to go walk around the hallway for my own good (mobility is medicine, lol), I said, "No."
Day 2 walk at least 500 ft (2 laps): still no. I was barely 30 and probably not going to get a blood clot, nauseous, in pain, and didn't feel like leaving the baby alone in the room (plus she was pretty much on me continuously).
However hard people say nursing is, I don't believe it's harder than being the patient, especially if the patient has to "work through the pain" after an ortho proecdure or feed and take care of a newborn (again, what's up with that?)
September 5, 2019
OS = Oculus Sinister
Which of your eyes is evil? In Latin, oculus sinister (OS), the left one.
Incidentally, the right eye, oculus dexter (OD), does have a television series about a serial killer named after it.
According to Rachel Spector, author of Cultural Diversity in Health and Illness, the evil eye is one of the oldest and most widespread cultural beliefs in the world.
The evil eye may strike a victim from the eye or mouth, bringing about mysterious illness or misfortune. In different parts of the world, beliefs around the source of the evil eye vary--strangers in Mexico, kinfolk in Iran, witches in Greece, the devil in the Mediterranean, a diety in the Near East, a "low grade phenomenon" among Slovak Americans (Spector, 2017, p.79).
The injury, illness or misfortune caused by an evil eye may be prevented or cured with rituals, symbols, and talismans such as the ones below.

In western medicine, we study stress and its effects on the immune system, viruses, bacteria, carcinogens and other pathogens. Perhaps the agents of the evil eye (envy, hate, jealousy) described in folklore are not so different from invisible microbes that one becomes more susceptible to when subjected to stress (if people around one envies or hates one and it shows). Stress lowers the ability of the immune system to fight off invaders and proofread errors or silencing in DNA replication/transcription (that may lead to cancer).
These agents of "evil" may be tangible or intangible. People colonized or sick with pathogens may "strike" one by sneezing and coughing on one or touching the same surfaces or objects. Stress, excessive anxiety, and lack of support can affect one's work performance, leading to additional stress and decreased immunity in a vicious cycle.
So, what to do?
Avoid: set boundaries, reduce/resolve conflicts and negativity
Alter: apply feedback, improve, compromise
Adapt: be flexible, positive, openminded, look at the big picture
Accept: forgive, understand, let go
It's not much, but one can't walk around wearing protective gowns, masks and gloves, covered with a hundred dangling blue-eyed talismans all day.
Reference:
Spector, Rachel E., Cultural Diversity in Health and Illness (2017), 9th ed. Boston, MA: Pearson.
Incidentally, the right eye, oculus dexter (OD), does have a television series about a serial killer named after it.
According to Rachel Spector, author of Cultural Diversity in Health and Illness, the evil eye is one of the oldest and most widespread cultural beliefs in the world.
The evil eye may strike a victim from the eye or mouth, bringing about mysterious illness or misfortune. In different parts of the world, beliefs around the source of the evil eye vary--strangers in Mexico, kinfolk in Iran, witches in Greece, the devil in the Mediterranean, a diety in the Near East, a "low grade phenomenon" among Slovak Americans (Spector, 2017, p.79).
The injury, illness or misfortune caused by an evil eye may be prevented or cured with rituals, symbols, and talismans such as the ones below.

In western medicine, we study stress and its effects on the immune system, viruses, bacteria, carcinogens and other pathogens. Perhaps the agents of the evil eye (envy, hate, jealousy) described in folklore are not so different from invisible microbes that one becomes more susceptible to when subjected to stress (if people around one envies or hates one and it shows). Stress lowers the ability of the immune system to fight off invaders and proofread errors or silencing in DNA replication/transcription (that may lead to cancer).
These agents of "evil" may be tangible or intangible. People colonized or sick with pathogens may "strike" one by sneezing and coughing on one or touching the same surfaces or objects. Stress, excessive anxiety, and lack of support can affect one's work performance, leading to additional stress and decreased immunity in a vicious cycle.
So, what to do?
Avoid: set boundaries, reduce/resolve conflicts and negativity
Alter: apply feedback, improve, compromise
Adapt: be flexible, positive, openminded, look at the big picture
Accept: forgive, understand, let go
It's not much, but one can't walk around wearing protective gowns, masks and gloves, covered with a hundred dangling blue-eyed talismans all day.
Reference:
Spector, Rachel E., Cultural Diversity in Health and Illness (2017), 9th ed. Boston, MA: Pearson.
August 26, 2019
Three Styles of Nursing Interviews
People have been asking, so here are some archetypal nursing interviews that a new grad might experience. There's always some overlap, especially for practical questions, but there are definitely distinct styles. Writing about II. nearly gave me full body hives just thinking about it again.
I. The Practical Interview
· Are you willing to work evening shifts? overnight shifts?
· If the next nurse does not show, you understand that it's patient abandonment if you leave and you will have to stay on to work a second shift unless or until coverage is obtained. You cool with that?
· Do you prefer to work full time? Part time? On call? How flexible is your schedule?
· Are you open to working holidays, weekends, extra shifts as needed?
· What are your long term goals, career wise?
· If a sister facility is short personnel, are you willing to drive there to fill in on short notice?
· Are you willing to relocate?
· Any questions for us?
II. The Grill
(First of all, it's a panel interview, of course, like the MLA*.)
 Panel interview. Photo courtesy: www.workitdaily.com
Panel interview. Photo courtesy: www.workitdaily.com
· National Patient Safety Goals, go. Yes, all of them. You're still missing one or two.
· Patient A is coding, patient B is in anaphylactic shock, patient C is asking for you urgently on the phone, and patient D is nonresponsive. Explain your order of priority, what you would do for each patient, and your rationale for each.
· What would you teach the patient about these medications?
· A patient is having issues getting an appointment with a specialist. What do you do?
· What is your role as a nurse in a pre-operative setting? What are your responsibilities and scope of practice?
· How would you serve the pediatric population as a nurse?
· How would you support women's health as a nurse?
· What experience have you had with telephone triage?
· What experience have you had with rapid deterioration of a patient?
· This really f-ed up and bizarre thing happened with a patient. What do you do?
· What do you teach a patient who has had a fracture?
· What do you do if a patient is noncompliant?
· How do you respond if your supervisor criticizes you in front of a patient?
· Why should we hire you?
· Any questions for us? :)
III. The Behavioral Interview
· Tell us a little about yourself.
· Describe a time when you felt challenged.
· Describe a time when you worked on a team.
· Describe a time when you made an unpopular decision.
· Describe a time when you faced a conflict. How did you resolve it, if you did?
· Describe a time when you did or did not meet a client's expectations. What happened, specifically?
· Do you have any questions for us?
*Modern Language Association--the conference where English majors interview for academic positions.
I. The Practical Interview
· Are you willing to work evening shifts? overnight shifts?
· If the next nurse does not show, you understand that it's patient abandonment if you leave and you will have to stay on to work a second shift unless or until coverage is obtained. You cool with that?
· Do you prefer to work full time? Part time? On call? How flexible is your schedule?
· Are you open to working holidays, weekends, extra shifts as needed?
· What are your long term goals, career wise?
· If a sister facility is short personnel, are you willing to drive there to fill in on short notice?
· Are you willing to relocate?
· Any questions for us?
II. The Grill
(First of all, it's a panel interview, of course, like the MLA*.)
 Panel interview. Photo courtesy: www.workitdaily.com
Panel interview. Photo courtesy: www.workitdaily.com· National Patient Safety Goals, go. Yes, all of them. You're still missing one or two.
· Patient A is coding, patient B is in anaphylactic shock, patient C is asking for you urgently on the phone, and patient D is nonresponsive. Explain your order of priority, what you would do for each patient, and your rationale for each.
· What would you teach the patient about these medications?
· A patient is having issues getting an appointment with a specialist. What do you do?
· What is your role as a nurse in a pre-operative setting? What are your responsibilities and scope of practice?
· How would you serve the pediatric population as a nurse?
· How would you support women's health as a nurse?
· What experience have you had with telephone triage?
· What experience have you had with rapid deterioration of a patient?
· This really f-ed up and bizarre thing happened with a patient. What do you do?
· What do you teach a patient who has had a fracture?
· What do you do if a patient is noncompliant?
· How do you respond if your supervisor criticizes you in front of a patient?
· Why should we hire you?
· Any questions for us? :)
III. The Behavioral Interview
· Tell us a little about yourself.
· Describe a time when you felt challenged.
· Describe a time when you worked on a team.
· Describe a time when you made an unpopular decision.
· Describe a time when you faced a conflict. How did you resolve it, if you did?
· Describe a time when you did or did not meet a client's expectations. What happened, specifically?
· Do you have any questions for us?
*Modern Language Association--the conference where English majors interview for academic positions.
Three Types of Nursing Interviews
People have been asking, so here are some archetypal nursing interviews. There's always some overlap, especially for practical questions, but there are definitely distinct styles. Writing about II. nearly gave me full body hives just thinking about it again.
I. The Practical Interview
· Are you willing to work evening shifts? overnight shifts?
· If the next nurse does not show, you understand that it's patient abandonment if you leave and you will have to stay on to work a second shift unless or until coverage is obtained. You cool with that?
· Do you prefer to work full time? Part time? On call? How flexible is your schedule?
· Are you open to working holidays, weekends, extra shifts as needed?
· What are your long term goals, career wise?
· If a sister facility is short personnel, are you willing to drive there to fill in on short notice?
· Are you willing to relocate?
· Any questions for us?
II. The Grill
(First of all, it's a panel interview, of course, like the MLA*.)
Panel interview. Photo courtesy: www.workitdaily.com
· National Patient Safety Goals, go. Yes, all of them. You're still missing one or two.
· Patient A is coding, patient B is in anaphylactic shock, patient C is asking for you urgently on the phone, and patient D is nonresponsive. Explain your order of priority, what you would do for each patient, and your rationale for each.
· What would you teach the patient about these medications?
· A patient is having issues getting an appointment with a specialist. What do you do?
· What is your role as a nurse in a pre-operative setting? What are your responsibilities and scope of practice?
· How would you serve the pediatric population as a nurse?
· How would you support women's health as a nurse?
· What experience have you had with telephone triage?
· What experience have you had with rapid deterioration of a patient?
· This really f-ed up and bizarre thing happened with a patient. What do you do?
· What do you teach a patient who has had a fracture?
· What do you do if a patient is noncompliant?
· How do you respond if your supervisor criticizes you in front of a patient?
· Why should we hire you?
· Any questions for us? :)
III. The Behavioral Interview
· Tell us a little about yourself.
· Describe a time when you felt challenged.
· Describe a time when you worked on a team.
· Describe a time when you made an unpopular decision.
· Describe a time when you faced a conflict. How did you resolve it, if you did?
· Describe a time when you did or did not meet a client's expectations. What happened, specifically?
· Do you have any questions for us?
*Modern Language Association--the conference where English majors interview for academic positions.
I. The Practical Interview
· Are you willing to work evening shifts? overnight shifts?
· If the next nurse does not show, you understand that it's patient abandonment if you leave and you will have to stay on to work a second shift unless or until coverage is obtained. You cool with that?
· Do you prefer to work full time? Part time? On call? How flexible is your schedule?
· Are you open to working holidays, weekends, extra shifts as needed?
· What are your long term goals, career wise?
· If a sister facility is short personnel, are you willing to drive there to fill in on short notice?
· Are you willing to relocate?
· Any questions for us?
II. The Grill
(First of all, it's a panel interview, of course, like the MLA*.)
Panel interview. Photo courtesy: www.workitdaily.com· National Patient Safety Goals, go. Yes, all of them. You're still missing one or two.
· Patient A is coding, patient B is in anaphylactic shock, patient C is asking for you urgently on the phone, and patient D is nonresponsive. Explain your order of priority, what you would do for each patient, and your rationale for each.
· What would you teach the patient about these medications?
· A patient is having issues getting an appointment with a specialist. What do you do?
· What is your role as a nurse in a pre-operative setting? What are your responsibilities and scope of practice?
· How would you serve the pediatric population as a nurse?
· How would you support women's health as a nurse?
· What experience have you had with telephone triage?
· What experience have you had with rapid deterioration of a patient?
· This really f-ed up and bizarre thing happened with a patient. What do you do?
· What do you teach a patient who has had a fracture?
· What do you do if a patient is noncompliant?
· How do you respond if your supervisor criticizes you in front of a patient?
· Why should we hire you?
· Any questions for us? :)
III. The Behavioral Interview
· Tell us a little about yourself.
· Describe a time when you felt challenged.
· Describe a time when you worked on a team.
· Describe a time when you made an unpopular decision.
· Describe a time when you faced a conflict. How did you resolve it, if you did?
· Describe a time when you did or did not meet a client's expectations. What happened, specifically?
· Do you have any questions for us?
*Modern Language Association--the conference where English majors interview for academic positions.
August 16, 2019
Metaphorsis = Metaphor/Metamorphosis
Thank you to The Laurel Review for selecting my (prose) poetry chapbook, Metaphorsis, as the winner of the Midwest Chapbook Contest, to be published by Greentower Press in 2020.
This project I actually did write during nursing school, while thinking about nursing theory, life changes, pain, and the metamorphosis of insects. Also, thank you so much, Dr. Lytle, for the entomological consult.
In a way, the manuscript was a precursor to our RN graduation speech about going from useless eggs and pathetic, wormy caterpillars to brand new butterflies. It's not all Kafka's The Metamorphosis, but we humans undergo metamorphosis metaphorically, through growth, life events, chance encounters, and seasons of life.
Since I never submitted parts of this project to journals, here're some free excerpts:
1. A microcosmic metaphor for the tenderness and terror of human longing and loss: the life cycle of an arthropod.*
We are always molting, shedding old cells, every few days a new stomach lining, each week new lung alveoli, new liver hepatocytes yearly, seven years almost the entire body renewed.
Growth, and loss, are constants.
2.
To molt: to shed old feathers, skin, hair, or shell, to make way for new growth.
To molt = pain & vulnerability.
Instar: a phase between two periods of molting.
With each instar, something is lost. Innocence, trust, the intangible and tangible. Beloved pets, loveys, grandparents, best friends, childhood.
[...]
10.
The imago is an adult insect, bright-eyed, emerald-winged. The imaginal stage: the stage in which an insect attains maturity.
The imago is also the image of one’s parents, in the best and worst ways.
Attachment theory, disciplinarian/authoritarian/let-them-eat-grass, love languages, refrigerator for mom—what reenactment of your childhood (damage) do you crave? Did your parents infantilize you? Ignore you? Congratulations, you will be attracted to just that, completely subconsciously and in a way out of your control, when it comes to friendships and partners. Whatever private prison your childhood (and the adults in it) imposed on you, remains part of you, your imago, even as you become a full-grown imago.
Is this the inescapable karma that makes us relive life cycles, patterns and relationships? Is it possible to achieve nirvana?
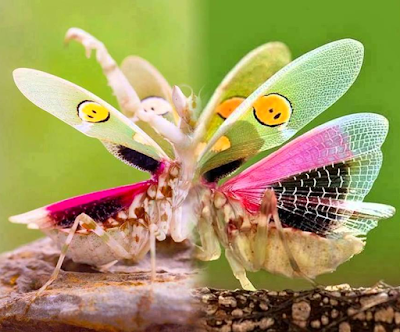 A robust, young, praying mantis, deprived of food, can eat every last one of its siblings.
A robust, young, praying mantis, deprived of food, can eat every last one of its siblings.
*An arthropod is an animal with no spinal column but has an exoskeleton, a body in sections, and paired, jointed appendages.
This project I actually did write during nursing school, while thinking about nursing theory, life changes, pain, and the metamorphosis of insects. Also, thank you so much, Dr. Lytle, for the entomological consult.
In a way, the manuscript was a precursor to our RN graduation speech about going from useless eggs and pathetic, wormy caterpillars to brand new butterflies. It's not all Kafka's The Metamorphosis, but we humans undergo metamorphosis metaphorically, through growth, life events, chance encounters, and seasons of life.
Since I never submitted parts of this project to journals, here're some free excerpts:
1. A microcosmic metaphor for the tenderness and terror of human longing and loss: the life cycle of an arthropod.*
We are always molting, shedding old cells, every few days a new stomach lining, each week new lung alveoli, new liver hepatocytes yearly, seven years almost the entire body renewed.
Growth, and loss, are constants.
2.
To molt: to shed old feathers, skin, hair, or shell, to make way for new growth.
To molt = pain & vulnerability.
Instar: a phase between two periods of molting.
With each instar, something is lost. Innocence, trust, the intangible and tangible. Beloved pets, loveys, grandparents, best friends, childhood.
[...]
10.
The imago is an adult insect, bright-eyed, emerald-winged. The imaginal stage: the stage in which an insect attains maturity.
The imago is also the image of one’s parents, in the best and worst ways.
Attachment theory, disciplinarian/authoritarian/let-them-eat-grass, love languages, refrigerator for mom—what reenactment of your childhood (damage) do you crave? Did your parents infantilize you? Ignore you? Congratulations, you will be attracted to just that, completely subconsciously and in a way out of your control, when it comes to friendships and partners. Whatever private prison your childhood (and the adults in it) imposed on you, remains part of you, your imago, even as you become a full-grown imago.
Is this the inescapable karma that makes us relive life cycles, patterns and relationships? Is it possible to achieve nirvana?
 A robust, young, praying mantis, deprived of food, can eat every last one of its siblings.
A robust, young, praying mantis, deprived of food, can eat every last one of its siblings.
*An arthropod is an animal with no spinal column but has an exoskeleton, a body in sections, and paired, jointed appendages.
August 7, 2019
Merced = Mercy
It's been a weird couple of months of job searching.
I saved myself for my first choice (Mercy*, of course) all the way until 4th of July when I lost my mind and applied to all the things. Then all the interviews came at once, including Mercy's. I was tempted by one 8-5 job (you can be a nurse, make a difference, AND drop off and pick up your kid!), and left another place before finishing my orientation shifts.
It's like dating half-heartedly and browsing Tinder (I mean Indeed) when you KNOW who you want but you don't know if they are interested in a second date but maybe you'll save yourself for them and turn down everyone else just in case one day they look your way...
So you leave town with your kid to visit family and finally meet your dad's secret girlfriend who turns out to be a Trump supporter, shootings happen all over America, and you think the end is near, all hope is nigh. Then a call arrives from HR pointing you to an email in your inbox, and you nearly go blind from all the celebration stickers your mind superimposes onto the visual field.
Hopefully the background check goes okay, because not sure if I can magic up a English language Taiwanese high school transcript from 20 years ago, or a W2 from a defunct Taiwanese magazine I wrote a column for in Chinese. I've only gotten chest X-rays to prove I don't have active TB once a year for the past three years (Thanks, Taiwan, for the fish and BCG vaccine) and I can reach my toes (was asked to do that, oddly, at my last physical).
A brief comparison of the difficulty level of life events that are actually dating or have been likened to dating (simile! not metaphor!) in recent conversations seems to go in this descending order, from, "Is this even possible?" to, "No prob":
Getting a literary agent > Dating someone and it works out--for life > Having and caring for a baby/young child > Getting a job at your dream hospital > Nursing school > Getting published > Getting into a nursing program > Getting any job > Getting any date.
With time and patience, may all my classmates (and anyone else on a search) get their dream jobs as well! Dating's overrated; employment is not.
And thank you, everyone, for all of your support and for being there through this journey!
*Merced, incidentally, means Mercy in Spanish. It works.
I saved myself for my first choice (Mercy*, of course) all the way until 4th of July when I lost my mind and applied to all the things. Then all the interviews came at once, including Mercy's. I was tempted by one 8-5 job (you can be a nurse, make a difference, AND drop off and pick up your kid!), and left another place before finishing my orientation shifts.
It's like dating half-heartedly and browsing Tinder (I mean Indeed) when you KNOW who you want but you don't know if they are interested in a second date but maybe you'll save yourself for them and turn down everyone else just in case one day they look your way...
So you leave town with your kid to visit family and finally meet your dad's secret girlfriend who turns out to be a Trump supporter, shootings happen all over America, and you think the end is near, all hope is nigh. Then a call arrives from HR pointing you to an email in your inbox, and you nearly go blind from all the celebration stickers your mind superimposes onto the visual field.

Hopefully the background check goes okay, because not sure if I can magic up a English language Taiwanese high school transcript from 20 years ago, or a W2 from a defunct Taiwanese magazine I wrote a column for in Chinese. I've only gotten chest X-rays to prove I don't have active TB once a year for the past three years (Thanks, Taiwan, for the fish and BCG vaccine) and I can reach my toes (was asked to do that, oddly, at my last physical).
A brief comparison of the difficulty level of life events that are actually dating or have been likened to dating (simile! not metaphor!) in recent conversations seems to go in this descending order, from, "Is this even possible?" to, "No prob":
Getting a literary agent > Dating someone and it works out--for life > Having and caring for a baby/young child > Getting a job at your dream hospital > Nursing school > Getting published > Getting into a nursing program > Getting any job > Getting any date.
With time and patience, may all my classmates (and anyone else on a search) get their dream jobs as well! Dating's overrated; employment is not.
And thank you, everyone, for all of your support and for being there through this journey!
*Merced, incidentally, means Mercy in Spanish. It works.


