
Lynda Huey's Blog, page 2
October 21, 2015
Win-Win: Prevention of Hip Surgery or Prehab

 0
0


 Follow By Robert Klapper, M.D. and Lynda Huey
Follow By Robert Klapper, M.D. and Lynda HueyJust as in the world of business, we like to talk about a win-win situation. Working to prevent hip surgery can create several wins for you. The ultimate win, of course, is that you follow the programs in this book, relieve your hip pain and dysfunction, and never need hip surgery of any kind. But there are several other possible wins. After several months of doing our pool program, you are likely to realize you’re in great shape, so you keep the water at the center of your lifelong fitness plan. It may turn out that you’ve postponed the need for hip surgery by five or ten years. That’s significant because technology keeps improving, and the surgery of the future will no doubt be superior and easier. But the other win is that even if you find yourself eventually scheduling a surgery, you will have become much stronger and able to bounce back more quickly.

Let’s say you come to our pool. When we first see you, we won’t be certain which path you will be on: Will you be avoiding the surgery? Postponing it? Doing a prehab program that will get you stronger before surgery? As we begin, it doesn’t matter. We just get started with our highly successful pool program—always with the intention of preventing surgery. About a month into the program, we expect to see improvement, first in pain reduction, then in improved range of motion, strength, and flexibility. We modify our expectations and plan for the future based on the results we see. We increase the effort of the exercises you are performing in order to help you become strong with greater mobility in your activities of daily life and your sports.


You can do the same, using the programs in Heal Your Hips Second Edition. Just start! Do the work and see where it takes you. Don’t be impatient. It might take up to a month before you start feeling improvement. Don’t give up too soon! You may be one of the lucky ones who regains good function and strength in your hip, and even though your X-ray or MRI hasn’t changed, you are out of pain and no longer considering surgery.
Some of you, however, may find that despite your best efforts, your pain may be continuing. If you have done the rehab program for two to three months without major reduction of pain, you may have to conclude that you are no longer going down the Prevention path as you had hoped, but rather are on the Prehab path. Remember, that was the final win. You have benefited from increased strength and ability due to your new exercise routines. And now you must refuel your commitment to continue training to be physically powerful enough to withstand the rigors of surgery and recover quickly.
There are two key reasons you may ultimately decide to have hip surgery: pain that keeps you awake at night or realizing your back or knees have started to hurt because you’re using them to compensate for lack of movement in your hip. You don’t want to ruin joints that are innocent bystanders as you keep trying to save your hip. At some point, you will begin to build toward the decision for surgery. You and your doctor may realize that the degenerative process has gone too far for any solution other than hip arthroscopy or hip implant surgery, which are explained in chapters 13 and 14 of Heal Your Hips Second Edition.
Water Rehab Specialist, Lynda Huey, MS, earned a bachelors and masters degree from San Jose State University where she also starred on the track and field team. Her own athletic injuries led her into the water where she learned to cross train and speed the healing of injuries. She has written six books on aquatic exercise and rehabilitation, books that are considered the foundation of aquatic therapy world-wide. Lynda is President of CompletePT Pool & Land Physical Therapy in Los Angeles.


October 8, 2015
Heal Your Hips: How to Prevent Hip Surgery and What to Do If You Need It
Orthopedic surgeon Dr. Klapper and aquatic rehab specialist Lynda Huey have been collaborating since 1994. That was the year NBA star Dr. Klapper arthroscoped Wilt Chamberlain’s painful hip. Dr. Klapper was one of the pioneers in doing arthroscopic surgery in the hip joint, and Wilt wanted what was then an advanced technique. Wilt told Dr. Klapper he was going to do aquatic therapy with Lynda Huey, who had been helping many of the world’s best Olympic and professional athletes speed the healing of their athletic injuries in water.
Lynda had already published three books when she met Dr. Klapper, so when those two clicked, it was inevitable they would write books together. Their first book, the first edition of Heal Your Hips, was published in 1999. It was the only book of its kind to speak directly to readers with hip problems and offer them healing treatments that included a full aquatic rehab program. Every other book about hips and hip surgery was written by surgeons for surgeons. If books offered exercises for hips, none of them included a single pool exercise. To this day, Heal Your Hips remains the only book of its kind.
On October 13, 2015, the Second Edition of Heal Your Hips will be published, offering over 50% more information on hips, including the explosion in new information about hip pain, hip preservation, and the latest diagnoses that have changed the entire landscape of hip care. Full programs of rehabilitative exercises are shown for both pool and land. The photographs and text are easy to follow with spectacular underwater and above water shots. These photos alone are a great reason to own the book: They were shot in a gorgeous backyard pool in Pacific Palisades overlooking the ocean. A scuba diver photographer shot the underwater pictures as Lynda Huey climbed in the pool beside him to get the form correct.


The graphic art was worked on again and again to make complicated medical issues easy to understand. Radiological studies and drawings with clear captions show examples of various hip conditions such as osteoarthritis, rheumatoid arthritis, torn labrum, avascular necrosis, femoroacetabular impingement (called FAI), dysplasia, and other common complaints.
The mission statement for this book is to hold the reader by the hand and provide hope and clarity as he or she struggles through the medical labyrinth. The first goal is to help readers try to prevent hip surgery. But if they try the conservative methods in this book and still can’t sleep at night or can’t participate in activities they love, they are guided cautiously toward prehab for surgery – rehab exercises to become strong enough to face surgery and recover quickly. This is the book for anyone who is fearful about their future because of hip pain. It speaks to them in a calm, caring voice full of wisdom and information.
Water Rehab Specialist, Lynda Huey, MS, earned a bachelors and masters degree from San Jose State University where she also starred on the track and field team. Her own athletic injuries led her into the water where she learned to cross train and speed the healing of injuries. She has written six books on aquatic exercise and rehabilitation, books that are considered the foundation of aquatic therapy world-wide. Lynda is President of CompletePT Pool & Land Physical Therapy in Los Angeles.
September 3, 2015
Alex Rasouli, M.D. – 90% of Back Problems Don’t Need Surgery!
By Alex Rasouli, M.D. and Lynda Huey

The spine is a collection of bones and ligaments that are subject to wear and tear, but if the body is injured the body’s very sophisticated healing mechanisms come into play. If a patient comes into my office with excruciating back pain, can barely move, and has been bed-ridden for even a few weeks, he is probably swearing that he needs surgery to fix things. But that same patient will normally come back to my office six weeks later and be completely fine even if we did nothing. Of course, you can accelerate that process by doing things like physical therapy, taking anti-inflammatories, and icing, but that example is just to point out that the body’s healing ability is remarkable. Time and time again, we see the statistic prove itself that 90% of all back problems resolve themselves and don’t need surgery. The body does a better job than a surgeon ever could do. That’s true for back pain; it’s true for sciatica; it’s true for disk herniations; and it’s even true for spinal fractures. It’s humbling for a surgeon to say, but it is true.
Time and time again, we see the statistic prove itself that 90% of all back problems resolve themselves and don’t need surgery.
–Spine Surgeon Alex Rasouli, MD
Let’s say a patient develops back pain that does not resolve within two or three days. That’s about how long most people are willing to tolerate some pain, because they aren’t eager to see a doctor. But if the pain doesn’t resolve within a few day, the patients starts to become alarmed, at which point they will see medical attention. They may see their primary care doctor or they may come directly to me. It will generally take the patient one to two weeks before they see me in my office for a persistent pain or discomfort in the back or neck or for pain going down the legs or the arms. At that time we will get some studies, an X-ray and an MRI if they complain of nerve pain.
Both the X-ray and MRI are good tools. We’re concerned about cost and value and efficiency of care, so we start with the X-ray which is more cost effective to use initially. The X-ray is obtained with the patient standing upright against gravity. We shoot one X-ray from the front and we shoot three from the side with the patient standing neutral, bending forward, and bending backward. This gives us a great lay of the land. Are all the bones aligned properly? Is there a fracture? Is one bone sliding past another showing instability? Is there a tumor? All these can be determined on an X-ray.
The MRI gives us a more detailed picture, because you can see things there that you can’t see on an X-ray: disks, nerves, and other soft tissue subtleties. I can see if there’s a disk herniation or an injury to a ligament. I look at the integrity of the bones (the vertebrae), the integrity of the disks, and the integrity of the nerves that run right behind the bones and the disks. The MRI helps me locate the source of the patient’s pain and gives me the ability to predict for the patient how long they are likely to be in this pain and what they can do about it. I often explain to my patients how tightly things are packaged in the spine. There isn’t much space, so a problem with a bone or a problem with the disks or ligaments will often become a problem of the nerves as well. If there is an injury to one structure, it easily affects the other structures around it.
We review the studies, and unless it’s something significant like stability, infection, or a tumor, I tell them to do physical therapy for at least four to six weeks. They can also do ice and heat treatments at home and do mat Pilates with an instructor who is well-trained in working with back conditions.
Physical Therapy
While “Tincture of Time” is being applied to a patient’s back pain, we like to see him or her moving, because movement stimulates healing. Probably the safest place to exercise is in the water. As soon as the patient enters the warm therapy pool, the muscles relax and movement becomes easier. Once the patient is in chest-deep water, he weighs only one-third of his normal weight. If a flotation belt is added and the patient is taken to deep water where his feet cannot touch the bottom of the pool, he becomes weightless and feels no impact with movement.
Back pain is often accompanied by a lack of core muscular strength – the abdominal muscles and other muscles of the torso. Thus aquatic therapy programs often focus on building such strength in order to support the back better. The program can start with something as simple as walking in chest-deep water. The water’s resistance forces the core muscles to work as the body moves forward, backward, and sideways. A next step up can be marching. Then patients are usually taken to the deep end of the pool where they can be totally free of gravity. They hold the side of the pool and do bicycling or running while they learn to activate their core muscles for stability. They also do walking motions and open and close their legs out to the sides. All exercises can be modified to be easier for anyone who experiences pain.

Deep-Water Running, Cycling, or Marching holding the side.
Stretching is next. It’s great to do stretching exercises in the water, because people can float into positions for the stretches that might otherwise be difficult to reach if performed on land. Then a significant amount of time is allocated to helping patients gain strength as they reduce their pain. Learning to hold the core muscles strong while moving the arms and legs is a big part of that process. By leaning back on the side of the pool, patients can brace themselves in order to get started. As they progress, they move away from the side of the pool to do upper body exercises while using their new-found core strength to balance. Once patients can keep their core muscles tight as they breathe and do upper body exercises, they learn to maintain that same muscular activation as they do lower body exercises.

Windmill Stabilization braced on the pool wall.

Squats.
These are three examples of exercises that can speed the recovery of back pain patients. Many more exercises are part of the program at Lynda Huey’s CompletePT, including the distraction technique shown next, which helps reduce pain.

Distraction technique (or Floating Traction)
The vast majority of patients resolve their back pain while doing conservative management of their condition. But there is that 10% of patients who may end up needing surgery.
The Exception – Time for Surgery
I sometimes wait on patients’ issues to die down for up to three months. During that time they can continue to do more physical therapy, take anti-inflammatories, and modify their activities. For example, they may have bad sitting hygiene at work – they sit for too long and they don’t get up and move around. Or they may have dietary indiscretions – eating foods that cause inflammation or cause them to gain excess weight. They may have other stresses in life. All these contribute to pain. But if by six weeks to three months, depending on what we find with the case, the patient is still not feeling better, then it’s time for something more interventional such as an injection of steroids or surgery. If a problem is going to heal itself, it’s rare that it doesn’t heal by three months.
I love doing surgery, but I want to avoid surgery, too. Who doesn’t? –Spine Surgeon Alex Rasouli, MD

Alex Rasouli, MD
Spine surgery is reserved for the very small sliver of cases where the test of time has been employed and the patient is still suffering no matter how many weeks or months have passed. There are conditions for which surgery is the best answer. Scoliosis (curvature of the spine) is an architectural issue that demands a surgery. The patient may have endured years of pain, continues to be in pain, and is actually getting worse. That would be a time to step in with surgery to straighten the curved spine. Another condition that requires surgery is spondylolisthesis, where one vertebrae of the spine moves forward of the vertebrae below it creating an unstable spine. Tumors and infections are other conditions that call for surgery.
There are a minority of cases in which massive disk herniations put extreme pressure on nerves that cause significant weakness of the arms and hands or the legs and feet. These large
herniations are an example of a condition that time will not heal. And there are several other conditions that the body’s regenerative powers simply can’t heal. In fact, they get worse over time. But remember: 90% of back problems do get better on their own.
People want to avoid surgery. I’m a surgeon. I love doing surgery, but I want to avoid surgery, too. Who doesn’t? We want more people to understand this so they don’t have back surgery unless it is a true necessity.
Dr. Rasouli on Being a Spine Surgeon
A doctor has to be perfect – he just has to be. Other professional don’t necessarily have to be perfect, but a physician, particularly a surgeon has to hold himself to the highest standard of perfection that only comes from within. The philosophy that I use every day whenever I recommend a treatment for a patient is to stop and ask myself, “If I had the same condition as this patient, is this what I would want done to me?” If the answer is no, I’m not going to recommend that treatment to a patient. If the answer is yes, then I’ll tell the patient, “This is what I would want done on my back and so I’m going to recommend it to you.”
To me, skill and conscience are the two important pillars. You can have great skill as a surgeon, but if you lack the conscience, you will execute surgeries very well, but eventually you’ll make a mistake. The mistake won’t be in the execution of the surgery; it’s going to be in performing the surgery on someone who didn’t clearly need it. You’ll find that the more conservative surgeons are the more experienced surgeons, because they know that surgery often is not the answer. They have had humbling experiences where, although they have seen things go well, they have also seen when things did not go well. That makes them quieter, calmer, less eager to jump into surgery with their patients.
What to Look for in a Spine Surgeon
Not everyone can come see Dr. Rasouli in Los Angeles, so here are some pointers in finding a back doctor with the kind of conscience he displays.
Experience is important. It doesn’t matter how old the doctor is. You want to consider how long he’s been doing the specific surgery you’re contemplating and look at his outcomes. The more experienced surgeons speak with a bit more humility than somebody that’s new. They have confidence that allows humility to be expressed. Inexperienced surgeons can be insecure and they want to do surgeries, but they don’t yet have the benefit of humbling experiences. If a surgeon has been doing surgery a few years and does 400 to 500 cases a year, that’s a healthy number.
Look out for a doctor who is very quick to recommend surgery. Most often spine surgery is something that can be done after time has been applied to the case and shown itself not to be the answer. If time isn’t the answer, surgery might be.
The surgeon should discuss alternatives to surgery and see if that’s of interest to the patient. Surgery is merely one tool in the repertoire with a lot of other non-surgical management techniques.
The final test is to ask, “Doctor, is this what you would do to yourself or a family member?” Ask the doctor point blank. If you see hesitation in the doctor’s eyes, think twice.
Spine Surgeon, Alex Rasouli, MD, went did his undergraduate work at Stanford, then went to medical school at the University of California, Irvine where he also did his residency. He did a fellowship at the prestigious University of Miami-Jackson Memorial Medical Center. Then he joined the staff at Cedars-Sinai Medical Center where he introduced computer-guided surgery in the spine. For a child prodigy who wrote his first computer program at the age of five, that was a natural extension.
Water Rehab Specialist, Lynda Huey, MS, earned a bachelors and masters degree from San Jose State University where she also starred on the track and field team. Her own athletic injuries led her into the water where she learned to cross train and speed the healing of injuries. She has written six books on aquatic exercise and rehabilitation, books that are considered the foundation of aquatic therapy world-wide. Lynda is President of CompletePT Pool & Land Physical Therapy in Los Angeles.
August 11, 2015
June 18, 2015
Pool Workouts for NBA Centers Wilt Chamberlain & Emeka Okafor
In the 1980s, when I first started taking some of the world’s best athletes into the pool, my long-time companion Wilt Chamberlain had elbow surgery by Frank Jobe, M.D. to repair a triceps tendon he had torn playing racquetball. Wilt wanted to speed healing and we had learned that pool workouts certainly seemed to do that. Thus I took Wilt into his home Jacuzzi to let him bend and straighten his elbow in the buoyancy of water. (See photo.)
Dr. Jobe did a high tibial osteotomy on Wilt’s knee some years later. Right away I began giving Wilt my full pool program three to four times a week. We did deep-water running, walking and jacks to keep his high level of cardiovascular fitness without any impact to his knee. Stretches and range of motion exercises for the knee soon had it moving smoothly. As the knee healed we could do shallow water running and jumping exercises with a flotation belt. That way he could jump up and the belt and water could catch him on his landing so the repaired knee didn’t have to work nearly as hard as it would have to do if he were jumping on land. Over the next months, we got him back to playing tennis and paddle tennis.
After Robert Klapper, M.D. performed arthroscopic surgery on Wilt’s left hip in 1994, we returned to the pool for forward, backward, and sideways walking – a lot of it so that he could relearn a walking pattern without a limp. We did the deep-water interval training, the shallow water running and the plyometric jumping exercises. What Wiltie loved best, though, was the kicking series. He loved it! We started doing each of the six kicks for thirty seconds, then 45 seconds, then a minute. Over the next month we built up to doing two minutes for each of the six kicks, increasing the speed and force for the last minute of each one. That was a tough workout all in itself.
ICE: A Free, Frozen Miracle
Ice is life’s most under-recognized drug and it needs no prescription. It’s right there in your freezer waiting for you. It’s easy to apply to an injury and quick to start working.
When an injury occurs, immediate application of ice constricts the capillaries to help prevent bleeding and swelling in the injured and creating a bruise. The use of ice decreases the need for anti-pain medication because it is a surface stimulant that overrides the pain in the injured area. Ice slows nerve conduction velocity. In other words, ice shuts down many nerve impulses that your brain interprets as pain.
Apply lavish amounts of ice to your injury and the area surrounding it. Use a large ice bag, a bag of frozen peas, or a gel ice pack – anything you have that will act as ice. Leave the ice in place ten to twenty minutes, then remove it and place a dry towel around the cold skin until you feel the area thaw. Wait thirty minutes and then apply the ice again. Ice off and on as often as possible during the first two days after the injury, then reduce this treatment to twice a day until the injury heals.
In treating neck and back, ice is applied to alleviate pain, spasm or inflammation even though the initial discomfort of the cold may give the impression of stiffening the muscles. Stay relaxed, stay with it, and the ice treatment will force the muscles in spasm to relax and return to their normal resting length.
One of the main reasons people “forget” to ice is that they don’t want to sit still to do it. Now there is no excuse. You can use ICE/HEAT by TRU-FIT. This product consists of a freezable gel pack, insulated soft fabric wrap, and an elastic extension strap. The strap holds the gel pack in the most desirable position over your knee, hip, back, shoulder or other injury site. You can wrap the ice bag snugly around any injury and continue your daily activities at work or at home. So while you cook dinner or write your daily blog, you can strap on some ice and speed the healing of your injury – not bad multi-tasking!
Once you are past the first forty-eight hours of your injury the gel pack can go into the microwave and be heated to offer contrast treatments – first cold, then heat, then finish with cold.
Lynda Huey, M.S., founder of CompletePT and Huey’s Athletic Network, is a former athlete and coach whose own injuries led her into the water to find fitness and healing. She was educated at San Jose State University where she starred on the track and field team during its golden years.

Prehab: Rehabilitation Prior to Surgery
Let’s say your hip has been bothering you for over six months and now you realize you need to get serious about interviewing some doctors and making a choice as to whose opinion and suggestion you wish to follow. If you are still active in sports and recreational activities, you’ll probably want to save as much of your hip as possible and search out doctors who perform hip arthroscopy and femoral head resurfacing. You may be a candidate for these newer surgeries and you may not. To learn more about these two new surgeries as well as femoral acetabular impingement (FAI), go to hiphelp.com. Whatever you learn, whoever you choose to do your surgery, you’ll want to get in shape for surgery.
I once worked with a three-time Olympic track athlete who told me, “I trained as hard for that surgery as I did for the Games.” And she meant it. She worked out two to four hours every day, just as she had when getting ready for Olympic competition. She knew that undergoing surgery would mean a loss of fitness and strength not only because of the pre-meditated trauma to the body but also because she would be unable to train at her usual level for many weeks following the surgery. So she got to work reaching her peak fitness level prior to surgery since she knew a negative slump was certain to follow.
Many patients routinely participate in prehab programs to better help their bodies cope with the stresses of surgery. You, too, can benefit from such a plan. The fitter you enter the operating room, the quicker you’ll return to your sports and daily activities.
If your hip pain is accompanied by dysfunction and limited range of motion, you’ll want to do your prehab in a pool. Here’s why: by taking the weight off your hip, you can run, powerwalk, and do other high-intensity moves in deep water. That means you can keep your cardiovascular fitness even if you’ve had to give up running, hiking, and biking on land. Your hip will move more freely in the buoyancy of water. And the water’s resistance provides you with a chance to strengthen the muscles surrounding your hip through all planes of motion.
See Hip Circles below, a great exercise for regaining mobility and strength in your hip. You may perform a much small circle, depending on your hip, and if you have lower back pain, don’t reach so far to the rear.



Lynda Huey, M.S., founder of CompletePT and Huey’s Athletic Network, is a former athlete and coach whose own injuries led her into the water to find fitness and healing. She was educated at San Jose State University where she starred on the track and field team during its golden years.
Sport-Specific Waterpower Workouts
If you want to run fast, you have to run fast. If you want to kick hard, you have to kick hard. No matter what the sport, sooner or later you must approach full speed, full strength, full distance in your training. High-speed, high-impact, or long-distance repetitions often cause injuries, so athletes and coaches walk a fine line when scheduling workout and rest periods. They must find a way to complete the necessary training without crossing the line into overtraining. They must reach and sustain high velocity without overstressing the speed mechanisms. They must learn to recruit the maximum number of muscle fibers for top strength without straining fragile connective tissue.
On land, such high-level training is limited. Only a few precision sprints can be performed before fatigue endangers the sprinter. Only a dozen or so long kicks can send the football through the uprights before the kicker’s leg must be protected. But in the water, athletes can run, jump and kick over and over again without fear of injury. Thus water training has become standard practice in the training of elite athletes, and recreational athletes have learned to follow their lead.
You can focus on speed and anaerobic capacity by adding sprints in elbow-deep water to your fitness program. Try sprinting in place for 45 seconds, then resting for 45 seconds. Do four to six sprints, depending on your fitness level. Check your heart rate after the third one. You should have reached your maximum working heart rate by then.
You can work on sports technique by performing the same moves in water that you make on land. Of course the moves will be slower because of the water’s resistance, but they will be effective nonetheless, for these extra seconds per move allow you to feel your body parts in “freeze frame,” which gives you more time for feedback to correct the motions. For example, you can take an old tennis racquet into the pool (one you don’t care if you ruin), and swing it through some forehand and backhand strokes to iron out any glitches you’d like to correct.
In the water, you can teach your body to assume your sport’s key positions that are difficult to reach on land. For instance, if it’s hard for you to bend low enough when digging a volleyball or hitting a kill shot in racquetball, practice the perfect form in the buoyancy of water until your body learns the “feel” of the correct position. You’ll be able to do more repetitions in water without overstressing your knees, and you’ll add grace to your movement.
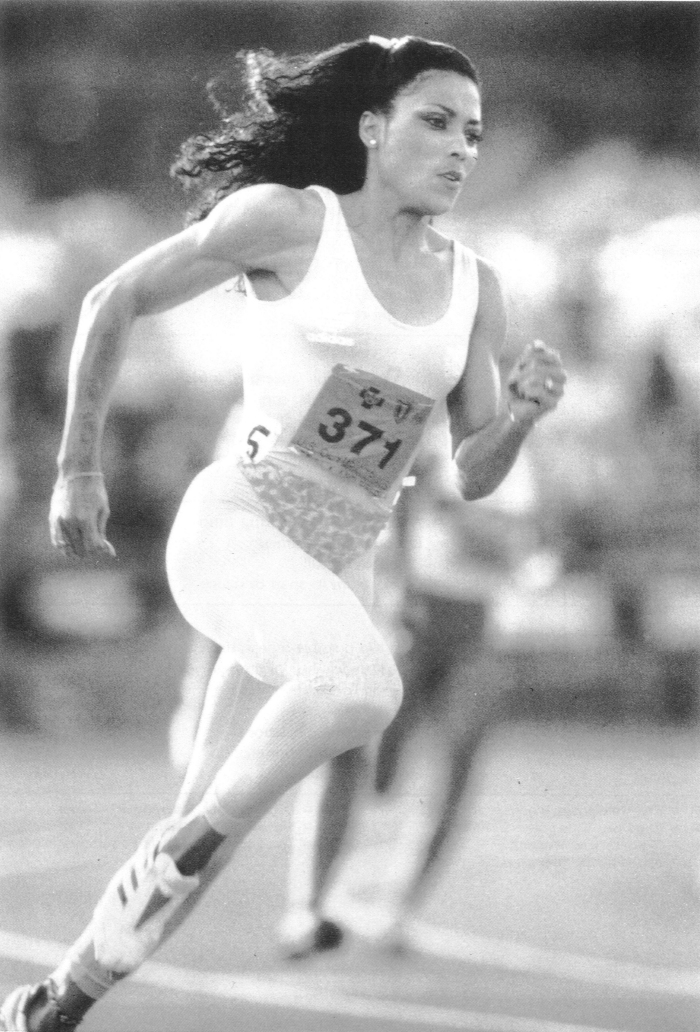
Florence Griffith Joyner was one of many Olympic sprinters who benefited from Lynda Huey’s pool sprinting program. These programs helped define aquatic physical therapy as we know it today.
Lynda Huey, M.S., founder of CompletePT and Huey’s Athletic Network, is a former athlete and coach whose own injuries led her into the water to find fitness and healing. She was educated at San Jose State University where she starred on the track and field team during its golden years.
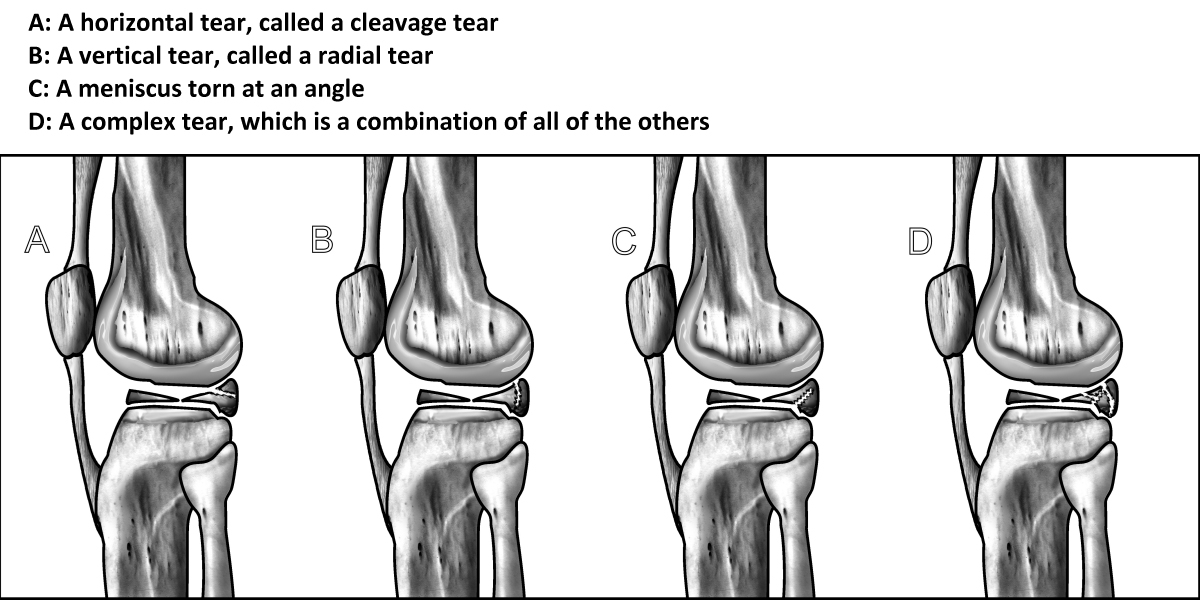
How to Prevent Knee Surgery for a Meniscus Tear
If your doctor just told you that you have a torn meniscus and you need knee arthroscopy, you may decide you want to do more research before going straight into the operating room. What to do about a meniscus tear depends on the kind of tear, the location of the tear, and the quality of the meniscus that is left. The illustration shows the most common types of meniscal tears. Learning more about your injury can help you choose the wisest path for recovery.
If you are under forty, most doctors will surgically repair the meniscus, whereas if you are over forty, you would probably best be served by two other alternatives:
Surgically trimming away and vacuuming out the torn part of the meniscus and leaving behind as much of the functioning meniscus as possible
Beginning an aquatic physical therapy or pool program designed to protect the torn meniscus while strengthening the muscles surrounding the knee
How can a pool program help you with your knee? Here’s the theory: Imagine the torn meniscus is like a blister in the palm of your hand. If you clipped a hundred roses in your back yard, you hand would hurt and you would see that the skin is torn. What is the treatment? If you gently and carefully continue to clip roses, the blister will become a callus. That’s how the pool exercises work on a torn meniscus. What was sore, vulnerable tissue turns into protected, callus-like tissue.
Doing our pool physical therapy program allows you to unload your weight and take the stress off your knee joint while you strengthen your muscles in an environment of weightlessness. As your muscles surrounding the knee joint become stronger and more able to stabilize your sore knee, they become better shock absorbers in preventing the stress from going through the joint. Nothing on land duplicates this. If you tried a muscle-strengthening program on land, you would be damaging the meniscus further, but in the pool, you’re unloading the joint at the same time you are placing resistance on the muscles.
After several months of the pool program, you will find that with every step you take, your muscles take more of the stress off the joint and fewer aggravating forces go through your knee. You may live happily-ever-after with an MRI that shows a meniscus not exactly the way it was before, just as your hand with a callus will look different from normal skin. But if it doesn’t hurt anymore, you’re not doing any damage. So consider doing the pool program, making your pain go away, and staying ahead of the game.
Lynda Huey, M.S., founder of CompletePT and Huey’s Athletic Network, is a former athlete and coach whose own injuries led her into the water to find fitness and healing. She was educated at San Jose State University where she starred on the track and field team during its golden years.
September 24, 2014
Aquatic Therapy Symposium in Brazil
The three previous times I went to South America, I changed planes or spent the night in Miami. This time I was pleased to see there was a 12-hour, non-stop flight from Los Angeles to Sao Paulo. I took it. Physical therapist Douglas Gil met me at the airport and as we drove into town, he explained with great pride that the regulatory body of physical therapy in Brazil had just the previous week estblished a new ruling that anyone who practiced aquatic therapy would first have to pass an exam and become a certified aquatic therapist. Douglas had been part of the group lobbying to make this change, so he was very pleased with that outcome.
The next day was gorgeous, and Douglas took me to Sao Paulo Park, the equivalent of New York’s Central park, albeit a bit smaller with very different vegetation. I was stunned by the immensity of the city. It was as though someone took a dozen Manhattans and jammed them next to one other – it was high rises and high rises as far as we could see and as far as we drove. The park was lovely with black swans in the lake and a mesmerizing fountain that kept changing its configuration of water sprays. I watched and took photos for nearly ten minutes and never saw the same thing twice.




Douglas was an incredibly gracious host throughout my visit. He had told me of his unique pool that curved along the outside of the city’s soccer stadium. But I hadn’t realized what an incredible jewel his Instituto Vita would be until I saw it for myself. What luxury! It reminded me of the old days of physical therapy when we were well paid by insurance companies and we could easily be profitable, which meant we could have lots of “extras.” They handed out plush towels and bathrobes to all those going into the pool. Lucky me, I was one of them. I went into his 93-degree pool for my own workout. The slippery tile on the bottom of the pool surprised me, but I would see throughout my trip that every single pool I visited in Brazil had a slippery tile bottom surface, unlike the plaster bottoms here in the U.S., which provide good traction. Also like the other pools I visited, they had an excess of overly shallow water that wasn’t even up to waist level, which wasted valuable space in the pool and was would go unused except by small children. (For most plyometric exercises, we make sure everyone is working in mid-chest-deep water.) The last 10-15 feet and the end of the pool was deep, which made me happy. I’ve learned that over half of the benefit of pool therapy comes from taking the weight off the knees, hips, back, legs, and feet so they can heal while fitness is gained or maintained.



Douglas took me to lunch at the nearby café, which must be fantastic for all those who work there. Great, fast, buffet with lots of variety. I tried quail eggs for the first time and loved them. Although I can fumble along in French and Italian, I don’t know much Portuguese, and although I tried, not much of it would stick. So Douglas connected me with doctors and therapists who spoke English so that I could chat with them. I learned the history of the clinic. Sixteen of the top orthopedic doctors in Sao Paulo got together and decided to create the best clinic ever. Douglas and one of the surgeons had known each other for years. When the doctor called Douglas and told him the idea, Douglas asked if there was going to be a pool. The doctor said no, to which Douglas replied, “Then it won’t be the best clinic ever!” They quickly altered the plans and squeezed in a pool around the track as seen in the photos. Douglas is in charge of the physical therapy and the doctors and therapists work in the same clinic taking great care of patients who might be trying to prevent orthopedic surgery, be preparing for surgery, or recovering from surgery. They afford the luxuries of this first-class facility by having mostly private paying patients, ones who pay for their care from their own pockets.
Douglas hadn’t intended to work that day, but when his patients started arriving and seeing him there, he began talking with them, and before long he was wearing his white coat and treating his patients. One of his female patients was a champion kick boxer. Douglas, as a gold medalist in judo at the 1987 Pan American Games, could help get her ready for competition. But over the weekend, she had broken her wrist and was there on a table wearing a cast.

The next day, Wednesday, we flew to Florianopolis, an island on Brazil’s East Coast. Physical therapist Romulo Brito met us there and took us to lunch. He and Douglas went over details of the Aquatic Therapy Symposium they had organized that would start on Friday at a local university. It was billed as the First International Aquatic Therapy Symposium. I think I was the international part.
Thursday was a sightseeing day with Lisianne Fabris, one of the many beautiful women of “Floripa” as the locals call it. It was astonishing to see so many stunning beauties everywhere you looked. Lisianne and I had planned to go body boarding that day. I had packed my wetsuit and fins. But rainy, cold weather stopped us. Instead Lisianne showed us her island. There’s a gorgeous fresh-water lagoon and overlook.

View from my hotel window. Rainy most mornings.

Lynda and Lisianne Fabris overlooking the large lagoon on Florianopolis.
We drove to the beach where we would have caught some waves if conditions had been better. Lovely, but nobody out surfing..

Joaquina Beach, Florianopolis
We drove around the island and stopped for lunch.

Even though I’d only met Lisianne that morning, I felt like I was on vacation with a long-time friend. She and Douglas and I crossed to the other side of the island where they wanted to show me the oyster farms. Douglas asked if I’d heard of Nostradamas. Of course! Well, he wanted to show me Osterdamas. “If you love oysters, this is the place you have to eat.” They showed me the oyster farms just off shore and said that every morning planes left that area with oysters for all of Brazil. Since he loved oysters, we stopped for him to eat some. Lisianne and I passed on the oysters and had dessert instead.


Friday came and the Symposium opened. All of the work by Lisianne, Romulo, Douglas, and others came to fruition. Dignitaries from the university gathered and gave speeches. Romulo and Lisianne turned the focus toward aquatic therapy, and then I gave the Grand Opening Address to 150 attendees. I used Douglas as my translator, but I could tell a few women in the front rows could speak English, because they would nod and smile as I spoke rather than having to wait to hear the translation.

I gave some background of what we learned from working with many of the world’s best athletes in water in the 1980s and 1990s – brief stories of Florence Griffith Joyner, Wilt Chamberlain, Willie Banks, Mike Powell, and Bo Jackson. Then I addressed the topic of preventing knee and hip surgery. In Brazil, the therapists hadn’t yet heard of the Finnish research study that showed that meniscus surgery may help no more than a fake operation. Physical therapy was the suggested alternative rather than having arthroscopic knee surgery. They had also not heard of the recent American study that concluded that over one-third of all total knee replacements done in America in the last five years were inappropriate based on patient surveys of their pain levels and ability to function. I taught them about deep-water prevention, prehab, or rehab for knees and hips – how we always hope to prevent the surgery, but if the problem doesn’t resolve, our work may turn into prehab for surgery. And in other cases, where patients come to us for the first time after they’ve already had surgery, we do the rehab starting in deep water where there is no weight bearing.
Later that evening, it was time to go to the pool. We used the diving well and the CompletePT flotation belts I brought with me to demonstrate deep-water interval training, deep-water exercises, and kick training.
Then we changed pools to have shallow, warmer water for the running and jumping (plyometric) exercises.



The next day, the seminar speakers would all be talking in Portuguese, so I took the day off and relaxed, walking along the water front, eating spectacular peanut butter ice cream, buying watermelon and papayas to eat throughout the day. The closing dinner was a traveling circus as we walked from one place to another trying to find somewhere that could accommodate 40 people for a last-minute dinner around 10pm. Yes, Brazil is like eating in Italy or Greece – very late at night.



We finished an all-you-can-eat sushi dinner around 1 am.
On Sunday we went to the airport to fly back to Sao Paulo. About six of us were on the same flight, and we waited together by the gate. A TV news program was about 20 yards away above everyone’s heads. I was facing the TV and Douglas had his back to it. Suddenly on the screen I saw a beautiful young woman in a wheelchair with a head rest. She was on the sidelines of a soccer game and a player came running over to her to kiss her. “Douglas!” I interrupted. “Is that the patient you were telling me about?” Douglas had told me the story of Lais Souza who was a two-time Olympic gymnast for Brazil. He had treated her for a torn labrum in her hip as well as after elbow and knee surgeries.

Since she was in her mid-twenties and old for a gymnast, she switched sports and made the 2012 Brazilian Olympic team in Freestyle Skiing (trick jumping, something fairly easy for a skilled gymnast). She had never seen snow until just about 6 months before she was to compete in the Winter Olympics. She was training in Park City, Utah, when she crashed into a tree and sustained severe traumatic injuries that left her unable to use her arms or legs. She was moved from Park City to Miami to obtain the best care for the spinal cord injury. Douglas flew there to help her in the pool.


Douglas ran over to the TV monitor and watched the rest of the broadcast. Yes, it was his patient Lais Souza as seen in the photos above.
Monday was my final day in Brazil before taking a red-eye flight back to L.A. Rosane Caetano spoke excellent English and gave me a tour of SAGA, her aquatic therapy clinic, which has 3 pools. I taught Rosane’s staff the same deep-water intervals, deep-water exercises, and kicking series I had taught in Floripa.

Rosane arranged for me to visit the hospital where she had worked previously, AACD, a hospital for disabled children primarily, but where adults were also being treated with physical therapy, aquatic therapy, occupational therapy, and many other treatments. We were allowed to observe a 13-year-old girl with cerebral palsy as she was taken through a LOKOMAT treatment – an amazing high-tech machine with body harness and a treadmill plus mechanical legs that force the patient’s own legs to move in time to a rhythmic, mechanical cadence while the patient watches a virtual walk through the park for biofeedback.
I got to observe rush hour in Sao Paulo first hand as Douglas drove me to the airport. It was very similar to rush hour in L.A. We got there right on time and I relaxed knowing that since I was on American Airlines, I would be back in the USA the moment I stepped onto the plane.
Lynda Huey, M.S., founder of CompletePT Pool & Land Physical Therapy and Huey’s Athletic Network, was a member of Wilt’s Wonder Women. She has cross trained many of the world’s best athletes in water from track and field, basketball, baseball, tennis, ice hockey and other sports. Lynda, an international speaker, is the author of four books on water exercise and water rehabilitation.
She has licensed her pool protocols to major health care providers, and her training methods will soon be available online at LyndaHuey.com.
To sign up for Lynda’s free monthly newsletter with video of pool exercises you can use right now, go to LyndaHuey.com.


