
Nicola Griffith's Blog, page 35
December 18, 2021
Omicron—some new data
Photo by Fusion Medical Animation on Unsplash
Two recent studies confirm that the Omicron variant of SARS-CoV-2 is very bad new in terms of infectiousness, ability to evade immunity, and resistance to existing therapies. In addition, although preliminary reports from South Africa suggested that infection with the Omicron variant could result in less severe illness than infection with the Delta variant, the UK data hints that there’s no significant difference in severity between the two (though the study is quick to list its caveats).
What follows is a look at those studies. But if you’re in a rush just skip to the summary and conclusions.
THE STUDIESUniversity Collage LondonNeil Ferguson, Azra Ghani, Anne Cori et al. Growth, population distribution and immune escape of the Omicron in England. Imperial College London (16-12-2021). Doi: https://doi.org/10.25561/93038
https://www.imperial.ac.uk/media/imperial-college/medicine/mrc-gida/2021-12-16-COVID19-Report-49.pdf
This study looked at over 21,000 cases of infection with the Omicron SARS-CoV-2 variant vs over 350,00 cases of infection with the Delta variant, and they controlled for vaccine status, age (in 10-yr age bands), sex, ethnicity, asymptomatic status, region and specimen date.
They suggest that the Omicron case rate is doubling every two days, with caveats:
“A total of 208,971 S+ and 15,063 S- cases with complete data were included in the SGTF analysis, and 142,340 Delta and 6,184 Omicron cases were included in the genotype analysis. Both analyses suggest rapid growth of the log odds frequency of the Omicron variant relative to Delta, with exponential growth rate estimates of 0.45/day (95%CI: 0.44-0.46) [1.5 day doubling time] and 0.43/day (95%CI: 0.42-0.44) [1.6 day doubling time] obtained from genotype and SGTF data, respectively. Given the frequency of Omicron exceeded 20% by the last time point examined, the exponential growth rate of frequency (as compared with log odds frequency) was estimated to be somewhat lower, at 0.34/day (95% CI: 0.33-0.35) [2.0 day doubling time] from both SGTF and genotype data, calculated using Poisson rather than logistic regression.”
I’m pretty sure this variant is doubling at least every two days. Recent wastewater data here in WA state—and this was 2 days ago—show 40% of virus is Omicron variant. Given doubling rate, I’d be shocked if today it were not easily the dominant strain—it’s just that the testing data hasn’t shown up yet.
They found that “Omicron was associated with a 5.41 (95% CI: 4.87-6.00) fold higher relative risk of reinfection compared with Delta.” And that, prior to Omicron, a cohort study of UK healthcare workers “estimated that SARS-CoV-2 infection gave 85% protection against reinfection over 6 months, or a relative risk of infection of 0.15 compared with those with no prior infection. Our hazard ratio estimate would suggest the relative risk of reinfection has risen to 0.81 [95%CI: 0.73-1.00] (i.e. remaining protection of 19% [95%CI: 0-27%]) against Omicron.” Also that their “estimates largely agree with those from UKHSA’s TNCC study and predictions from predicting VE from neutralising antibody titres (4,14), suggesting very limited remaining protection against symptomatic infection afforded by two doses of AZ, low protection afforded by two doses of Pfizer, but moderate to high (55-80%) protection in people boosted with an mRNA vaccine.”
In other words, a 2-dose vaccination regimen offered 19% protection against severe illness; prior infection offered 20% protection; but a two-dose vaccination followed by an mRNA booster gave at least 55% protection and perhaps as much as 80%. And here they’re talking about AstraZeneca and Pfizer; Moderna has been shown to more effective than either. This is relatively good news.
The bad news is that they “find no evidence (for both risk of hospitalisation attendance and symptom status) of Omicron having different severity from Delta,” though, as they point out, “data on hospitalisations are still very limited.” In other words, it’s early days yet. We’ll just have to keep waiting.
bioRxiv.orgLihong Liu, Sho Iketani, Yicheng Guo et al. Striking Antibody Evasion Manifested by the Omicron Variant of SARS-CoV-2. Doi: https://doi.org/10.1101/2021.12.14.472719
https://www.biorxiv.org/content/10.1101/2021.12.14.472719v2
This study, posted on bioRxiv.org, largely agrees with everything ICL study suggests about lowered immunity but go into detail on the efficacy of monoclonal antibodies. With previous variants, when administered as early as possible after infection, monoclonal antibodies can stop many people from developing severe Covid. But the new study suggests that all of the therapies currently in use and most in development are much less effective against omicron, if they work at all.
In neutralisation studies with monoclonal antibodies, only one (Brii198 — which is a combination of amubarvimab and romlusevimab) maintained notable activity against omicron. However an update yesterday suggests that sotrovimab (Xevudy) still works (though, again, monoclonal antibodies not only have to be administered in a certain timeframe, their effects are, at best, modest).
The alarming thing noted by teh study was that there’s one small subset of Omicron that evades monoclonal antibodies completely—all of them: “Neutralization studies on B.1.1.529 pseudovirus showed that 18 of the 19 mAbs tested lost 109 neutralizing activity completely or partially (Fig. 2c and Extended Data Fig. 3). The potency of 110 class 1 and class 2 RBD mAbs all dropped by >100-fold, as did the more potent mAbs in RBD 111 class 3 (REGN10987, COV2-2130, and 2-7). The activity of S309 declined modestly, whereas 112 Brii-198 was spared. All mAbs in RBD class 4 lost neutralization potency against B.1.1.529 by at least 10-fold, as did mAb directed to the antigenic supersite26 (4-18) or the alternate site23 113 (5-7) on 114 NTD. Strikingly, all four combination mAb drugs in clinical use lost substantial activity against 115 B.1.1.529, likely abolishing or impairing their efficacy in patients. 116 Approximately 10% of the B.1.1.529 viruses in GISAID1 117 also contain an additional RBD mutation, R346K, which is the defining mutation for the Mu (B.1.621) variant27 118 . We therefore constructed 119 another pseudovirus (B.1.1.529+R346K) containing this mutation for additional testing using the 120 same panel of mAbs (Fig. 2d). The overall findings resembled those already shown in Fig. 2c, 121 with the exception that the neutralizing activities of S309 and Brii198 were further diminished or 122 abolished. In fact, the entire panel of antibodies was essentially rendered inactive against this 123 minor form of the Omicron variant.”
The good news, though, is that I can’t see any reason for oral antiviral therapies, whose mode of action has nothing to do with the mutations on Omicron’s spike that help it evade antibodies, to be less effective against Omicron than against any other strain of SARS-CoV-2. Pfizer’s Paxlovid (nirmatrelvir and ritonavir tablets—not yet approved by the FDA) has been shown to reduce risk of hospitalisation or death by 88%. Lagrevio (molnupiravir tablets—already approved) should also maintain its efficacy—though as that was only about 30%, it’s usefulness is modest.
SUMMARYInfection rateOmicron is 5.41 times as infectious as DeltaCases are doubling at least every 2 daysOmicron likely already the dominant strain in the US and UKImmunityTwo-dose mRNA vaccine series gives only 19% protection against hospitalisation/deathPrior infection gives about 20% protectionTwo-dose mRNA vaccination plus an mRNA booster confers 55-80% protection against severe illnessTreatmentMost monoclonal antibodies are useless against OmicronTwo that maintain modest efficacy: sotrovimab (Xevudy)combo of amubarvimab and romlusevimab (Brii198)though one minor form of the variant renders *all* antibody therapy ineffectiveOral antiviral therapies will remain effective:molnupiravir (Lagrevrio) modestly so, with 30% reduction in hospitalisation/deathnirmatrelvir (Paxlovid) strongly so, with 88% reduction of samePreventionmRNA vaccines + booster still work well against Omicron, just not *as* wellAdd in masks—the better fitting and higher filtration rate the better—and you’re pretty safeCONCLUSIONGet vaccinated, get boosted, cancel travel-or-party plans, and wear a mask (KN95 or N95). Maintain social distance at all times, masked or not, and, until we have more data on disease severity, do not mingle indoors with anyone not a member of your household. Buy at least two rapid Covid tests from your local pharmacy plus a pulse-oximeter. If you feel sick—and Omicron symptoms look like a cold to start with (headache, runny nose, sore throat rather than fever and loss of smell)—test yourself then talk to your doctor. Hope the FDA okays Paxlovid very, very soon and that supplies can meet demand. There’s going to be a lot of demand.
Happy holidays.


December 14, 2021
Pre-order Spear as a holiday gift
Image description: A 3-D representation of a book, ‘Spear by Nicola Griffith.’ Above, lettered in black, ‘Coming 4.19.22…’ The background of the book cover is charcoal, shading to black at the bottom, with the author’s name at the top in orange-red and the title, at the bottom, and ‘from the author Hild’ in white. The main image is of a great hanging bowl of black iron with inlaid figures and great bronze escutcheons for the hanging hooks. It is wreathed about by smoke and flame and fumes, and the fumes form images: in white, woods with a woman and a stone and a sword; about the trees, shading to orange, is an figure with a spear on a horse; a fort gate and box palisade, and over all, flying up in the smoke towards the author’s name, two birds.
If you pre-order Spear from Phinney Books as a holiday gift (for yourself, for some other lucky person, for everyone you know), I will sign and personalise it/them for you when it arrives at the shop in April. For the first ten pre-order customers I’ll also include a specially-designed postcard with a hand-written message from me. All books (including those with the cards) will ship directly to you on publication.
To whet your appetite, here’s an eight-minute audio snippet of me reading from the beginning.
Audio clip of first 8 mins of SpearYou can read lots more about the book, including reviews, on the Spear book page.
December 13, 2021
Jolly Spearness
Happy Monday! My holidays are starting early with early reviews of Spear starting to come in. Five so far: Grimdark (“Gorgeous!”), Salon Futura (“Magnificent. I am in awe”), Publishers Weekly (“A genuine pleasure”), Shelf Awareness (“Vibrant and dazzling”) and Tor.com (“Brilliant. Gripping…and all-around marvellous”). I also have a growing selection of delicious quotes from other authors, which you can read on Spear‘s very own page.
In the prepublication phase of Hild I noticed just how many comps I was getting in early reviews and author blurbs (Beowulf, Tolkien, Sutcliff, Renault, Mantel, Dunnett…) , so I started tracking them. And on publication ran a giveaway competition for those who came closest to the final numbers. I thought I might do something similar with Spear, this time focusing on high-test adjectives (“Dazzling!” “Gorgeous!” “Brilliant!”). I’m not sure what the prize will be yet, but it will be spiffy.
And thinking of holidays and Spear, tomorrow I’ll post a holiday pre-order offer for you.
November 27, 2021
Omicron: Don’t panic
Omicron is the latest SARS-CoV-2 Variant of Concern (VOC), initially discovered and sequenced in South Africa.1 It is considered concerning because of the number and type of mutations—32 of them on the spike protein. Spike is the bit of the virus that a) gives the virus entrée into the cells, which affects transmissibility, and b) is used as the model against which to build vaccines. The worry is that the high number of mutations will make the virus must more transmissible and/or make it easier for the virus to escape not only innate immune response but the immune response acquired via previous infection and/or vaccination.
It’s pretty clear already that Omicron is, in fact, much more transmissible than either the original virus or today’s most prevalent variant, Delta. One graph I’ve seen indicates that Omicron took less than 20 days to reach a greater than 90% share of all sequenced cases in South Africa, whereas Delta took almost a 100 days to do the same. Don’t quote these figures because I’m just eyeballing pictures, rather than tallying tables of data, but its possible Omicron could out-compete Delta four times as fast as Delta out-competed other variants. In other words, if we could make direct comparison between the virus’s impact in South Africa to what will happen in the rest of the world, in a few weeks Omicron will be the only variant that matters.2
As for the ability to escape immunity—innate or acquired—no one knows yet, though preliminary evidence suggests reinfection rates with Omicron are high. Should it prove to escape immunity I think it’s likely a) it will only be partial and b) many of the treatments—particularly the corticosteroids and IL6 receptor blockers—will work. The antivirals may still be effective, depending on the mode of action.3 Also, if mRNA vaccines do turn out to be a little less effective against Omicron than against the Delta variant, both Pfizer and Moderna have suggested they could produce tailored vaccines within a 100 days or so.4
My real question about Omicron concerns virulence: is it more, less, or equally as deadly as other variants? In this regard I feel a very faint hope. There are some anecdotal reports from South Africa that it could, in fact—at least in the acute phase—cause a milder illness than other variants. Patients’ symptoms seem to be not only slightly different—fever, elevated heart rate (especially in the young), no loss of smell, not much lung involvement—but milder; they recover faster. (Having said that, it’s important to note that the group initially infected with Omicron were mostly university students—a very different health profile to the general population.) If the story of Covid were only about the acute phase, and if these early anecdotal reports were borne out by further study, then this would be fantastically good news: it could be the beginning of the long, winding road to Covid becoming no more worrisome than a bad cold.5
BUT. Okay, two buts. One, it may not be borne out when expanded to a wider population. And, two, the story of Covid is also about its chronic phase: Long Covid.
The data we have about Long Covid isn’t very good (in the sense that we can only talk about those who have been diagnosed with a positive PCR test—which could be a fraction of the whole). But what we do have suggests that more than one third of those testing positive for SARS-CoV-2, even those whose symptoms were mild, still have one or more symptoms 3-6 months later. Some people have Long Covid a year and half after diagnosis and it seems worryingly likely that for some it is a form of ME/CFIDS, which can be a debilitating, life-long condition. Because Omicron is newly sequenced, there’s absolutely no way to tell how or whether Long Covid percentages will differ. That could end up having a massive long-term impact on the overall health (and therefore healthcare burden, and therefore economy) of a population.
In conclusion: it’s probable that Omicron is more transmissible than other variants but even that is not yet certain. The rest is a series of questions that will be answered one by one over the coming weeks and months—and those answers could be a mix of good news and bad news. We just don’t know.
So for now: get vaccinated, get boosted, wear a mask, keep a couple of rapid home tests close by and test yourself and other members of your household if you’ve been exposed and/or show any symptoms.6 Above all: don’t panic. Precautions that work against Delta—masking, social distancing—will work against Omicron. And while, sure, it’s possible we could all die tomorrow of some super-virulent super mutation it’s also possible that Omicron could be an early holiday gift: the faint and tiny glimmering of a possibility that Covid may become a minor inconvenience, nothing worse than a cold.
1 Does it mean that’s where it originated? Not necessarily.
2 For comparison, the Delta variant is 70% more transmissible than the original. And of course we can’t compare South Africa to, say, North America directly: the demographics there are completely different. And the initial group of those infected with Omicron were university students—a really different profile. Nonetheless, I think by the New Year, Omicron may very well be synonymous with Covid here, in Europe, and almost everywhere.
3 but to what degree? The Merck antiviral pill has now been found to be only 30% effective against the symptoms of Covid, but Pfizer’s protease inhibitor, Paxlovid, which, if administered in the first five days, cuts the risk of hospitalisation by an almost unbelievably impressive 89%, is still looking very good. Though it has not yet, to my knowledge, been tested against the Omicron variant, given its mode of action I doubt it’s effectiveness will be massively reduced.
4 I’m assuming right now that AstraZeneca can, too. If you celebrated Thanksgiving I hope you gave thanks to medical science; I certainly did.
5 I repeat long. I repeat winding. There are many coronaviruses—including about 20% of those that now cause some of the illnesses lumped under ‘common cold’—that probably started out as deadly pandemics. (Possibly, for example, the so-called Russian Flu of the late 19th century.) But it doesn’t happen overnight. It can take decades.
6 You can buy them at any pharmacy. Buy a few. If you test negative, test again to be sure. If you test positive, go get a PCR test.
November 18, 2021
Two years later and 17 million dead
In November 2019 the corona virus, now known as SARS-CoV-2, first began infecting people in Wuhan, China. The earliest identifiable person with what is now known as Covid-19 first displayed symptoms on December 1. Then people started to die. Then it spread. The World Health Organisation declared a pandemic on 11 March 2020. To many of us it was perfectly obvious long, long before that we had passed the containable outbreak stage.
Two years after the virus’s first appearance, the official global death toll is about 5.1 million. I think that’s a serious underestimate; the Economist agrees, suggesting that the global total is closer to 17 million.
17 million is both a policy failure and a human triumph. It’s a failure because people are, well, people: not perfect. Looked at kindly, we don’t want to believe what is inconvenient or frightening. Looked at cynically, a lot of people used the pandemic as an opportunity to increase their following and/or strengthen their brand. It’s a triumph because people are, well, magnificent: we formed mutual aid networks, we worked heroically, we moved at feverish speed to bring together teams to research, test, produce, and administer vaccines, antivirals, and treatment best practises. Right now, if you are a healthy person living in any of the richest countries, you are very, very unlikely to die of Covid. This is because there are a series of medical filters available to you—or, in the case of antiviral pills, very soon to be available to you—that reduce the odds, stage by stage. The biggest and best filter is a mRNA vaccine, such as Moderna: two full doses followed by a half-dose booster.1 Then there are N95 or KN95 masks. Then there’s social distancing. Then there are HEPA filters. If you still somehow get the virus, and—even more unluckily—develop symptoms, then there are antiviral pills such as Merck’s polymerase inhibitor, Molnupiravir, which—if administered within the first five days of symptoms—reduces the risk of hospitalisation by 50%, and, even better, Pfizer’s protease inhibitor, Paxlovid, which, also if administered in the first five days, cuts the risk of hospitalisation by an almost unbelievably impressive 89%. If you don’t get the vaccine, or don’t get an antiviral early, then there’s still remdesivir, another polymerase inhibitor, by IV. If that doesn’t start helping and you begin to develop those first stages of inflammation that are really the most dangerous aspect of Covid, then there’s dexamethasone, a cheap but very effective corticosteroid. If that, plus the remdesivir, doesn’t help then you add in baricitinib, a janus kinase inhibitor, which blocks the activity of some of those enzymes that lead to inflammation. It is a series of almost miraculous science-based treatments filtering out and reducing harm.
For some, of course, the miracles are less effective. If your immune system is compromised—if you have to be on immune-suppressing medications for some kinds of cancer, for MS, organ transplants, or other conditions—then vaccines won’t trigger the production of antibodies and you can’t develop immunity. Luckily you can take the antivirals, and if you take them early enough your odds of staying out of hospital are very good.
Then there are those people who choose not to take vaccines.2 I won’t waste words on those selfish fools here.
Then, of course there are all those billions living in less rich countries who have very little access to any of the technologies I’ve mentioned here.
So where will we be two years from now? I don’t know. I think it’s likely Covid will be endemic in most countries; I think the virus’s deadliness will wax and wane; I think there will be waves of mutations—some more deadly that the Delta variant, some more contagious, and some—like Delta when compared to the original strain—that are both. But the antivirals will become cheaper to manufacture and eventually (I hope) available to all everywhere. Eventually, too, mutations will be routinely tracked and vaccines routinely tweaked to counter them. On the whole, I think Covid will become flu: occasionally terrible, mostly not. It’s the next new virus that worries me—but there will be another (and another, and another).
But the Covid-like-flu evolution is very much a people-are-magnificent scenario which, as we’ve seen, we can’t always afford to rely on. It is also predicated on the no-new-disasters-soon scenario—whether geopolitical, climatological, financial, or one of those wild, from-left-field unk-unks such as asteroids, aliens, and inter-dimensional portals. Hey, after the last six years you look me in the eye and tell me none of that can happen…
1 I have, as they say, Some Thoughts on the booster shot but will save it for another post.
2 There are a few people, particularly from traditionally marginalised groups, who have every right to be wary of government-sponsored medical treatment; I think they’re dangerously wrong, but I hope we can all do a better job of listening and helping assuage their wariness
November 13, 2021
Kitten report #20: Not dead yet [photos]
Today Charlie and George are exactly two and half years old—and I am Officially Tired of reporting on their near-death experiences. Before we even met them both came close a couple of times—their four litter mates did not survive. Then Charlie had a disastrous reaction to anaesthesia during an operation to remove a polyp, resulting in brain damage—from which he’s made a remarkable recovery. Then George ate a bird infected with salmonella and spent a couple of days in kitty ICU—though, like Charlie, made a remarkable recovery (without brain damage).
Last week, it was George’s turn again: this time it was poison. But yet again, he’s made a remarkable recovery and is more or less back to his old self–except he’s very jumpy, and sticking much closer to me than usual. There again, they’ve both been jumpy and sticking closer to home—mainly because we’ve been travelling for the first time in their lives, and they Do Not Approve.
I’ve already talked about one set of travel we did in September/October. A week later we had to be gone again for a visit to Saint Martin’s University in Lacey. Then last week Kelley had to make an unexpected five-day trip back to Florida (but that’s not my story to tell). She left at five in the morning and by ten o’clock George was very unwell—drooling gallons (he sat on the threshold of the family room and living room for five minutes, and when he moved away there was an actual pool—not a few drops, a pool about 18 inches wide)—not eating, and barely able to move, and when he could move wanting to drag himself under the sofa where no one would be able to reach him and he could die in peace. He behaved in much the same way with salmonellosis. It took me a long time to figure out what the problem was, and I am enormously grateful a) that I didn’t figure it out until he had already turned the corner for the better, and b) for his strong constitution.
George’s downfall was a broken bottle of diluted grapefruit essential oil.1 It smashed on the bathroom floor the morning Kelley was leaving, and Kelley swept, then wiped, then actually washed the floor—because oil, because slippy, because I don’t walk well—before she left at zero-dark-thirty for the plane. George hates the smell of citrus so I’m pretty sure the closest he got to the grafefruit oil was walking across the swept wiped, and washed floor then licking his paws. And that was enough.
Because here’s what I know now that I didn’t then: grapefruit is a deadly poison for cats. So much so that if they ingest any, do not, under any circumstances, administer an emetic—because if they even breathe in the fumes from the vomit they could die. Yes, it’s that bad. But as I say I didn’t know that until George was already clearly improving: salivating less, coming for comfort, eating a bit. Oh, don’t get me wrong, he still looked woebegone, and he was moving like a little old man, but he was no longer trying to escape himself and everyone else by crawling into a hole and dying. I found out that evening about the grapefruit oil, looked it up, and my stress went through the roof. I was up most of the night fussing over George, until he basically gave me the, Oh stop *fussing* for heaven’s sake and let me get some sleep! look, and Charlie came and laid his paw on my forearm and looked at me gravely as if to say, I’ve got this, go to sleep. So I did—only to be woken three hours later by the two of them having a knock-down-drag-out fight then thundering all around the house—up and down curtains, over and under furniture, knocking things off the counter—then yelling at me comprehensively about their empty food dishes. So, yeah, George is fine.
And he’s a bit different: much, much more cuddlesome.
 Please don’t ever go away again
Please don’t ever go away againImage description: Large tabby cat clinging desperately, possessively to a white woman—his paw is curled around her forearm from above; his tail is curled around her arm from below—relaxing on an ivory sofa with a big mug of tea
Charlie is too—though of course that’s as likely to be the result of the miserable weather we’ve been having the last 10 days as any sudden increase in gratitude:
Image description: A screenshot of a Seattle Times article with a photo of waves crashing against a pier and below a single sentence, “A tornado warning, heavy rain, hail, high winds, severe thunderstorm, snow and a small earthquake were part of a mixed bag of events that occurred during a dramatic Tuesday in Washington state.”
So, before that little incident, how have they been? Fine! Happy, healthy, curious, plus in-my-face, on-my-keyboard, complaining about the service, and assuming a new throne.
The throne, of course, is Charlie’s: I have a new wheelchair (more on that in another post)2, which has become the most expensive kitty bed on the planet:
 Most expensive cat bed in the world
Most expensive cat bed in the worldImage description: Photo of an all-black wheelchair against an orange wall warmly lit by candlelight. A small tabby cat is curled on the chair fast asleep.
George, when he’s not coming for lap time, is mooching treats.
 Nothing will solve George’s existential crisis except another treat
Nothing will solve George’s existential crisis except another treat George is weighed down by one hundred and four individual cat treats now filling his belly.Hey, you tried to poison me; it’s only fair you now feed me instantly on demand
George is weighed down by one hundred and four individual cat treats now filling his belly.Hey, you tried to poison me; it’s only fair you now feed me instantly on demandImage description: Two photos of the same tabby cat posing on the same brown velvet cushion. On the left he sits upright looking sweet and sad and soulful (but you can just tell he’s laying on thick). On the right he sits in half profile meatloaf style looking full, smug, and not-far-from-sleep
Both of them are now proper cats. That is, when they’re not running around outside killing things, or mooching food from us—even Charlie has started to enjoy cat treats3—they sleep. Charlie’s three favourite daytime places are my exercise machine—a NuStep, which is a recumbent cross-trainer—my wheelchair, and my lap. They sometimes compete over laps.
 The Adoration
The Adoration He’s looking, isn’t he? Ha ha ha, all mine George!Image description: Two photos—on the left, a white woman with short hair sits cross-legged on an ivory sofa with a small tabby cat in her lap gazing at her adoringly. On the right, the same tabby, now demonic-looking, sits on a woman’s lap trying to see through the back of his head to another tabby sitting on the floor staring at the other cat in what could either be envy or threat
He’s looking, isn’t he? Ha ha ha, all mine George!Image description: Two photos—on the left, a white woman with short hair sits cross-legged on an ivory sofa with a small tabby cat in her lap gazing at her adoringly. On the right, the same tabby, now demonic-looking, sits on a woman’s lap trying to see through the back of his head to another tabby sitting on the floor staring at the other cat in what could either be envy or threatWhen Charlie can’t have a lap or my chair or the exercise machine—or just when it’s colder than usual—he seeks out the second most expensive cat bed in the world, which is our Denon receiver.
 Swimming in a dream—he and I both love the Apple TV+ screen savers
Swimming in a dream—he and I both love the Apple TV+ screen savers Dreaming of catching bats—which you’ll understand if you’ve seen the showImage description: Two photos. On the left, a TV screen and, below, a cat on an audio receiver, all in cool blue tones. The screen is showing deep sea jellyfish; the cat is oblivious: he’s asleep. On the right, all in sepia tones, a TV and a TV console with audio receiver. The screen is showing a chiaroscuro still from Midnight Mass: the priest in the confessional. Below, fast asleep on the audio receiver, a small tabby cat with his white chin to the sky, clearly having blissful dreams.
Dreaming of catching bats—which you’ll understand if you’ve seen the showImage description: Two photos. On the left, a TV screen and, below, a cat on an audio receiver, all in cool blue tones. The screen is showing deep sea jellyfish; the cat is oblivious: he’s asleep. On the right, all in sepia tones, a TV and a TV console with audio receiver. The screen is showing a chiaroscuro still from Midnight Mass: the priest in the confessional. Below, fast asleep on the audio receiver, a small tabby cat with his white chin to the sky, clearly having blissful dreams.At some point I plan to do a whole blog post about our new AV setup, but for now I’ll just say OH MY GOD I LOVE MY DOLBY ATMOS SOUND! I love it so much that I’m seriously considering spending an unreasonable amount of money to hunt down and buy any of my favourite music that’s been remastered for Atmos. It’s that fucking good. No, it’s better: it’s mind-blowingly magnificent! If you’ve been dithering about getting something similar, just do it. It is so very worth it. One drawback: George doesn’t like the sound moving around the family room: it’s so clear and convincing and so precisely placed that he can track it to within inches but can never see it. It freaks him out. But hey in this one regard, humans win.
Charlie used to be bothered by it, but now doesn’t get fussed. Perhaps it’s because of his brain damage—I’m pretty sure he spent some time seeing things that were’t there, and now not seeing things that are there is just another manifestation of the weirdness he’s grown used to—that and the fact that he’s always been less skittish than his brother. But, yes, he too loves his audio receiver.
I’ll leave you with a picture of him posing as the Emergency Medical Hologram from Star Trek: Voyager.
 Please state the nature of your emergency
Please state the nature of your emergencyImage description: A poised and alert tabby cat with perfectly curved whiskers sitting before a blank TV screen on an audio receiver with his tail curled precisely around his paws, looking quizzically into the camera
Perhaps I’ll post another Kitten Report over the holidays. Meanwhile, feel free to catch up on previous kitten reports.
1I use it as a mosquito repellant; it contains nootkatone—which is an even better repellant than DEET and absolutely nontoxic, to people. You can drink the damn stuff. I dilute five drops of essential oil with several tablespoons of neutral oil and it works like a magic shield. Also, it smells nice. I can recommend it. But obviously not for cats.
2 When I say expensive, I’m not kidding. But, oooh, it’s supercool!
3 They like Orijen, original flavour, which are whole-prey (muscle, organ, bone) dehydrated raw food pellets. They love to chase them.
October 28, 2021
Spear available on NetGalley
For booksellers, librarians, producers, reviewers and other book professionals, Spear is now available for request on NetGalley.
The digital galley doesn’t have the gorgeous interior illustrations by Rovina Cai, and the long, historically-focused Author’s Note is not left-justified1 but otherwise it’s a faithful reproduction of what you’ll read in the finished hardcover and ebook (or hear in the audiobook).
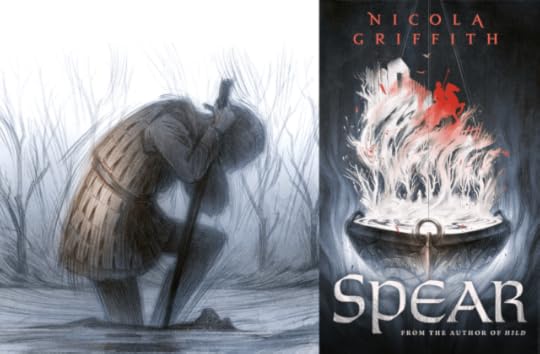
Image description: A composite image with, on the left, painted in muted colours—ice blue, umber, fawn—a figure half kneeling in a river leaning her weight on something submerged, perhaps another figure, with her sword. And on the right, the cover of a novel, Spear, by Nicola Griffith, also in muted colours, this time white, dark blue, bronze, charcoal, and ember-red.
The book won’t be out until April 19 next year, but requests are beginning to roll in for appearances, real and virtual. If you want me at your store/conference/school next year, now’s the time to get in touch with my publicist at Tor, Alexis Saarela. I have no idea where the world will be, pandemic-wise, but I have my fingers crossed for some live and in-person events.
Meanwhile I’m turning my attention to a couple of juicy essays I’ve been meaning to write for a year or two, and some blog posts of varying heft about all the things I learnt, and/or discarded, and/or think I might use in some future Peretur tale. So tell me what you’re curious about and I’ll see what I can do.
[1] It’s centre-justified, so it looks as though it should be written on a scroll, and read like a municipal proclamation: Hear Ye, Hear Ye, Whereas on this twenty-seventh day of October, in the two-thousandth-and-twenty-first year of this Common Era, the Author did herein note—
October 21, 2021
OtherLife now on Prime Video!
OtherLife, the film Kelley wrote based on her novel, Solitaire, has moved from Netflix and is now available on Prime Video.
Turning a long, speculative “stylistic and psychological tour de force” (New York Times) novel into just over 90 minutes of sleek, luscious-looking sci-fi thriller, all on a low budget, was a rollercoaster ride: sometimes wildly exciting, sometimes grindingly hard, but never, ever boring. But that’s Kelley’s story to tell and happily she’s done that in a fascinating series of journal entries about the 11-year journey from book to screen. You’ll find it an eye-opening read. It was not always a smooth ride and the only reason that f illm ever got made was through the sheer force of Kelley’s will. I’ve never been more proud of her—and I’m proud of her a lot.
In the US, you watch the film here: https://www.amazon.com/Otherlife-Jessica-Gouw/dp/B091FXHR8T
In the UK, here: https://www.amazon.co.uk/OtherLife-Jessica-Gouw/dp/B077VTKPQS
And to help you make up your mind you can watch the trailer on YouTube:
October 19, 2021
Monstrously good! [video]
What is monstrously good and coming in exactly 6 months? Spear!
Monstrously good…Video description: a T-Rex stomping about (and roaring at the occasional overhead pterosaur) on top of a pile of advance reading copies of the novel Spear by Nicola Griffith.
But you can, of course, pre-order the hardcover, audio, and ebook editions right now from these fine retailers:
IndieBound | Amazon.com | Bookshop.org | Barnes & Noble | Amazon.co.uk
Or see this enormous list of independent booksellers in the UK, US, Canada, Australia, New Zealand, and Ireland.
And it would be a good idea to pre-order now, especially if you want a hardcover copy. Why? Three reasons—two that almost always apply, and one that’s special to these pandemic times.
First, pre-ordering is good for you, the reader—once you’ve plunked down your cash you don’t have to worry about remembering anymore. When I know there’s a book I definitely am going to want, the best way to make sure I get it—because who can remember things like publication dates?—is to just buy it now and relax knowing it will magically arrive the first day it’s available.
Second, even in the best of times, it’s good for the author. Here’s what one publisher has to say about it1:
For an author, pre-orders can alert retailers and consumers that they should pay attention to your book. From the bookseller perspective, the pre-order quantity is a good early indicator of a book’s success, and can lead to retailers increasing their initial orders.
Additionally, pre-orders can have a ripple effect in the broader publishing industry, and a pre-publication buzz campaign in support of pre-orders can build anticipation for your book launch, allowing you to carry momentum through the weeks following your on-sale date.
Third, today—mid-pandemic—is most definitely not the best of times for publishing. You’ve probably heard that there are global supply chain disruptions affecting all sorts of industries. Publishing is one of them. One of Seattle’s booksellers, Robert Sindelar of Third Place Books, recently spoke to the New York Times about this. Shortages and shipping bottlenecks are occurring at several different points in the chain: not enough paper, not enough workers to print, bind, pack the books, not enough shipping containers to put them in, not enough ships to carry them, or workers to unload the shipping containers when they arrive, or trucks to transport the books to the warehouses, and from the warehouses to the stores, and so on. Print runs are usually ordered far in advance, so a publisher has to make an informed guess about numbers. In the best of times it doesn’t matter too much if they underestimate; it’ll only take a couple of weeks to print more. But, yeah—right now not the best of times. An author’s worst nightmare: readers queuing up to buy the delicious hardcover and there being no copies available anywhere and no idea when there might be.
So if you want to read Spear—and it’s monstrously good!—do you, me, and the publisher a favour and pre-order now. And keep the receipt so that closer to publication date you can enter to win a spiffy enamel pin.2
Penguin RandomhouseThe Spear pin is so great I actually wear in on my jacket lapel. I can’t remember the last time I liked something well enough to do that with—oh, well, okay, yes I do :)October 11, 2021
Wednesday October 13, 7 pm: Les Bailey Writers Series, Saint Martin’s University
Image description: a flyer for an event. On the left, text reading “Saint Martin’s University Les Bailey Writers Series, Nicola Griffith, Making and Remaking the World, Wednesday October 13, 7:00pm, Worthington Center St Martin’s University,” followed by logos for St Martin’s University and Barnes and Noble. On the right, a black and white photograph of a smiling short-haired white woman at a microphone.
On Wednesday evening I’ll be in Lacey, WA at the Worthington Center, Saint Martin’s University, to give a public talk, Making and Remaking the World. Actually, it’ll be more of a guided conversation: Kelley will be asking me questions and we’ll talk for about an hour, then I’ll answer audience questions—often my favourite part of events like this—and then I’ll sign books. The university bookstore will be selling copies of Hild and So Lucky, but if you bring personal copies of any of my other works I’ll be happy to sign them.
So what does “Making and Remaking the World” mean? The long answer is basically my PhD thesis, plus every essay I’ve ever written about my work. The shortest answer is all about how and why I write—and who I write for. I write to some degree for myself—I write to find out—but I also write to change the world, one reader at a time. I write to see myself, and others like me, like you, in pasts, presents, and futures we’ve been told don’t belong to us. I build fictional worlds where we can all not only survive but thrive. And by building fictional worlds, and putting traditionally underrepresented people in them, I help recast attitudes we hold towards the world we live in today. And changing attitudes changes culture.
Some of the conversation will be about how I do that, and some about why I do that. I may or may not include a couple of very short (2 mins or so) readings—I haven’t decided yet.
Perhaps that sounds weighty and serious—and to an extent it is—but as one of the truest reasons I write is for pleasure, I’m hoping the conversation is pleasurable, too. When I write—and speak—I don’t just want to change the real world, I want the fictional world the reader lives in to delight them, thrill them, fill them with joy. Because in my experience joy is contagious: if my work fills you with joy, you may then go out into the world and fill others with joy. And that, too, will change the world.
Making and remaking worlds—this one or any other—does not have to be onerous. So come and join me and Kelley for a lovely evening of conversation and exploration.


