
On the Diagnostic Manual in Psychiatry (Part 1/3)
Hello my children, and nearly every one of you is young enough to be my child; otherwise if you are too old you are not interested in what I have to say. And I think of you all as my kids who want to learn; I take it as a sacred trust to fulfill that need. I am also sure that many of you have an expertise where I could learn. We are all smart in different ways. Anyway, I print the above from Time Magazine (March 2012) about the new DSM manual, now as thick as the Manhattan Telephone Book, to explain why this is nonsense and the field of psychiatry/psychology is bankrupt. It has left science behind; well, not exactly. It has addressed science through the new machines such as the MRI, but it is cloistered away from the actual practice of therapy. And never the twain shall meet. MRI results never tell us how to do psychotherapy; they tell us what drugs to give or not give. They tell us more about our neurons in the brain but not what causes them to act the way they do. We take their actions as a given and go from there, very much like Freud’s Id. We need to know why cortical neurons are sometimes hyperactive, not just how do we slow them down. There is a whole system encapsulating behavior, not just something that stands alone without any background information, nor any interrelationship to other parts of us. We are just “behaving” and the cognitivists/behaviorists say our task is only to change it. Such a mechanical view of complex human beings.
Look at the above Time description and then multiply it by hundreds of pages to understand the garden variety of neuroses. It is literally mind boggling. What it does, as you see, is list behaviors; and the field is captivated by the behaviorists who never see underlying motivations, who count this or that behavior as a disease. Eat too much? Bulimia. Eat not enough? Anorexia. How to define this? By behavior. The behaviorists hold sway in the field today. What you see is what you get; you look for the problem, you see behavior. You look for the answer and you see behavior. You look for progress, you look at behavior, and never, never look deeper. So in their scheme of treatment a certain number of weeks of feeling down puts you in the pathological category called depression. And, the insurance will pay for this therapy category, for a very brief time only. I imagine if you were required to to be depressed for 25 weeks before we could diagnose you as depressed you would get grief from the insurance companies. It all has to be brief; and therefore we are obliged to shorten our therapy accordingly.
Giving fancy names to psychiatric disorders does not make it scientific; it just makes it complicated. And when you rely on lists of names instead of feelings you see how complicated it gets.
All this has to be complicated because when you leave the arena of feelings and travel to the disconnected neocortex you have ever-widening verbiage with less and less sense. You arrive at an intellectual never-never land. I guess the whole idea is to make it so complicated; that no layman can understand it, therefore it has the patina of something really “scientific.” Look, I have two advanced degrees, have been in practice for 60 years and I cannot understand it. It is just mystifying. What compels all these names, diagnoses and lists is the behaviorist belief that behavior alone accounts for afflictions. And since behavior is as broad as the entire human condition, imagine the difficulty in diagnosis. They have built themselves a trap: they define in terms of behavior and then have to list almost all behaviors in terms of neurosis or not. Whew!! Let’s see, now I have to count how many months someone has been hypomanic to see if she qualifies for my concocted diagnosis. More important, to see if she qualifies for money. The diagnosis has to fit, not science, but finance.
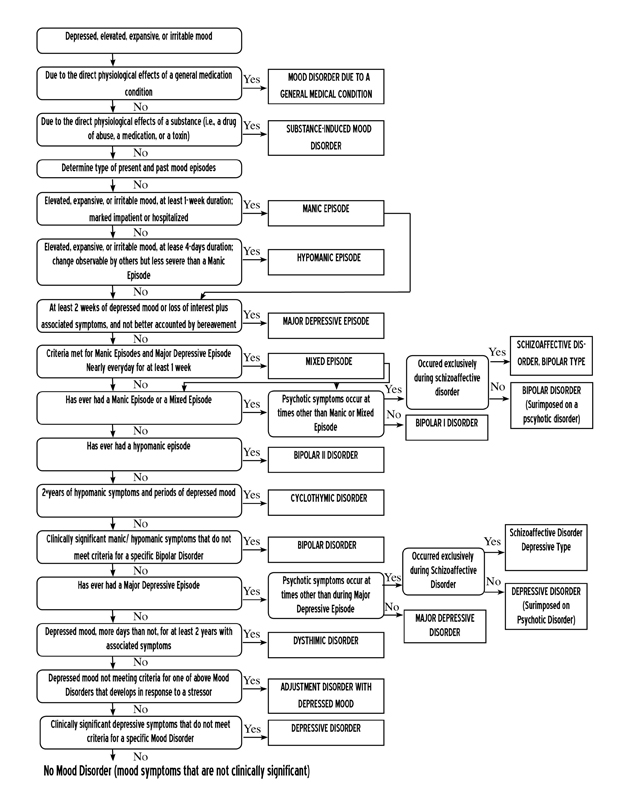
So in the category, Expansive Irritable Mood, it needs to go on for days to earn the diagnosis. Now who decided that? What about 3 days or six days? What they conflate is average with normal. The average period is about 4 days; ergo, the diagnosis is for those who suffer for four days. Below or above can be normal. If I don’t eat hardly at all for six days you are anorexic, but if only 3 days you are normal. You see the trap in counting the days. How about the forces that drive all that? Examine the fear of elevators. I have treated dozens of these cases, and the generating source is most often a post-birth trauma of being enclosed in an incubator just after birth. `The terror of being enclosed all alone with no kind and warm human contact is imprinted at the time and remains embedded in the system. Anything later that can trigger the memory (resonance) can set off the original terror and the phobia. So why dance around the behavior instead of going to the source? Because the source is never recognized, particularly with cognitive/behavior therapists who have no place for generating sources in their psychiatric schemata. Their theory does not allow it. “Stay on the surface” is their motto, and they do. Can anything be more spurious? We have a whole history of experiences that could help us understand who we are now and it is all ignored. They only want to correct behavior, which is the modus operandi of the Behaviorists. Only correct what we can see. What we cannot see is forgotten.
You see the patient has to recount to the doctor whether something is mildly annoying or really terribly debilitating so she can note the depth of the probelm. I have an article before me written by a patient who was anxious for years and never knew it. Why would they do in this case with our diagnosis? She was only mildly aware. So is she severely neurotic? Look at the obsessive-compulsive disorder. I have treated many who suffer from it. Often there is imprinted terror down deep in the brain that underlies it. It surfaces as, “If I try the doorknob twenty times I will be safe.” It has little to do with a doorknob and more to do with underlying terror that drives the search for trying to feel safe. If you ignore the underlying force you need to make a list, many lists, because one key feeling can drive multiple behaviors.
Are you compelled to try the door five times a day or twenty? If twenty you are obsessive. If five??? If even once you are still compelled to try the doorknob to feel safe and that is the underlying motivation, and if you have to do it everyday, I offer you my diagnosis—compulsive. If the generating source is ignored you have to spin a diagnosis that is off in intellectual never-never land. Let’ s see, I go to my office, see a patient, and then I have to count her number of episodes. And then I have to take her word if it is annoying or not. Yes, I refer her first for an MRI, magnetic resonance, and it comes back "agitation in the amygdala," now what? Is there someone who will connect the two (the MRI and the patient’s complaint) from a comprehensive diagnostic point of view? Will it dictate the therapy we do? Doubtful. Each specialist is off on their own. I have an MRI that shows what happens in the brain when I am compulsive but who notes that there is underlying terror and why? And above all, what to do about it? For that we need an overarching theory that encompasses theory and therapy so that one informs the other.
The behaviorists are caught in a trap.They have to decide on a diagnosis based only what they can see. So four days of one behavior makes it a disease but three days does not. And you need to be depressed for at least one week to qualify; and for what? To get paid by the insurance companies for a disease called depression. And it is now called a disease, not because of scientific input, but because of money to be paid. Here the insurance companies and the psychiatric profession are imbricated and merge into a financial arrangement that suits both well. Behaviorism pays and it helps the insurance companies lower their payouts: brilliant! Everyone should be happy—except the patient. Doctors will correct your behavior and your ideas until you reach what they decide is normal, and voila!, success. We have become willing tools of the insurance companies whose key role is to keep costs down; and too, of the psychiatric establishment who has a financial incentive to find quick ways to treat, with diagnoses that lend themselves to quick fixes. And what are the costs? Us. The quicker the cure, by their definition, the quicker the end of therapy. This obviates feeling therapies that do not lend themselves to quick fixes. The problems are more long-standing, deeper and more remote. So we accommodate to the companies through specious diagnoses and rearrange our treatment modes. And then we really believe that we are dealing with real biologic states. We are really dealing with financial states with a veneer of psychiatric lingo. Did I say that the APA brings in millions of dollars through the world-wide sales of the manual? This is really where finance, politics and psychiatry meld into one. The APA hired a Pentagon spokesman to defend their work, as if it were a matter of promotion and influence, not science. Maybe it really is indefensible. And maybe it has to be promoted just because it is scientifically indefensible. And maybe scientists were not engaged to explain it because it cannot be explained within the realm of science. If it were clear and solid science it would not have to be "promoted."



No comments have been added yet.
Arthur Janov's Blog

- Arthur Janov's profile
- 63 followers
Arthur Janov isn't a Goodreads Author
(yet),
but they
do have a blog,
so here are some recent posts imported from
their feed.

