
Jeffrey Dach's Blog, page 11
September 23, 2021
Vaccinoffee, A \/@ccine with Every Coffee
 Vaccinoffee, A \/@ccine with Every Coffee
Vaccinoffee, A \/@ccine with Every Coffee
In the year 2027, a string of coffee shops in New York City became wildly successful after offering a vaccination with every double expresso. Years ago, the Covid vaccine passed into extinction along with all the old viruses. Instead, we now have new viruses, 365 of them, and the drug industry has invented 365 new vaccines for various scary diseases hyped incessantly in the media. And in order to maintain a valid vaccine passport, one must receive a different vaccination each day for 365 days. How convenient can this be? The waitress jabs your arm as she brings your morning coffee. Started by a 22 year old college drop out entrepreneur, named Seymour Smucklinberger, his brainstorm was called ” Vaccinoffee”. After going nation wide, the business was acquired in a leveraged buy out by Amazon making Seymour the youngest billionaire in New Jersey.
Once acquired by Amazon, the Vaccinoffee coffee shops expanded further, now offering PCR testing and antibody testing for the 365 new viral diseases. A large machine at the front of the store validated your Vaccine Passport, and at the same time, video cameras used facial recognition software to alert local police of your location, should you have any outstanding “violations”.
The 365 vaccines were incredibly safe, and no adverse reactions were ever recorded. Heart attacks and strokes in the patrons were quite common in the Vaccinoffee shops, not causally related to the vaccine of course, explained as merely a coincidence.
In 2028, a rebel leader by the name of William Ashbury along with a large following on social media denounced the 365 vaccination program as a fraudulent program to enslave the population, and large unruly mobs of thugs dressed in black rioted in every major city targeting the Vaccinoffee shops. Thousands were arrested and held in prison indefinitely. It was somehow leaked that William Ashbury was an FBI operative, which explained why he was never arrested, searched or indicted.
The next great billionaire enterpreneur made his fortune by selling breakfast cereal with a ready to use vaccine in each box, calling them Cheery-Vax and Wheaty-Vax. Not to be out-done, fast food franchises added vaccines to each menu item, thus the Double Cheeseburger-Vax was born. It was not uncommon for every citizen to have a vaccine with every meal, breakfast lunch and dinner, organic of course.
People started complaining about difficulty getting all the vaccines every day. It seems there just wasn’t enough time in the day to get them all, and then have the mandatory meetings twice a day at work discussing the virtues of vaccines. All employers were mandated to have “Vaccine Virtue Breaks”. During this time, people were encouraged to talk among themselves about the wonders of vaccines, the greatest medical invention in history. It was not uncommon for people to start crying for joy and gratitude, and to take up a collection for the less fortunate.
The unvaccinated were considered an abhorrent disease ridden enemy. Any contact with an unvaccinated person must be immediately reported to the “Vaccine Police” who then do “contact tracing” of all associated people. Facial recognition software and GPS tracking is used to its full extent. The citizen must then undergo decontamination, a lengthy and expensive process which takes weeks or months to complete.
In the year 2027, the average citizen was happy with this new world of Vacinoffeee shops and Vaccine Passports, and wondered why people didn’t always do it this way?
This is The End
This has been a science fiction essay in the future year 2027. any resemblance to people, things or events is purely a coincidence and unintentional. This fictional essay by the author and is copyrighted 2021 and is protected as Free Speech by the Second Amendment of the Constitution. Comments may be entered below. Any nasty comments will be reported to the “thought police”.
Jeffrey Dach MD
7450 Griffin Road Suite 180/190
Davie, Florida 33314
954 792-4663
header image courtesy of wikimedia commons
Published on September 23rd, 2021 by Jeffrey Dach MD
The post Vaccinoffee, A \/@ccine with Every Coffee appeared first on Jeffrey Dach MD.


September 17, 2021
FDA Director Marion Gruber Battles Over Boosters
 FDA Director Marion Gruber Battles Over Boosters
FDA Director Marion Gruber Battles Over Boosters
Marion Gruber, director of the FDA’s Office of Vaccines Research & Review, and deputy director Phil Krause are both resigning in the fall over a dispute about Booster Shots. Political Appointees at the White House, with no background, or knowledge in medicine, virology or science have called for a Booster Vaccine rollout, meaning a third dose of the Pfizer or Moderna vaccine eight months after the initial two doses. To matters even worse, these “political appointees” have announced this Booster Program Rollout with no actual data to support this decision, completely bypassing the FDA’ s important function of “Protecting the American People” . The fact two high ranking FDA officials are jumping ship suggests an imminent mutiny within the ranks of the FDA, with various outside advisors joining in.
Lancet Article Opposed to Boosters
Joined by 16 other authors, both Drs. Gruber and Krause penned a recent Lancet article voicing their opposition to a Covid-19 Booster program, citing various reasons such as increased risk of myocarditis, and Guillain-Barre syndrome (a neurological disorder causing paralysis), and lack of clear data indicating Boosters are needed. They opine that if such adverse events were to occur, the public outrage and backlash could derail not only the COVID vaccine program, but also place the entire childhood vaccination program at risk. Drs Krause and Gruber write in The Lancet (2021):
Although the benefits of primary COVID-19 vaccination clearly outweigh the risks, there could be risks if boosters are widely introduced too soon, or too frequently, especially with vaccines that can have immune-mediated side-effects (such as myocarditis, which is more common after the second dose of some mRNA vaccines, or Guillain-Barre syndrome, which has been associated with adenovirus-vectored COVID-19 vaccines). If unnecessary boosting causes significant adverse reactions, there could be implications for vaccine acceptance that go beyond COVID-19 vaccines. Thus, widespread boosting should be undertaken only if there is clear evidence that it is appropriate. . . . Current evidence does not appear to show a need for boosting in the general population, in which efficacy against severe disease remains high. Even if humoral immunity appears to wane, reductions in neutralizing antibody titre do not necessarily predict reductions in vaccine efficacy over time, and reductions in vaccine efficacy against mild disease do not necessarily predict reductions in the (typically higher) efficacy against severe disease.(1) end quote
Australia Health Minister Dr Kerry Chant
Rather than agonize over the Booster decision, Dr Kerry Chant the South Wales Minister of Health (Australia) is more straight forward and blunt with her public announcement that, yes there will be Boosters. The esteemed doctor publicly stated at a 8/29/21 press conference: :
“Booster doses and repeat doses will be part of it….I can assure you that the commonwealth government has purchased large quantities of vaccine into 2022 and this will be a regular cycle of vaccination and revaccination as we learn more about when immunity wanes…(people) will be getting vaccinated regularly (against COVID.)”(2)
Israel Booster Roll Out, Get Ready for Fourth Dose
Meanwhile, July 29, 2021 the Israeli Prime Minister Naftali Bennet had already announced their Booster Program with the Pfizer vaccine, and as of one month later on August 29, 2021, over 2.5 million Israelis had received the Booster (third dose). A study showing efficacy of the Booster shot has already been published. (3) At about this same time, Prof. Salman Zarka, Israel’s COVID-19 “virus czar”, announced that Israelis should prepare for another (second) booster, the fourth dose of the Pfizer COVID-19 vaccine, as he is already predicting failure of the third booster shot. (4)
FDA Advisory Panel Votes Against Booster For All, OK for over 65 or high risk for disease.
9/17/21: The FDA Advisory panel voted against The White House Booster Program rollout for everyone, instead restricting Booster Shots to the over 65, and high risk patients. (5)
One might ask, where is the vaccine safety board? And where are the monthly press briefings on vaccine safety ? There aren’t any.
Conclusion: The need for repeated Booster doses of a vaccine is an obvious admission of vaccine failure. As mutiny spreads through the FDA, the “Battle Over the Boosters” is just heating up. Will the “vaccine hesitant” exercise even more caution with a vaccine program that is more and more resembling a runaway train with nobody at the controls?
=================================================
Vaccines and Related Biological Products Advisory Committee – 9/17/2021
Jeffrey Dach MD
7450 Griffin Road Suite 180/190
Davie, Fl 33314
954-792-4663
Links and References
Header Image Courtesy of Wikimedia Commons
1) Krause, Philip, et al. “Considerations in Boosting COVID Vaccine Immune Responses.” (2021). Lancet, Sept 13, 2021.
2) Dr Kerry Chant Press Briefing on Twitter
3) Bar-On, Yinon M., et al. “BNT162b2 vaccine booster dose protection: A nationwide study from Israel.” medRxiv (2021).
4) Virus czar calls to begin readying for eventual 4th vaccine dose. Salman Zarka says COVID-19 is here to stay for and that next booster shot may be adjusted for variants: ‘This is our life from now on, in waves’ By TOI staff 4 September 2021, 6:38 pm Times of IsraelThis weekend Prof. Salman Zarka, Israel’s COVID-19 health czar, “called for the country” to prepare for their “fourth doses of the” Pfizer COVID-19 vaccine, as the third booster shot is already predicted to fail.
5) By ABC News, Associated Press, CNN
FDA panel backs Covid booster shots only for elderly, at-risk
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
www.drdach.com
Heart Book by Jeffrey Dach
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Copyright (c) 2021 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Published on September 17th, 2021 by Jeffrey Dach MD
The post FDA Director Marion Gruber Battles Over Boosters appeared first on Jeffrey Dach MD.
September 15, 2021
Povidone Iodine Mouth Wash, Rinse, Gargle for C0\/lD Prevention
 Povidone Iodine Mouth Wash, Rinse, Gargle for C0\/lD Prevention
Povidone Iodine Mouth Wash, Rinse, Gargle for C0\/lD Prevention
by Jeffrey Dach MD
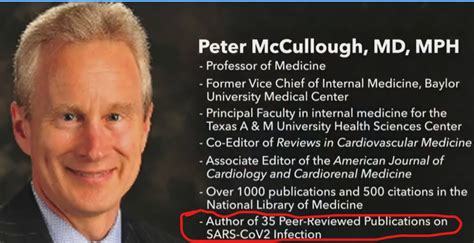
Dr. McCullough, in this interview with Peter Breggin MD (author of Talking Back to Prozac) discusses the routine use of dilute (1%) Povidone Iodine mouth wash in the dental office as an excellent preventive measure for Covid-19.
10% Povidone Iodine is available OTC (Over the Counter) without a prescription at any drug store for a few dollars.
Note: This 10% Povidone Iodine must be diluted to 1% strength before use as a mouth wash, otherwise it is too strong and irritating. Dilute by adding 2-3 drops of the 10% Povidone Iodine into a full glass of water. Now it is dilute enough to use as a mouth rinse, or gargle.
Dr. McCullough recommends routine use of this mouthwash on a daily basis, and especially after contact with large indoor groups.
See this Sept 14, 2021 Dr Peter Breggin Interview with Dr Peter McCullough on Brighteon discussing Covid, vaccines, early treatment, prevention with Povidone Iodine mouth wash etc:
Jeffrey Dach MD
Articles with Related Interest:
Peter McCullough on Early Treatment vs. Vaccination
The Covid Vaccine is Safe and Effective?
CDC Director Rochelle Walensky Warns of ADE Antibody Dependent Enhancement
Ivermectin for Covid and the Failure of American Medicine
Ivermectin Anti-Cancer Anti-Parasitic Wonder Drug
Jeffrey Dach MD
7450 Griffin Road, Suite 180/190
Davie, Florida 33314
954-792-4663
References and Links
Goldstein, Leo. “Oronasal Hygiene with PVP-I for COVID19.” (2021).
https://link.springer.com/article/10....
Arefin, Mostafa Kamal, et al. “Virucidal effect of povidone iodine on COVID-19 in the nasopharynx: an open-label randomized clinical trial.” Indian Journal of Otolaryngology and Head & Neck Surgery (2021): 1-5.
Maurya, Raj Kumar, et al. “Povidone-iodine preprocedural rinse—An evidence-based, second-line defense against severe acute respiratory coronavirus virus 2 (SARS-CoV-2) in dental healthcare.” Infection Control & Hospital Epidemiology (2021): 1-2.
Mohebbi, Simin Z., Tayebe Ebrahimi, and Ahmad Reza Shamshiri. “Do Mouthwashes Reduce Covid-19 Viral Load during Dental Procedures and Oropharyngeal Examinations? A Systematic Review.” (2021).
Ebrahimi, Tayebe, Ahmadreza SHamshiri, and Simin Z. Mohebbi. “Do mouthwashes reduce covid-19 viral load during dental procedure and oropharynge-al examination? A systematic review.” (2021).
Tadakamadla, Jyothi, et al. “In vitro studies evaluating the efficacy of mouth rinses on Sars-Cov-2: a systematic review.” Journal of Infection and Public Health (2021).
https://www.ncbi.nlm.nih.gov/pmc/arti...
Moreno, María Victoria Mateos, et al. “ORAL ANTISEPTICS AGAINST CORONAVIRUS: IN VITRO AND CLINICAL EVIDENCE.” Journal of Hospital Infection (2021).
https://www.sciencedirect.com/science...
Chaudhary, Prem Prashant, et al. “Estimating salivary carriage of SARS-CoV2 in non-symptomatic individuals and efficacy of mouthwash in reducing viral load: a randomized controlled trial.” The Journal of the American Dental Association (2021).
https://www.ncbi.nlm.nih.gov/pmc/arti...
Hassandarvish, Pouya, et al. “In vitro virucidal activity of povidone iodine gargle and mouthwash against SARS-CoV-2: implications for dental practice.” British dental journal (2020): 1-4.
Introduction Virus particles in respiratory droplets and aerosols generated during medical/dental procedures are a potential source of SARS-CoV-2 cross infection. In the dental setting, oral decontamination could be an important adjunct to personal protective equipment and is recommended by a number of national COVID-19 guidance documents for dental settings.
Aim To assess the in vitrovirucidal activity of an oral povidone iodine (PVP-I) product against SARS-CoV-2.
Material and methods BETADINE gargle and mouthwash (1% PVP-I) was tested against SARS-CoV-2 virus under both clean and dirty conditions using a suspension assay based on EN14476 methodology. Virucidal activity of the product, undiluted and at 1:2 dilution, was tested at contact times of 15, 30 and 60 seconds. Viral titres were calculated using the Spearman-Kärber method and reported as median tissue culture infectious dose (TCID50/ml).
Results The undiluted product achieved >5 log10 reduction in viral titres compared to the control at 15, 30 and 60 seconds under both clean and dirty conditions. At a twofold dilution (0.5% PVP-I), the test product demonstrated >4 log10 kill at 15 seconds and >5 log10 kill at 30 and 60 seconds in both clean and dirty conditions.
Conclusion PVP-I gargle and mouthwash product, undiluted and at 1:2 dilution, demonstrated potent and rapid virucidal activity (≥4 log10 reduction of viral titre) in 15 seconds against SARS-CoV-2 in vitro. The PVP-I gargle and mouthwash product is widely available and could be readily integrated into infection control measures during dental treatment including pre-procedural oral decontamination.
https://www.ncbi.nlm.nih.gov/pmc/arti...
Bidra, Avinash S., et al. “Rapid in‐vitro inactivation of severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) using povidone‐iodine oral antiseptic rinse.” Journal of Prosthodontics 29.6 (2020): 529-533.
To investigate the optimal contact time and concentration for viricidal activity of oral preparation of povidone‐iodine (PVP‐I) against SARS‐CoV‐2 (‘corona virus’) to mitigate the risk and transmission of the virus in the dental practice.
Materials and Methods
The severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) USA‐WA1/2020 strain, virus stock was tested against oral antiseptic solutions consisting of aqueous povidone‐iodine (PVP‐I) as the sole active ingredient. The PVP‐I was tested at diluted concentrations of 0.5%, 1%, and 1.5%. Test media without any virus was added to 2 tubes of the compounds to serve as toxicity and neutralization controls. Ethanol (70%) was tested in parallel as a positive control, and water only as a negative control. The test solutions and virus were incubated at room temperature (22 ± 2 °C) for time periods of 15 and 30 seconds. The solution was then neutralized by a 1/10 dilution in minimum essential medium (MEM) 2% fetal bovine serum (FBS), 50 µg/mL gentamicin. Surviving virus from each sample was quantified by standard end‐point dilution assay and the log reduction value (LRV) of each compound compared to the negative (water) control was calculated.
Results
PVP‐I oral antiseptics at all tested concentrations of 0.5%, 1%, and 1.5%, completely inactivated SARS‐CoV‐2 within 15 seconds of contact. The 70% ethanol control group was unable to completely inactivate SARS‐CoV‐2 after 15 seconds of contact, but was able to inactivate the virus at 30 seconds of contact.
Conclusions
PVP‐I oral antiseptic preparations rapidly inactivated SARS‐CoV‐2 virus in vitro. The viricidal activity was present at the lowest concentration of 0.5 % PVP‐I and at the lowest contact time of 15 seconds. This important finding can justify the use of preprocedural oral rinsing with PVP‐I (for patients and health care providers) may be useful as an adjunct to personal protective equipment, for dental and surgical specialties during the COVID‐19 pandemic.
https://pubmed.ncbi.nlm.nih.gov/32520...
Frank, Samantha, et al. “Povidone-iodine use in sinonasal and oral cavities: a review of safety in the COVID-19 era.” Ear, Nose & Throat Journal 99.9 (2020): 586-593.
Objectives: Approaches to nasal and oral decontamination with povidone-iodine (PVP-I) have been published to reduce nosocomial spread of Severe Acute Respiratory Syndrome-Coronavirus 2 (SARS-CoV-2). The safety of PVP-I topically applied to the nasal and oral cavity is addressed by a literature review. The specific efficacy of PVP-I against coronaviruses and its potential efficacy against SARS-CoV-2 is discussed.
Methods: A review was performed utilizing PubMed and Cochrane Databases. All citations in protocols for nasal and oral PVP-I use regarding COVID-19 were independently reviewed.
Results: Povidone-iodine has been safely administered for up to 5 months in the nasal cavity and 6 months in the oral cavity. Concentrations less than 2.5% in vitro do not reduce ciliary beat frequency or cause pathological changes in ciliated nasal epithelium, upper respiratory, or mucosal cells. Adverse events with oral use have not been reported in conscious adults or children. Allergy and contact sensitivity is rare. Chronic mucosal use up to 5% has not been shown to result in clinical thyroid disease. PVP-I is rapidly virucidal and inactivates coronaviruses, including SARS-CoV and Middle East Respiratory Syndrome (MERS).
Conclusions: Povidone-iodine can safely be used in the nose at concentrations up to 1.25% and in the mouth at concentrations up to 2.5% for up to 5 months. Povidone-iodine rapidly inactivates coronaviruses, including SARS and MERS, when applied for as little as 15 seconds. There is optimism that PVP-I can inactivate SARS-CoV-2, but in vitro efficacy has not yet been demonstrated.
Published on September 15th, 2021 by Jeffrey Dach MD
The post Povidone Iodine Mouth Wash, Rinse, Gargle for C0\/lD Prevention appeared first on Jeffrey Dach MD.
September 2, 2021
Dr Peter McCullough on Early Treatment vs Vaccination
 Dr Peter McCullough on Early Treatment vs Vaccination
Dr Peter McCullough on Early Treatment vs Vaccination
The following is a Transcript of the Dr. Peter McCullough Interview Sept 2, 2021:
Dr. Peter McCullough Speaking:
I (Dr. Peter McCullough) am Professor of Medicine at Texas A and M College of Medicine for about 10 years. I am on the Baylor Dallas campus. I am in a private practice. and I maintain my board certification in Internal Medicine and Cardiology. I also lead a research team in downtown Dallas. When Covid-19 hit, I redirected all of my focus towards the pandemic. I recognized this was going to be a giant challenge for us. We have actually very few infectious disease doctors in the US, completely subscribe in the hospital. I am more of an outpatient oriented doctor. I poured all my efforts into scholarship on Covid 19 in the last year. In a sense I’ve done a self directed fellowship on infectious disease.
I have published the first treatment guidance on how to treat COVID 19 as an outpatient. These are the most widely utilized publications in all of COVID 19 in the world for outpatient treatment. I’ve been relied upon by the US Senate ti testify in the Senate, and to render my opinion.
I have been blessed to a regular contributor on FOX news almost every week now over the last several months. What kind of authority do I have to give any opinions about COVID 19 ? Before COVID, I was the most published person in my field in world history. My field is the interface between heart and kidney disease. How do these organs communicate with each other.
I am the editor in chief of CadioRenal Medicine. I am the editor in chief of Reviews in Cardiovascular Medicine. I have 600 peer reviews publications in the National Library of Medicine. I have lectured all over the world, the New York Academy of Sciences, NIH, FDA,
I am on the calling card of someone who has a position of authority in medicine.
I have over 45 publications on COVID 19.
I published the two sets of treatment guidance when no-one else would step up.
I have had the illness myself, and I have had serious cases in my family including fatalities.
I think as a single person, I probably have the most authority to give my opinion on what is going on in this pandemic, than any one in the world..
And I can tell you the problem with what Americans are seeing on TV right now is they are not seeing doctors like me working in teams of doctors and advising the country.
We are down to one or two people that are government officials, that people see on TV who by the way are not board certified, they don’t have qualifications for doing what they are doing right now. And as singular people, they are issuing, not recommendations, not guidance, they are issuing directives. and we are seeing these things come down over time. So we can tackle them one by one.
First off we should tackle five really important points.
When this first hit, no one knew what this virus was about, including myself. But we do have a year and three months later, we have a framework of understanding.
The first important point: The virus spreads from a sick person to a well person, period.
The virus does not spread from asymptomatic person to asymptomatic person. It took months to get these data. These are the two studies showing no asymptomatic spread, published in the best journals :
Cao, Shiyi, et al. “Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China.” Nature communications 11.1 (2020): 1-7.
Madewell, Zachary J., et al. “Household transmission of SARS-CoV-2: a systematic review and meta-analysis.” JAMA network open 3.12 (2020): e2031756-e2031756.
Madewell, Zachary J., et al. “Factors Associated With Household Transmission of SARS-CoV-2: An Updated Systematic Review and Meta-analysis.” JAMA Network Open 4.8 (2021): e2122240-e2122240.
Cheng, Hao-Yuan, et al. “Contact tracing assessment of COVID-19 transmission dynamics in Taiwan and risk at different exposure periods before and after symptom onset.” JAMA internal medicine 180.9 (2020): 1156-1163.
Zhang, Weiwei, et al. “Secondary transmission of coronavirus disease from presymptomatic persons, China.” Emerging infectious diseases 26.8 (2020): 1924.
Has the Evidence of Asymptomatic Spread of COVID-19 been Significantly Overstated?19 December 2020 / Updated 7 March 2021by Dr Clare Craig FRCPath and Jonathan Engler MBChB LLB
Gao, Ming, et al. “A study on infectivity of asymptomatic SARS-CoV-2 carriers.” Respiratory medicine 169 (2020): 106026.
Is there asymptomatic spread of COVID-19? Posted on August 7, 2021 by State of the Nation
The virus does not spread asymptomatically. If anybody in this room has the virus right now, but they have no symptoms, they cannot spread it to us, in fact they are forming their own immunity. Asymptomatic spread must be less than 1% of all spread.
(Note from Jeffrey Dach MD regarding asymptomatic transmission of COVID: Dr McCullough is quite correct in this. However, one must distinguish between the asymptomatic patient with a false positive COVID test who does not carry the virus and can not transmit to another vs. Pre-symptomatic transmission which is perhaps the most common mode of viral transmission from one person to the next. This is viral transmission from a pre-symptomatic person to another. In this case, for a brief period of time, a day or two prior to onset of viral symptoms, a carrier person may harbor a viral infection in the nasal passages which, although producing no symptoms in the carrier, can be transmissible to others. Symptoms will then start shortly, one to two days later. If the suspected pre-symptomatic carrier remains asymptomatic for the next week or so, then there never was any risk of transmitting the disease, and the person was not a carrier after all. End Added Note by jeffrey dach md ) (8-9)
Asymptomatic Testing Was Useless
OK because of that, that means that asymptomatic testing was completely useless. In the US we have had 35 million cases of COVID , we have actually burned 400 million COVID tests right now. Even the World Health Organization says June 25, Stop the Asymptomatic Testing. (CDC Aug 26: Asymptomatic People no longer require test)
All this nasal and oral testing was never approved for routine screening, it was never approved for people to get on airplanes, or any thing else, that was just an over reach.
Point number one: No Asymptomatic Spread.
Point number Two: Asymptomatic Testing is a complete waste of time. It is not FDA approved. It is not even advised by the WHO.
Point Three: Natural Immunity, once somebody has had the virus , is robust complete and durable. You can not get the virus twice.(1-3)
When grandmother had it last year , she is not going to get it again.
We have seen it sweep through the nursing homes. It is done. It is a one and done. There is this narrative, that people keep getting COVID over and over again. But when you ask people, they say: “No, I have had it and I am done”. One and DONE.
Cleveland Clinic Study
There has even been challenges where Cleveland Clinic published a study where people had recovered. (1) They went right back and worked with COVID right in their face . You can’t get it (the COVID virus ) again . So this idea its ONE and DONE, Natural Immunity is robust, complete and durable. This is very important. So if you have workers in your business who have had Covid, they don’t have to worry, they are not going to get it again.
There is incredible continuing fear, there are legal demands into the CDC to recognize Natural Immunity. Even Gov Abbott here in Texas, by Executive Order in April, has an EO, Natural Immunity, we recognize it in TEXAS by executive order.
The governor said his reason behind not issuing another mask mandate is due to people having “immunity to COVID through the vaccination or through their own exposure and recovery from it.(Natural Immunity)” 7/20/21 interview on KPRC 2 News at 5 Click2Houston.com
And (these naturally immune) people ask, “Do I have to take the Vaccine ?” Of course you don’t. You can not get it (COVID) a second time. That is the third point.
The fourth point is : The Covid-19 virus is treatable. That was our work. So we know now that we have an approach. People over 50 who have additional medical problems have a greater than one per cent chance of being hospitalized or dying. That is enough to treat. And we have treatment protocols that involve FDA approved (EUA approved) antibodies. I can make a phone call. Patients can go right down here to Baylor, get an antibody infusion free of charge. It is wonderful. The US government bought 500 million doses of these monoclonal antibodies, but there is no word of them. You don’t see them on TV , there is no 1-800 numbers. When people get their COVID test result, they are not told how to access these. (Access Your Free Monoclonal Antibody Infusion Here)
Your businesses and viewers should demand answers about antibody infusions. Call your hospital and say, listen, my grandmother is sick with COVID 19, and I want an antibody infusion. Now is the time to get activated because your government agencies are not helping you on early treatment.
We are busting the myth that COVID is not treatable. I am here to tell you it is treatable. The two key publications, I am the first author, American Journal of Medicine 2020, and the second article is Reviews in Cardiovascular Medicine 2020, these are the most cited and utilized , and relied upon papers for Early Treatment for COVID -19 in the world,
Patients over age 50 with multiple medical problems, that is the only group that really needs treatment. The younger person who presents with severe symptoms, they are a younger person with some problems like cyctic fibrosis sure, they could require treatment. But in general it is 25% of adults. Seniors ought to demand these monoclonal antibody infusions . President Trump got it.
After that, the drugs that work are used in combination and sequence, and they are based on a signal of benefit and acceptable safety. It is so early in the disease process, we don’t have proven efficacy and safety, we don’t. It is a signal of benefit and acceptable safety.
So what can be used (for Early Treatment of COvid-19) ?
Hydroxychloroquine use is supported by 200 studies. Countries like the US appropriately stockpiled it for a reason.
Ivermectin has 60 Supportive studies. We combine it with Doxycycline or Azithromycin.
Everybody can use an inhaler, Budesonide inhaler (Pulmocort). Richard Bartlett was the first to discover this in Texas. This was Proven in the UK in the STOIC TRIAL.
We can use oral prednisone on day 5 of pulmonary symptoms, much like an asthmatic would use it. Or someone with an allergic reaction condition would use it.
We use a Gout medication, for 30 days in high risk patients called Colchicine, one pill a day. This was proven in a large randomized trial from Montreal Heart Institute called Co-Corona Trial 4,000 pts.
Tardif, Jean-Claude, et al. “Colchicine for community-treated patients with COVID-19 (COLCORONA): a phase 3, randomised, double-blinded, adaptive, placebo-controlled, multicentre trial.” The Lancet Respiratory Medicine (2021).
We use Aspirin 325 mg per day because this virus is unique, it causes blood clots. It is the only viral infection we have ever seen that causes blood clotting, and that is what actually kills patients. So we use Aspirin as a blood thinner. It is a full adult dose. Higher risk patients we actually use Lovonox injections, like someone would get for the treatment of a clood clot.
Thats what is called sequenced multi-drug therapy. It is all done at home. Supported by the Association of the American Physicians and Surgeons. AAPSonline.org
Download the home AAPS Home Treatment Guide !!!! Be Ready. Click Here : AAPS Home Covid Patient Treatment Guide
It is also supported by another group in the United States.
The Front Line Critical Care Consortium (FLCCC). They have a little different set of protocols, but the principles are the same.
Now these are well in advance of the CDC, NIH or the FDA or the Infectious Disease Society of America that have yet to publish any outpatient treatment guidelines.
Why is that ? They have been focusing on in-patients (in the hospital). So one of the reasons I wanted to fill this void is: ” How many years are we going to wait and have Americans Suffer before they get any treatment at home (as outpatients)?
We can even order OXYGEN concentrators at home with a simple phone call. Because under the emergency use authorization, we can actually get them out to the home, and get people supplemental oxygen.
We have been so successful with this Early Treatment Protocol, we have an 85% reduction in risk of hospitalization and death. I have treated patients well into their 90’s and we have avoided the panic and fear, isolation of the hospital,
The contemporary mortality rate in the hospital right now if someone needs the ICU in the US, 38%, and that’s published by the STOP COVID Collaboration out of Harvard.
So point number four is: Covid is treatable, it takes about 4-6 drugs.
ADULTS WITH MILD CASES- 5 days
Average person our age, about 10 days.
Seniors, it could be about 30 days, a longer illness.
What about people under 50. They breeze through COVID.
A Neutraceutical bundle which is recommended for everybody, which is reasonable includes:
Zinc
Vitamin C
Vitamin D
Quercetin
If a Younger person develops symptoms, they can move into treatment. But only 25% of people who get COVID need early treatment. It helps them avoid the hospital or death. And younger people breeze through this.
COVID Vaccines
Point number 5 is the contentious issue of the vaccine, and I have rendered my opinion on this multiple times. The vaccines are brand new. In the US we have Pfizer, Moderna, and J and J. They are a brand new technology. They are nothing like a flu shot. They actually transfer genetic material inside our cells, and they cause our cells to make the spike protein. So , there is the ball, the nucleocapsid, and the little spines or spikes on the outside of the ball (the spike protein). The vaccines trick our body into making the spike protein, and then we form an immune reaction to it.
The short discussion on the vaccines is this: while half of Americans have taken them, for some individuals the vaccines have not worked out too well, in terms of being sufficiently safe for human use. Obviously, many tens of millions of Americans took it , they had a sore arm, they got through it just fine. People in my family took it. It is not a big deal if there are no complications. But for those who are getting complications, we are currently at as of today, CDC has told us, we are at 12,000 Americans that have died after the vaccine. 86% of the time independent reviewers have determined the vaccine caused the death. 50% of the deaths occur within 48 hours of the vaccine. 80% of the deaths occur within a week of the vaccine. And it is a modern day tragedy.
We have never had any medical product ever in the history of mankind result in 12,000 American deaths. We have 400,000 certified vaccines injuries right now due to the vaccine along the lines of neurological, cardiac, immunologic or hematologic abnormalities. That’s about the size of a medium sized city right now of people who have had vaccine injuries. So there is great concern as we move forward that the vaccines look like they don’t have a safety profile to be the solution to the problem.
What we know is that the number of deaths has exceeded the cumulative total reported into the data system for all time.
Just to give you an Idea, we have 70 (?) vaccines on the market, roughly 500 million shots . This year I had Shingles and Flu shots. Everyone gets vaccines. 500 million shots, 70 vaccines. The average annual deaths reported to the database was about 150 or so. On Jan 22, we were already at 186 for COVID 19 deaths, and we have already raced up to 12,000 deaths, an astronomical number.
Almost everybody knows somebody who either died or been injured with the vaccines now. People are talking, and Americans are worried that our federal officials have not come clean on safety. We have not had a press briefing on overall vaccine safety. Can you imagine that? We should be having probably weekly briefings or at least monthly briefings, because we want to make sure the program is safer. There may be certain people who shouldn’t get the vaccine. For instance: the COVID recovered. You can’t get COVID a second time. If they took the vaccine and they have already been revved up from the first infection, are they the people who are getting the complications? We don’t know because our agencies have not fairly disclosed this. Is it among diabetics ? Is it among patients with prior neurological disorders or cardiac disease? No one knows because our agencies, and this is a terrible word to say on the air, the correct word is “malfeasance”, it is wrongdoing by those in a position of authority. And so that is what we are having right now. Just like the the “Trusted News Service” is pre-stated censorship. We now have malfeasance by our government agencies on safety.
The second update on the vaccines is that while half of Americans have taken them, and we wish every single person well, we have deeply concerning reports now, out of the United Kingdom, and out of Israel that the vaccines are failing. And what I man by that, is the virus has mutated, and the current version is called Delta. That is our most recent version in the United States is now the predominant version. And the mutations are occurring because we are vaccinating.
There is a paper from the Mayo Clinic in Boston by Niessen and colleagues that have shown when we get to 25% of the population vaccinated, the virus starts to mutate, and escape the effect of the vaccine.
Niesen, Michiel, et al. “COVID-19 vaccines dampen genomic diversity of SARS-CoV-2: Unvaccinated patients exhibit more antigenic mutational variance.” medRxiv (2021).
So now the Delta variant has escaped the effect of , for sure, the Pfizer vaccine, because we know in Israel now, 80% of people who have had COVID in Israel right now have been fully vaccinated with Pfizer .
When the case is well defined, you have had COVID, you had the characteristic signs and symptoms, you had a positive PCR or antigen test, and the case is well defined, there has actually never been reported so far in the world, a second case,
Now, the difficulty is when the first case was not well defined. You didn’t get a test, or you are not really sure, there is a a lot of uncertainty, in an analysis by (?) Virtue and colleagues has done a meta-analysis of 11 studies, 615 thousand individuals, Even with the ill defined case in a population, and looked at a year later what happened, the risk of COVID was 0.2%
So what i am telling you is infinitesimally low , it is so low, that in my view, one doesn’t need to be worried about COVID 19.
I have had it myself. I don’t go through my day in fear. I could encounter a patient with COVID 19 and I know I cant get the virus. I know the vaccine can not benefit me. In fact the FDA, CDC, Moderna and J and J excluded people like you and me (recovered from previous COVID) from the clinical trials. They knew we couldn’t get COVID 19.
The registration for clinical trial had exclusion criteria: COVID recovered, suspected COVID recovered, pregnant women, women of child bearing potential, even people with positive antibodies . They were excluded because the FDA knew we could not benefit, and we would only be harmed by the vaccine . In fact, they were right. COVID recovered patients, in THREE STUDIES, Methudias, Rah and Kamer, have shown us that COVID recovered patients, when they take the vaccine, which they don’t need, they actually have higher side effects, including ending up with something serious ending up in the hospital. So, I have told America, a prior COVID infection is a contra-indication to get the vaccine. You should not get the vaccine. And it is sad to say, that right now in America, in the world, about 25 to 30% of people taking the vaccine have already had COVID, so the vaccine can not help them at all, and can only hurt them.
Mask Question
Unfortunately , ,, our public health response for months was absolutely focused unnecessarily so, on masking. I think if we would have taken the focus off masks, and actually focused on treatment, treating sick people, we would have saved hundreds of thousands of lives.
Having masks morning noon and night on TV commentary, our federal officials, they probably had innumerable press briefings on the mask. Can you imagine we haven’t had a single press briefing on vaccine safety, and we are asking people to take these vaccines, yet we have had a million press briefing on the mask.
Well here is a couple of points:
1) The virus is about one micron in size. The mask filters out three microns, even the really good ones. So the virus moves in and out of the mask very easily ,
2) there have been 12 randomized trials, that is our gold standard, including most recently the Dan Mask trial, showing public masking has no benefit.
In Dallas we have had a natural experiment. We had our Dallas Independent School district shut down, parochial schools didn’t, we never had any school outbreaks here or across the United States.
There has never been a credible case of a student giving the virus to a teacher. It has never happened. Pulling the kids out of school, and making the kids wear masks, retrospectively, was a complete and total waste of time.
Those of you who have college students, and I had a college student in my office the other day, and he was being seen for a cardiac problem. and I asked him how was college Univ of Texas?
End of Transcript of Interview with Dr. Peter McCullough
22:00
========================== =================
Update Sept 14, 2021: Dr Peter Breggin Interview with Dr Peter McCullough on Brighteon
————————— ———————–
TPC #559: Dr. Peter A. McCullough, MD, MPH (The Medical Super Bowl) Tommy’s Podcast Published September 7, 2021
Articles with Related Interest:
Rochelle Wolensky Warns of ADE Antibody Dependent Enhancement
Covid Vaccines Are Safe and Effective ?
Ivermectin and the Failure of American Medicine
Ivermectin Antiparasitic Anticancer Miracle Drug
Jeffrey Dach MD
7450 Griffin Road Suite 180/190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
header image courtesy of: Dare to Seek truth
References
1) (Cleveland Clnic Study)
Shrestha NK. 2021. Necessity of COVID-19 Vaccination in Previously Infected Individuals: A Retrospective Cohort Study. medRxiv.
study only looked at individuals over a five-month period
The study concludes, “individuals who have laboratory-confirmed symptomatic SARS-CoV-2 infection are unlikely to benefit from COVID-19 vaccination, and vaccines can be safely prioritized to those who have not been infected before.”
Importantly, not a single incidence of SARS-CoV-2 infection was observed in previously infected participants with or without vaccination.
(LA)
2) Kojima, Noah, et al. “Incidence of Severe Acute Respiratory Syndrome Coronavirus-2 infection among previously infected or vaccinated employees.” medRxiv (2021).
Previous SARS-CoV-2 infection and vaccination for SARS-CoV-2 were
associated with decreased risk for infection or re-infection with SARS-CoV-2 in a routinely screened workforce. The was no difference in the infection incidence between vaccinated individuals and individuals with previous infection.
(Israel)
3) Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections by Sivan Gazit, MD MA1,2*; Roei Shlezinger, BA1; Galit Perez, MN MA2; Roni Lotan, PhD2; Asaf Peretz, MD1,3; Amir Ben-Tov, MD1,4; Dani Cohen, PhD4; Khitam Muhsen, PhD4; Gabriel Chodick, PhD MHA2,4; Tal Patalon, MD1,
This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. end quote
4) O Murchu, Eamon, et al. “Quantifying the risk of SARS‐CoV‐2 reinfection over time.” Reviews in medical virology (2021): e2260.
Only one study estimated the population‐level risk of reinfection based on whole genome sequencing in a subset of patients; the estimated risk was low (0.1% [95% CI: 0.08–0.11%]) with no evidence of waning immunity for up to 7 months following primary infection. These data suggest that naturally acquired SARS‐CoV‐2 immunity does not wane for at least 10 months post‐infection.
4A) Goldberg, Yair, et al. “Protection of previous SARS-CoV-2 infection is similar to that of BNT162b2 vaccine protection: A three-month nationwide experience from Israel.” medRxiv (2021).
Vaccination was highly effective with overall estimated efficacy for documented infection of 92·8% (CI:[92·6, 93·0]); hospitalization 94·2% (CI:[93·6, 94·7]); severe illness 94·4% (CI:[93·6, 95·0]); and death 93·7% (CI:[92·5, 94·7]). Similarly, the overall estimated level of protection from prior SARS-CoV-2 infection for documented infection is 94·8% (CI:[94·4, 95·1]); hospitalization 94·1% (CI:[91·9, 95·7]); and severe illness 96·4% (CI:[92·5, 98·3]). Our results question the need to vaccinate previously-infected individuals.
5) Pilz, Stefan, et al. “SARS‐CoV‐2 re‐infection risk in Austria.” European Journal of Clinical Investigation 51.4 (2021): e13520.
We observed a relatively low re- infection rate of SARS- CoV- 2 in Austria. Protection against SARS- CoV- 2 after natural infection is comparable with the highest available estimates on vaccine efficacies.
6) Sheehan, Megan M., Anita J. Reddy, and Michael B. Rothberg. “Reinfection rates among patients who previously tested positive for COVID-19: a retrospective cohort study.” medRxiv (2021).
Conclusions Prior infection in patients with COVID-19 was highly protective against reinfection and symptomatic disease. Protective effectiveness increased over time, suggesting that viral shedding or ongoing immune response may persist beyond 90 days and may not represent true reinfection. As vaccine supply is a limited resource around the world, patients with known history of COVID-19 could delay early vaccination to allow for the most vulnerable to access the vaccine and slow transmission.
Asymptomatic vs Presymptomatic Transmission
8) Bender, Jennifer K., et al. “Analysis of asymptomatic and presymptomatic transmission in SARS-CoV-2 outbreak, Germany, 2020.” Emerging infectious diseases 27.4 (2021): 1159.
We determined secondary attack rates (SAR) among close contacts of 59 asymptomatic and symptomatic coronavirus disease case-patients by presymptomatic and symptomatic exposure. We observed no transmission from asymptomatic case-patients and highest SAR through presymptomatic exposure. Rapid quarantine of close contacts with or without symptoms is needed to prevent presymptomatic transmission.
Presymptomatic transmission accounted for >75% of all transmissions to OCs in the cohort (Appendix).
In conclusion, our study suggests that asymptomatic cases are unlikely to contribute substantially to the spread of SARS-CoV-2. COVID-19 cases should be detected and managed early to quarantine close contacts immediately and prevent presymptomatic transmissions.
9) Jung, Jiwon, et al. “Frequent Occurrence of SARS-CoV-2 Transmission among Non-close Contacts Exposed to COVID-19 Patients.” Journal of Korean medical science 36.33 (2021).
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission among non-close contacts is not infrequent. We evaluated the proportion and circumstances of individuals to whom SARS-CoV-2 was transmitted without close contact with the index patient in a nosocomial outbreak in a tertiary care hospital in Korea. From March 2020 to March 2021, there were 36 secondary cases from 14 SARS-CoV-2 infected individuals. Of the 36 secondary cases, 26 (72%) had been classified as close contact and the remaining 10 (28%) were classified as non-close contact. Of the 10 non-close contact, 4 had short conversations with both individuals masked, 4 shared a space without any conversation with both masked, and the remaining 2 entered the space after the index had left. At least one quarter of SARS-CoV-2 transmissions occurred among non-close contacts. The definition of close contact for SARS-CoV-2 exposure based on the mode of droplet transmission should be revised to reflect the airborne nature of SARS-CoV-2 transmission.
Physician List & Guide to Home-Based COVID Treatment
Dr. Peter McCullough Update on Vaccine for COVID Pod Cast
UncoverDC Published August 13, 2021
Yahi, Nouara, Henri Chahinian, and Jacques Fantini.Infection-enhancing anti-SARS-CoV-2 antibodies recognize both the original Wuhan/D614G strain and Delta variants. A potential risk for mass vaccination ? Journal of Infection (2021).
•Infection-enhancing antibodies have been detected in symptomatic Covid-19
•Antibody dependent enhancement (ADE) is a potential concern for vaccines
•Enhancing antibodies recognize both the Wuhan strain and Delta variants
•ADE of Delta variants is a potential risk for current vaccines
•Vaccine formulations lacking ADE epitope are suggested
Antibody dependent enhancement (ADE) of infection is a safety concern for vaccine strategies. In a recent publication, Li et al. (Cell 184 :1-17, 2021) have reported that infection-enhancing antibodies directed against the N-terminal domain (NTD) of the SARS-CoV-2 spike protein facilitate virus infection in vitro, but not in vivo. However, this study was performed with the original Wuhan/D614G strain. Since the Covid-19 pandemic is now dominated with Delta variants, we analyzed the interaction of facilitating antibodies with the NTD of these variants. Using molecular modelling approaches, we show that enhancing antibodies have a higher affinity for Delta variants than for Wuhan/D614G NTDs. We show that enhancing antibodies reinforce the binding of the spike trimer to the host cell membrane by clamping the NTD to lipid raft microdomains. This stabilizing mechanism may facilitate the conformational change that induces the demasking of the receptor binding domain. As the NTD is also targeted by neutralizing antibodies, our data suggest that the balance between neutralizing and facilitating antibodies in vaccinated individuals is in favor of neutralization for the original Wuhan/D614G strain. However, in the case of the Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity. Thus, ADE may be a concern for people receiving vaccines based on the original Wuhan strain spike sequence (either mRNA or viral vectors). Under these circumstances, second generation vaccines with spike protein formulations lacking structurally-conserved ADE-related epitopes should be considered.
======================== = ==================
On Friday 20th – 21st August, the Village SDA Church will host a COVID, Coercion, and Conscience weekend. National speakers such as Dr. Peter McCullough, Professor Bruce Cameron, and Dr. Lela Lewis,
Rebuttal to Peter Mccoullough Dr. Peter McCullough’s COVID-19 and Anti-Vaccine Theories Sean Pitman 2 weeks ago Dr Pitman quotes Dr Gorski (?)
================== =============== =============
Pandemic Perspectives Channel on Bitchute
“This Interview Could Save Your Life” | A Conversation with Dr. McCullough, Part #1
Renowned physician and professor of medicine Dr. Peter McCullough describes early treatment protocols for COVID-19 that have saved countless lives… and the forces that have aligned themselves against their widespread adoption.
“This Interview Could Save Your Life” Part Two: The Dangers of the Injections | Episode #20 Dr. Peter McCullough offers the most lucid and meticulous analysis to date of the mass injection program now ravaging the world.
McCullough, Peter A., et al. “Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19).” Reviews in cardiovascular medicine 21.4 (2020) Multifaceted-highly-targeted-sequential-multidrug-treatment-of-early-ambulatory-high-risk-SARS-CoV-2-Infection
McCullough, Peter A., et al. “Pathophysiological basis and rationale for early outpatient treatment of SARS-CoV-2 (COVID-19) infection.” The American journal of medicine 134.1 (2021): 16-22.
McCullough, Peter A. “Regarding:“Hydroxychloroquine: a comprehensive review and its controversial role in coronavirus disease 2019”.” Annals of Medicine 53.1 (2021): 286-286.
A grim warning from Israel: Vaccination blunts, but does not defeat Delta
With early vaccination and outstanding data, country is the world’s real-life COVID-19 lab 16 Aug 2021 By Meredith Wadman Science Magazine
Coronavirus in Israel: What do we know about the 143 hospitalized people? Jersualem Post Of the 143 hospitalized patients, 58% were vaccinated, 39% were not at all, and 3% were partially vaccinated.
By MAAYAN JAFFE-HOFFMAN JULY 21, 2021 ….Fifteen of the 20 people who died this month were fully vaccinated.
Latest UK Data: Vaccinated People 3-times More Likely To Die From Delta Variant Than Unvaccinated By News Rescue – June 27, 2021 by Kelen McBreen
A report published Friday by the UK government agency Public Health England reveals individuals who received a COVID-19 vaccine are more than three times more likely to die from the Delta variant than unvaccinated people.
Out of 117 total deaths occurring within 28 days of infection, 44 of them were unvaccinated individuals.
In total, 70 out of the 27,192 vaccinated individuals in the study died, which is a 0.26% mortality rate.
Meanwhile, 44 out of the 53,822 unvaccinated people in the paper died, resulting in a 0.08% mortality.
The Vaccines Do Not Stop Severe Covid or Death
By Vasko Kohlmayer September 11, 2021
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydachmd.com
www.drdach.com
Heart Book by Jeffrey Dach
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
http://sci.med.narkive.com/covV2Qo2/jeffrey-dach-book-announcment-natural-medicine-101
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Copyright (c) 2021 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. See Repost Guidelines.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation
Last updated on September 15th, 2021 by Jeffrey Dach MD
The post Dr Peter McCullough on Early Treatment vs Vaccination appeared first on Jeffrey Dach MD.
Dr Peter McCoullough on Early Treatment vs Vaccination
Dr Peter McCoullough on Early Treatment vs Vaccination
Tresncript of Interview
“The Vaccine Is Failing In The UK And Israel”
Interview Sept 2, 2021: Professor of Medicine at Texas A and M College of Medicine for about 10 years
I am on the Baylor Dalas caompus. I am ina provate practice. and I maintain my board cetification in Internal Medicine and Cardiology. I also lead a research team in downtowen Dallas.
When Covid 19 hit, I redirected all of my focus towards the pandemic.
I recognized this was going to be a giant challenge for us.
We have actually very few infectious disease doctors in the US, completed subscrine=bed in the hosptial.
I am more of an outpatient oriented doctor.
I poured all my effots into schoolarsjhip on Covid 19 in the last year.
In a sense Ive done a self dorected fellowshiop on infetious disease.
I have published the forst treatment guidance on how to treat COVID 19 as an outpatient. These are the most widely utilized publications in all of COVID 19 in the world for outpatient treatment.
Ive been relied upon by the US Senate ti testify in the Senate, and to render my opinion.
I have been blessed to a regular contibutor on FOX news almost every week now over the last serval months.
What kind of authority do I have to give any opinions about COVID 19 ?
Before COVID, I was the most published person in my field in world hisotry.
My field is the interfasce between heart and kidney disease. How do these organs
I am th eeditor in chief of CadioRenal Medicine.communicate with one another.
The editor in cheif of Reviews in Cardiovascular Medicine
I have 600 peer reviews publications in the Nationl Library of Medicine.
I have lectured all over the world, the New York Academy of Sciences, NIH, FDA,
I am on the calling card of someone who has a position of authority in medicine.
I have over 45 publications in COVID 19
I publuished the two sets of treatment guidancee when noone else woluld step up.
I have had the illness myself.
I have had serious cases in my family including fatalities.
I think as a single person, I probanbly have the most authority to give my opinnion on whats going on in this pandemic, than any one inthe world..
And I can tell you the probelem with what Americans are seeing on TV right now
is they are not seeing doctors like me working in teams of doctors and advising the country.
We are down to one or two people that are government officials, that people see on TV who by the way are not board certified, they dont have qualifiactions for douing what they are doing tight now. And as singular people, they are issuing , not recommendations, not guidance, they are issuing directives. and we are seeing these things come down over time. So we can tackle them one by one.
First off we should tackle five really important points.
When this first hit, noone knew what this virus was about, including myself.
But we do have a year and three months later, we have a framework of understanding
The first important point: The virus spreads from a sick person to a well person, period.
The virus does not spread from asymptomatic person to asymptomatic person. It took months to get these data.
Paper by Cowv out of China
paper by Madewell published in the best journals
it does not spread asymptomatically.
If anybody in this room has rthe virus right now, but they have no symptoms, they vcannot spread it to us, in fact they are forming their own immunity.
Assymptomatic spread must be less than 1% of all spread.
OK becasue of that, that means that assymptomatic testing was completely useless.
In the US we have had 35 million cases of COVID , we hav actually burned 400 million COVID tests right now.
Even the World Health Organisation says June 25, Stop the Assymptomatic Testing.
All this nasal and oral testing was never approved for routine screening, it esd never approved for people to get on airplanes, or any thing else,
That was just an over reach.
Point number one: No asymptomatic Spread.
Point number Two: Assymptomatic Testing is a complete waaste of time. It is not FDA approved. It is not even advised by the WHO.
Point Three: Natural Immunity, once somebody has had the virus , is robust complete and durable. You can not get the virus twice.
When grandmother had it last year , she is not going to get it again.
We have seen it sweep through the nursing homes. It is done. It is a one and done.
There is this narrative, tha people keep getting COVID over and over again. But when you ask people, No I have had it and I am done, One and DONE.
Cleveland Clinic Study
There has even been challenges where Cleveland Clinic published a study where people had recovered. They went right back and worked with COVID right in their face . You cant get it ((the virus COVID) again . So this idea its ONE and DONE, Natural Immunity is Robust, complete and durable. very important.
So if you have workers in your business who have had covid, they dont have to worry, they are not going to get it again.
There is incredible continuing fear, there are legal demands into the CDC to recognize Natural Immunity. Even Gov Abbott here in Texas, by Executive Order in April, has an EO, Natural Immunity, we recognize it in TEXAS by executive order..
And (these natually immune) people ask, DO I have to take the Vaccine ?
Of course you dont. You Can not get it (COVID) a second time. That is the third point.
The fourth point is : The Virus is treatable. That was our work. So we know now that we have an approach. People over 50 who have additional medical problems have a greater than one per cent chance of being hospitalized or dying . That is enough to treat. And we have tratment protocols that involve FDA approved EUA approved (EUA approved) antibodies. I can make a phone call. Patients can go right down here to Baylor, get an antibidy infusion free of charge. It is wonderful. The US goverment bought 500 million doses of these monoclonal antibodies, but there is no word of them. You dont see them on TV , there is no 1-800 numbers. When people get their COVID test result, therey are not told how to access these.
Your busineeses and viewers should demand ansers about antibody infusions. call your hospital and say , listen, my grandmother is sick with COVID 19, and i want an antibody infusion. Now is the time to get activated becasue your government agencies are not helping you on early treatment
We are busting the myth that COVID is not treatable.
I am here to tell you it is treatable . The key publications , I am the first author, Americal Journal of Medicine 2020, Reviews in Cardiovascular Medicine 2020,
these are the most cited and utilized
, and relied upon papers in all of COVID -19 in the world for early treatment
Patients over age 50 with multiple medical problems, that is the only group that really needs treatment. The younger person who presents with severe symptoms, they are a younger person with some problems like cyctic fibrosis sure, they could require treatment. But in general it is 25% of adults. Seniors ought to demand these monoclonal antibody infusions . President Trump got it.
After that, the drugs that work are used in combination and sequence, and they are based on a signal of benefit and acceptable safety. It is so early in the disease process, we dont have proven efficacy and safety, we dont. It is a signal of benefit and acceptable safey.
So what can be used ?
Hydroxychloroquine, supported by 200 studies. Countries like the US appropriately stockpiled it for a reason.
Ivermectin : 60 Supportive studies. We combine it with Doxycycline or Azithromycin
Everybody can use an inhaler, Budesonide inhaler. Richard Bartlett was the first to discover this in Texas. Prven in the UK in the STOIC TRIAL.
We can use on day 5 of pulmonary symptoms, oral prednisone, much like an asthmatic would use it. Someone with an allergic reaction condition.
We use a Gout medication, for 30 days in high risk patients called Colchicine, one pill a day. Proven in a large randomized trial from Montreal Heart Institute
called Co-Corona Trial 4,000 pts.
We use Aspirin 325 mg per day becasue this virus is unique , it causes blood clots.
It is the only viral infection we have ever seen that causes blood clotting, and that is what actually kills patients. So we use Aspirin as a blood thinner.
Its a full adult dose. Higher risk patients we actually use Lovonox injections, like someone would get for the treatment of a clood clot.
Thats what is called sequenced multi-drug therapy. It is all done at home. Supported by the Association ofo the American Physicians and Surgeons. AAPSonline.org
Download the home tretment Guide !!!! Be Ready.
It is also supported by another group in the United States
The front Line Critical Care Consortium. They have a litle differnt set of protocols, but the principles are the same.
Now these are well in advance of the CDC , NIH or the FDA or the Infectious Disease Society of America that have yet to publish any outpatient treatment guidelines.
Why is that ?
YThey have been focsing on inpatients. So one of the reasons I wanted to fill this void is: ” How many years are we goinfg to wait and have Americans Suffer before they get any treatment at home?
We can even order OXYGEN concentrators at home with a simple phone call. Becasue under the emergency use authorization, we can actually get them out to the home.
and get people supplemental oxygen.
We have been so successfull with this, we have an 85% reduction in risk of hospitalization and death. I have treated patients well into their 90’s and we have avoided th epanic and fear, isolation of the hospital,
The contemprotary mortality rate in the hospital right now if someone needs the ICU in the US, 38%, and thats published by the STOP COVID Collaboration out of Harvard.
So point number four is: Covid is treatable, it takes about 4-6 drugs.
ADULTS WITH MILD CASES- 5 days
Average person our age , about 10 days.
seniors, it could be about 30 days, a longer illness.
What about people under 50. They breeeze through COVID.
Neyutrceutical bundle which is recommended for everybody, which is reasonable includes:
zinc
Vitamin C
Vitamin D
Quercetin
If a Younger person developes symptoms, they can move into treatment. But only 25% of people who get COVID need early treatment. It helps them avoid the hospital or death. An d younger people breeze through this.
Point number 5 is the contentious issue of the vaccine, and I have rendered my opinion on this multiple times.
The vaccines are brand new. In the US we have Pfizer Moderna and J and J.
They are a brand new technology. They are nothing like a flu shot.
They actually transfer genetic material inside our cells, and they cause our cells to make the spike protein.
…
So ther is the ball, the nucleocpsid, and the little spines or spikes .
The vaccines trick our body ino making the soike protein , an dthen we form an immune reaction to it.
The short discussion on the vaccines, while half of Americans have taken them, for some induviduals the vaccines have not worked out too well, in terms of being sufficiently safe for human use.
Obviously, many tend of millions of Americans took it , they had a sore arm, they got through it just fine. People in my family took it. It is not a big deal if there are no complications. But for those who are getting complications, we are currently at as of today, CDC has told us, we are at 12,000 Americans that have died after the vaccine. 86% of the time independent reviewers have determined the vacicine caused the death. 50% of the deaths occurr within 48 hours of the vaccine. 80% of the deaths occurr within a week of the vaccine. And it is a modern day tragedy.
e have never had any medical product ever in th e history of mankind result in 12,000 American deaths. We have 400,000 certified vaccines injuries right now due to the vaccine along the lines of neurologic, cardiac, immunologic or hematologic abnormalities. Thats about the size of a mediaum sized city right now of people who have had vaccine injuries. So there is great concern as we move forward that the vaccines look like they dont have a safety profile to be the solution to the problem
What we knwo is gthat the number of ddeaths has exceeded the cumulative total reported into the data system for all time.
Just to give you an Idea, we have 70 (?) vaccines on the market, roughly 500 million shots . This year I had shingles =nd Flu shots. Everyone gets vaccines.
The average annual deaths reported to the database was about 150 or so.
13:46
The current vaccines are obsolete , unsafe and unfit for human use.
========================== ========================= =======================
header image courtesy of: Dare to Seek truth
Jeffrey DAch MD
.
Zinc Quercetin 120 Vegetarian Capsules
https://amzn.to/3iQqxQ8
Physician List & Guide to Home-Based COVID Treatment
https://rumble.com/vl499z-dr.-peter-m...
Dr. Peter McCullough Update on Vaccine for COVID Pod Cast
UncoverDC Published August 13, 2021
Suzanne Humphries Smallpox Illusions. How safe and effective was that vaccine?
French study Jounal of Infections ADE
Letter to the Editor|Articles in Press
Infection-enhancing anti-SARS-CoV-2 antibodies recognize both the original Wuhan/D614G strain and Delta variants. A potential risk for mass vaccination ?
Nouara Yahi Henri Chahinian Jacques Fantini
Published:August 09, 2021
•
Infection-enhancing antibodies have been detected in symptomatic Covid-19
•
Antibody dependent enhancement (ADE) is a potential concern for vaccines
•
Enhancing antibodies recognize both the Wuhan strain and Delta variants
•
ADE of Delta variants is a potential risk for current vaccines
•
Vaccine formulations lacking ADE epitope are suggested
Antibody dependent enhancement (ADE) of infection is a safety concern for vaccine strategies. In a recent publication, Li et al. (Cell 184 :1-17, 2021) have reported that infection-enhancing antibodies directed against the N-terminal domain (NTD) of the SARS-CoV-2 spike protein facilitate virus infection in vitro, but not in vivo. However, this study was performed with the original Wuhan/D614G strain. Since the Covid-19 pandemic is now dominated with Delta variants, we analyzed the interaction of facilitating antibodies with the NTD of these variants. Using molecular modelling approaches, we show that enhancing antibodies have a higher affinity for Delta variants than for Wuhan/D614G NTDs. We show that enhancing antibodies reinforce the binding of the spike trimer to the host cell membrane by clamping the NTD to lipid raft microdomains. This stabilizing mechanism may facilitate the conformational change that induces the demasking of the receptor binding domain. As the NTD is also targeted by neutralizing antibodies, our data suggest that the balance between neutralizing and facilitating antibodies in vaccinated individuals is in favor of neutralization for the original Wuhan/D614G strain. However, in the case of the Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity. Thus, ADE may be a concern for people receiving vaccines based on the original Wuhan strain spike sequence (either mRNA or viral vectors). Under these circumstances, second generation vaccines with spike protein formulations lacking structurally-conserved ADE-related epitopes should be considered.
Published on September 2nd, 2021 by Jeffrey Dach MD
The post Dr Peter McCoullough on Early Treatment vs Vaccination appeared first on Jeffrey Dach MD.
Free Monoclonal Antibody Infusion Regen-Cov Treatment for Covid 19
Free Monoclonal Antibody Infusion
(Regen-Cov Treatment) for COVID-19
Broward County Location:
CB Smith Park – 900 North Flamingo Road, Pembroke Pines, Florida,
Hours of Operation: Monday to Sunday 9am to 5pm
Don’t live in Broward ?, then use this link to find a location near you throughout state of Florida: https://www.patientportalfl.com/s/location-finder?language=en_US
Or call for Assistance:Telephone Hot Line: (850) 344-9637 Monoclonal Antibody Treatment Support Line
Monoclonal Antibody Therapy for COVID-19
Monoclonal antibody treatments can prevent severe illness, hospitalization and death in high-risk patients who have contracted or been exposed to COVID-19. These treatments are widely available in Florida. Treatment is free and vaccination status does not matter. If you are 12 years and older and are at high risk for severe illness due to COVID-19, you are eligible for this treatment. In clinical trials, monoclonal antibody treatment showed a 70% reduction in hospitalization and death. For high-risk patients who have been exposed to someone with COVID19, Regeneron can give you temporary immunity to decrease your odds of catching the infection by over 80%.
To schedule an appointment for Monoclonal Antibody Infusion:
Go to Florida Dept of Health Web Site: https://www.patientportalfl.com/s/?language=en_US
Set up an account. Once you have an Account set up, To schedule a monoclonal antibody treatment of REGEN-COV, made by Regeneron, select “GET REGEN-COV” on the homepage of your account screen.
A Doctor’s Prescription for the Infusion is NOT REQUIRED !!!! Just go the the web site and make an appointment !!!
Jeffrey Dach MD
7450 Griffin Road Suite 180/190
Davie, Florida 33314
954-792-4663
Published on September 2nd, 2021 by Jeffrey Dach MD
The post Free Monoclonal Antibody Infusion Regen-Cov Treatment for Covid 19 appeared first on Jeffrey Dach MD.
August 26, 2021
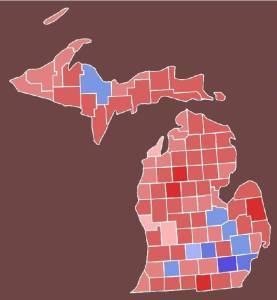
Matt Deperno on Whats Happening in Michigan ?
 Matt Deperno on Whats Happening in Michigan ?
Matt Deperno on Whats Happening in Michigan ?
Remember Antrim County on November Third ? A little glitch ? Or something else? Here is Matt Deperno’s update on what is happening in the great state of Michigan… Reawaken America Tour, Grand Rapids, MI – Matthew DePerno August 24, 2021
Published on August 26th, 2021 by Jeffrey Dach MD
The post Matt Deperno on Whats Happening in Michigan ? appeared first on Jeffrey Dach MD.
August 23, 2021
Director of CDC, Rochelle Walensky warns of ADE, Antibody Dependent Enhancement From Israel Data
 Director of CDC, Rochelle Walensky Warns of ADE, Antibody Dependent Enhancement From Israel Data
Director of CDC, Rochelle Walensky Warns of ADE, Antibody Dependent Enhancement From Israel Data
According to Robert Malone, MD inventor of the mRNA vaccine technology, the most severe adverse side effect of all four COVID-19 vaccines is ADE, Antibody Dependent Enhancement, responsible for the stunning failure of all previous coronavirus vaccine development efforts, causing all experimental animals death upon re-exposure to the virus. (16-17)
Two Types of Antibodies
In this scenario, there are two types of antibodies in the experimental animals. The first type is the neutralizing antibodies and the second type is the enhancing antibodies. The neutralizing antibodies are preferred since they “neutralize” or completely eliminate the virus from the body. The enhancing antibodies are the problem since they “enhance” entry of the virus into cells, enhancing viral replication and severity of the disease. Enhancing antibodies do exactly the opposite of the intended effect of the vaccine. Instead of protecting the animal, the vaccine makes the viral disease worse and kills the animal.(1-15)
Previous Failed Human Trials
Previous human vaccines against RSV and Dengue virus resulted in failed vaccine trials because of ADE, Antibody Dependent Enhancement. In the Philippines, failure of the Dengue vaccine program led to criminal charges for researchers. Their failed Dengue virus program vaccinated 800,000 children before the program was halted. (11-13)
Previous respiratory syncytial virus and dengue virus vaccine studies revealed human clinical safety risks related to ADE, resulting in failed vaccine trials. (3) Endquote
So far, with the mRNA COVID 19 vaccine, we have not seen this ADE to any appreciable degree in the US. However, early data from Israel suggests ADE is starting to appear in the vaccinated population, those who received their vaccination the earliest.
What is the significance of receiving your vaccine the earliest ? Pfizer is now recommending a third booster shot after 6 months, admitting the vaccine induced antibody protection wanes after 6 months or so.(14-15)
As antibodies wane, the patient is now at risk for viral infection after vaccination as we have been seeing with “break through” cases. This is the predicted scenario for ADE, and prompted Pfizer to recommend a third booster shot to avoid catastrophic ADE, as was seen with the Dengue virus in the Phillipines.(1-15)
Dr. Rochelle Walensky
Watch this video of CDC Director Rochelle Walensky who warns about ADE, or worsening disease in vaccinated individuals after re-exposure to the virus :
“Additionally, reports from our international colleagues, including Israel, suggest increased risk of severe disease amongst those vaccinated early.”
Conclusion: Rachelle Walensky of the CDC is now warning us about ADE , Antibody Dependent Enhancement. This is an adverse effect in which the vaccine makes the disease worse. Some authors have suggested abandoning the current mRNA vaccines in favor of new vaccines using T cell immunity rather than antibody immunity.(5)
These models place increased emphasis on the importance of developing safe SARS-CoV-2 T cell vaccines that are not dependent upon antibodies. (5) endquote
If ADE occurs to any extent in the vaccinated population, this would cause a severe loss in confidence in both vaccination of any type and the medical system itself.
Robert Malone MD Discussing ADE
Articles with Related Interest
The Covid Vaccine is Safe and Effective ?
Could the Covid Vaccine be the Next Vioxx ?
Ivermectin for Covid, the Failure of American Medicine
Jeffrey Dach MD
7450 Griffin Road Suite 180/190
Davie, Florida 33314
954-792-4663
Links and references
Header image courstesy of Rochelle Walensky and Wikimedia Commons File:CDC-Director-Rochelle-Walensky-Headshot.jpg
1) Nouara Yahi Henri Chahinian Jacques Fantini August 09, 2021 Letter to the Editor, Journal of Infection , Infection-enhancing anti-SARS-CoV-2 antibodies recognize both the original Wuhan/D614G strain and Delta variants. A potential risk for mass vaccination ?
• Infection-enhancing antibodies have been detected in symptomatic Covid-19
• Antibody dependent enhancement (ADE) is a potential concern for vaccines
• Enhancing antibodies recognize both the Wuhan strain and Delta variants
• ADE of Delta variants is a potential risk for current vaccines
• Vaccine formulations lacking ADE epitope are suggested
Antibody dependent enhancement (ADE) of infection is a safety concern for vaccine strategies. In a recent publication, Li et al. (Cell 184 :1-17, 2021) have reported that infection-enhancing antibodies directed against the N-terminal domain (NTD) of the SARS-CoV-2 spike protein facilitate virus infection in vitro, but not in vivo. However, this study was performed with the original Wuhan/D614G strain. Since the Covid-19 pandemic is now dominated with Delta variants, we analyzed the interaction of facilitating antibodies with the NTD of these variants. Using molecular modelling approaches, we show that enhancing antibodies have a higher affinity for Delta variants than for Wuhan/D614G NTDs. We show that enhancing antibodies reinforce the binding of the spike trimer to the host cell membrane by clamping the NTD to lipid raft microdomains. This stabilizing mechanism may facilitate the conformational change that induces the demasking of the receptor binding domain. As the NTD is also targeted by neutralizing antibodies, our data suggest that the balance between neutralizing and facilitating antibodies in vaccinated individuals is in favor of neutralization for the original Wuhan/D614G strain. However, in the case of the Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity. Thus, ADE may be a concern for people receiving vaccines based on the original Wuhan strain spike sequence (either mRNA or viral vectors). Under these circumstances, second generation vaccines with spike protein formulations lacking structurally-conserved ADE-related epitopes should be considered.
2) Risk of COVID‐19 vaccines worsening clinical disease
1. THE RISK OF ADE IN COVID‐19 VACCINES IS NON‐THEORETICAL AND COMPELLING
Vaccinees at higher risk for more severe COVID‐19 disease when they encounter circulating viruses.
3) Lee, Wen Shi, et al. “Antibody-dependent enhancement and SARS-CoV-2 vaccines and therapies.” Nature microbiology 5.10 (2020): 1185-1191.
Antibody-based drugs and vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are being expedited through preclinical and clinical development. Data from the study of SARS-CoV and other respiratory viruses suggest that anti-SARS-CoV-2 antibodies could exacerbate COVID-19 through antibody-dependent enhancement (ADE). Previous respiratory syncytial virus and dengue virus vaccine studies revealed human clinical safety risks related to ADE, resulting in failed vaccine trials. Here, we describe key ADE mechanisms and discuss mitigation strategies for SARS-CoV-2 vaccines and therapies in development. We also outline recently published data to evaluate the risks and opportunities for antibody-based protection against SARS-CoV-2.
4) Wen, Jieqi, et al. “Antibody-dependent enhancement of coronavirus.” International Journal of Infectious Diseases (2020).
Antibody-dependent enhancement (ADE) exists in several kinds of virus. It has a negative influence on antibody therapy for viral infection. This effect was first identified in dengue virus and has since also been described for coronavirus. To date, the rapid spread of the newly emerged coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), causing coronavirus disease 2019 (COVID-19), has affected over 3.8 million people across the globe. The novel coronavirus poses a great challenge and has caused a wave of panic. In this review, antibody-dependent enhancements in dengue virus and two kinds of coronavirus are summarized. Possible solutions for the effects are reported. We also speculate that ADE may exist in SARS-CoV-2.
5) Ricke, Darrell O. “Two Different Antibody-Dependent Enhancement (ADE) Risks for SARS-CoV-2 Antibodies.” Frontiers in immunology 12 (2021): 443.
COVID-19 (SARS-CoV-2) disease severity and stages varies from asymptomatic, mild flu-like symptoms, moderate, severe, critical, and chronic disease. COVID-19 disease progression include lymphopenia, elevated proinflammatory cytokines and chemokines, accumulation of macrophages and neutrophils in lungs, immune dysregulation, cytokine storms, acute respiratory distress syndrome (ARDS), etc. Development of vaccines to severe acute respiratory syndrome (SARS), Middle East Respiratory Syndrome coronavirus (MERS-CoV), and other coronavirus has been difficult to create due to vaccine induced enhanced disease responses in animal models. Multiple betacoronaviruses including SARS-CoV-2 and SARS-CoV-1 expand cellular tropism by infecting some phagocytic cells (immature macrophages and dendritic cells) via antibody bound Fc receptor uptake of virus. Antibody-dependent enhancement (ADE) may be involved in the clinical observation of increased severity of symptoms associated with early high levels of SARS-CoV-2 antibodies in patients. Infants with multisystem inflammatory syndrome in children (MIS-C) associated with COVID-19 may also have ADE caused by maternally acquired SARS-CoV-2 antibodies bound to mast cells. ADE risks associated with SARS-CoV-2 has implications for COVID-19 and MIS-C treatments, B-cell vaccines, SARS-CoV-2 antibody therapy, and convalescent plasma therapy for patients. SARS-CoV-2 antibodies bound to mast cells may be involved in MIS-C and multisystem inflammatory syndrome in adults (MIS-A) following initial COVID-19 infection. SARS-CoV-2 antibodies bound to Fc receptors on macrophages and mast cells may represent two different mechanisms for ADE in patients. These two different ADE risks have possible implications for SARS-CoV-2 B-cell vaccines for subsets of populations based on age, cross-reactive antibodies, variabilities in antibody levels over time, and pregnancy. These models place increased emphasis on the importance of developing safe SARS-CoV-2 T cell vaccines that are not dependent upon antibodies.
6) Wang, Jiong, and Martin S. Zand. “The potential for antibody-dependent enhancement of SARS-CoV-2 infection: Translational implications for vaccine development.” Journal of Clinical and Translational Science 5.1 (2021).
There is an urgent need for vaccines to the 2019 coronavirus (COVID19; SARS-CoV-2). Vaccine development may not be straightforward, due to antibody-dependent enhancement (ADE). Antibodies against viral surface proteins can, in some cases, increase infection severity by ADE. This phenomenon occurs in SARS-CoV-1, MERS, HIV, Zika, and dengue virus infection and vaccination. Lack of high-affinity anti-SARS-CoV-2 IgG in children may explain the decreased severity of infection in these groups. Here, we discuss the evidence for ADE in the context of SARS-CoV-2 infection and how to address this potential translational barrier to vaccine development, convalescent plasma, and targeted monoclonal antibody therapies.
7) Farshadpour, Fatemeh, and Reza Taherkhani. “Antibody-Dependent Enhancement and the Critical Pattern of COVID-19: Possibilities and Considerations.” Medical Principles and Practice (2021).
The pathogenicity of several viral infections is mediated by effector mechanisms of the immune system.
• Antibodies produced during the previous exposure to seasonal coronaviruses or possibly severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are proposed to trigger antibody-dependent enhancement.
• Antibody-dependent enhancement might lead to more severe and lethal illness upon infection with SARS-CoV-2, results in cytokine storm and tissue damage, and can modulate immune responses to-ward an inflammatory profile.
8) Bastug, Aliye, and Hurrem Bodur. “SARS-CoV-2 Infection and Antibody-Dependent Enhancement.” Understanding COVID-19: The Role of Computational Intelligence. Springer, Cham, 2022. 101-113.
Although there exist insufficient data, the titers of antibodies have been reported to be decreasing rapidly, suggesting a risk of reinfection. If reinfection occurs, another concern is whether it will be more severe due to the preexisting low level antibodies. To combat the continuing pandemic, antibody-based treatments, such as monoclonal antibodies (mAbs), convalescent plasma (CP) therapies, and vaccine studies, have been investigated. Although it may not be as troublesome as in the Dengue fever, clinicians should be alert about the possible risk of ADE. Non-neutralizing antibodies or sub-protective levels of NAbs may trigger immunopathogenic events via immune complex-mediated or Fc receptor-dependent endocytosis, resulting in enhanced viral infection. In this chapter, literature findings revealing the factors with an impact on eliciting NAbs, possible mechanisms and risks of ADE, and safety concerns for SARS-CoV-2 treatment interventions are outlined.
9) Khan, Kashif Rehman. “Antibody Dependent Disease Enhancement and the Covid-19 Vaccine: A Word of Caution.”
Antibody-Dependent Enhancement (ADE), refers to a counter-intuitive and potentially dangerous situation when the presence of antibodies, which are supposed to vanquish disease, worsens rather than quells an infection.
➢ In ADE, instead of neutralizing the virus, host antibodies, designated as non-neutralizing antibodies, facilitate its infectivity.
➢ Both Intrinsic and Extrinsic ADE work in tandem to enhance viral disease by increasing the number of cells getting infected and decreasing the innate response of body against that infection.
➢ It is important for scientists to consider ADE before progressing to clinical trials
10) https://europepmc.org/article/ppr/ppr...
Kelleni, Mina. “Autoimmunity and Antibody Dependent COVID-19 Enhancement of SARS CoV-2 Vaccination: A Global Human Right to Know then Decide.” (2021).
SARS CoV-2 vaccines are being advertised as a tool to beat COVID-19, yet with the emergence of different variants that are suggested to be vaccine-resistant, and the emergence of SARS CoV-2 vaccine induced serious adverse effects a personalized risk benefit ratio should be carefully assessed. mRNA based and adenovirus vectored vaccines, types of nucleic acid-based vaccination, were first ever or first commercially ever approved for the public, respectively. However, these new types possess a potential risk to induce auto-immune diseases e.g., thrombocytopenia and some of these complications might also reason for some of the post vaccination sudden death reports e.g., autoimmune myocarditis and immune induced thrombosis and thromboembolism. Moreover, all SARS CoV-2 types of vaccines, depending on the spike protein immunogenicity, especially the conventional inactivated ones might increase the likelihood of COVID-19 severity upon re-infection through antibody dependent enhancement which might also reason for some of the serious adverse effects encountered with administration of convalescent plasma to COVID-19 patients. Moreover, these vaccines might have shared in development of the potentially more lethal SARS CoV-2 B.1.617 variants and might lead to evolution of more virulent ones. Finally, A moral, legal, and sacred constitutional public right to know and decide basing on a personalized risk benefit ratio must be secured. Finally, it is a real misfortune that a draft of this manuscript is being denied an opportunity to be properly peer reviewed by numerous reputable medical journals for more than six months and even before a single mortality was reported and we totally condemn, from a medical point of view, any national or international policy that necessitates these experimental vaccines and we also condemn the trials in children as well as the European Court of Human Rights shameful ruling that compulsory vaccination would not contravene human rights law and we suggest that the rapid race to develop and approve SARS CoV-2 vaccines might eventually end with a man-made Hades.
11) Dengue vaccine fiasco leads to criminal charges for researcher in the Philippines By Fatima Arkin Apr. 24, 2019 , SCience Magazine
A prominent pediatrician and medical researcher in the Philippines has been indicted over the failed—and many say premature—introduction of Dengvaxia, a vaccine against dengue that was yanked from the Philippine market in 2017 because of safety issues. If convicted of accusations leveled at her by the national Department of Justice (DOJ), Rose Capeding, 63, former head of the dengue department of the Research Institute for Tropical Medicine (RITM) here, could face up to 48 years in prison.
In September 2018, DOH Undersecretary Enrique Domingo told reporters that 130 vaccinated children had died; 19 of those had dengue, meaning ADE possibly played a role. The case triggered “mass hysteria,” says Edsel Salvaña, an infectious disease physician at the University of the Philippines here. “Parents thought their kids were all going to die.”
12) Wilder-Smith, Annelies, Stefan Flasche, and Peter G. Smith. “Vaccine-attributable severe dengue in the Philippines.” The Lancet 394.10215 (2019): 2151-2152.
In 2016, WHO1 recommended that the dengue vaccine CYD-TDV (Dengvaxia; Pasteur, Lyon, France), the first dengue vaccine, licensed for use in adults and children aged 9 years or older, be considered for use in highly endemic regions where at least 70% of 9-year-old children had previously been infected with dengue. The Philippines was the first country to introduce Dengvaxia on a large scale in selected highly endemic regions, targeting about 1 million children aged 9–10 years. In November, 2017, an excess risk of hospitalisation for dengue and severe dengue in vaccinees who had not had a previous dengue infection at the time of vaccination was reported,2 on the basis of retrospective analyses3 of data from the Dengvaxia phase 3 trials, using a novel non-structural protein 1 (NS1) based antibody assay. Following a reanalysis of these data,3 the Philippine Dengvaxia programme was suspended. However, by the time the programme had been suspended, more than 830 000 children had received at least one of the three recommended Dengvaxia doses. The news about the safety concerns in dengue-naive vaccinees led to major public outcry, with loss in vaccine confidence that extended to routine childhood vaccines.4
13) Larson, Heidi J., Kenneth Hartigan-Go, and Alexandre de Figueiredo. “Vaccine confidence plummets in the Philippines following dengue vaccine scare: why it matters to pandemic.” Human Vaccines & Immunotherapeutics.
In November 2017, it was announced that the new dengue vaccine (“Dengvaxia”) had risks for those not previously exposed to dengue. While some countries proceeded with adjusting guidance accordingly, the Philippines reacted with outrage and political turmoil with naming and shaming of government officials involved in purchasing the vaccine, as well as scientists involved in the vaccine trials and assessment. The result was broken public trust around the dengue vaccine as well heightened anxiety around vaccines in general. The Vaccine Confidence ProjectTM measured the impact of this crisis, comparing confidence levels in 2015, before the incident, with levels in 2018. The findings reflect a dramatic drop in vaccine confidence from 93% “strongly agreeing” that vaccines are important in 2015 to 32% in 2018. There was a drop in confidence in those strongly agreeing that vaccines are safe from 82% in 2015 to only 21% in 2018; similarly confidence in the effectiveness of vaccines dropped from 82% in 2015 to only 22%.
14) CDC warns of a “significant decline” in vaccine effectiveness for some, prompting booster dose decision By Alexander Tin Updated on: August 18, 2021
New data being released Wednesday by the Centers for Disease Control and Prevention warns of a “significant decline” in vaccine effectiveness against infection from COVID-19 in nursing home residents, as the highly contagious Delta variant of the virus causes a spike in hospitalizations among mostly unvaccinated Americans.
The release came as the Biden administration says it is preparing to offer booster shots for all Americans who got the Pfizer or Moderna vaccines, eight months after their second dose, beginning the week of September 20.
“Given this body of evidence, we are concerned that the current strong protection against severe infection, hospitalization and death could decrease in the months ahead, especially among those who are at higher risk or who were vaccinated earlier,” CDC Director Dr. Rochelle Walensky said at a briefing Wednesday.
15) CDC, FDA contradict Pfizer on COVID-19 vaccine booster
16) mRNA vaccine inventor: COVID-19 vaccines may make virus more dangerous Dr. Robert Malone warns that the development of antibody dependent enhancement among those vaccinated with COVID vaccines ‘is the vaccinologist’s worst nightmare.’ The scientist has recently been calling for a halt to vaccinations.
17) Dr Robert Malone: “The Covid-19 Vaccine Causes the Virus to Become More Infectious”
=========================
Nurse raises hell…Posted by Kane on August 20, 2021 7:14 am
https://www.newsweek.com/7-vaccinated...
7 Vaccinated Florida Patients Die of COVID; Nurse Calls Situation ‘Disturbing’
By Andrew Stanton On 8/17/21 at 10:47 AM EDT
Florida nurse said seven fully vaccinated patients died from COVID-19 in the past two weeks in a situation she as “heartbreaking.”
Patricia Seemann, who runs All About You Home Visiting Clinicians in Saint Cloud, told Newsweek in an interview Tuesday afternoon that before the deaths, she had successfully treated hundreds of patients with COVID-19. She said she works with housebound patients who are over 60 years old and are at high-risk of COVID-19 related deaths. “We didn’t lose a single patient,” she said.
https://fee.org/articles/massive-nurs...
Massive Nurse Shortage Hits Houston—Weeks After 150 Unvaccinated Nurses and Hospital Workers Fired
Houston hospitals have “reached a breaking point” amid a COVID-19 outbreak, which struck weeks after 150 hospital workers were fired by Houston Methodist hospital, one of several hospitals struggling.
Wednesday, August 18, 2021
BRAVE NURSE EXPOSES CDC & FAUCI LIES — REGISTERED NURSE NICOLE
A courageous registered nurse has come forward to blow the whistle on the CDC, Dr. Fauci & the mainstream mockingbird media’s covid “vaccine” lies. Her name in Nicole and in coming weeks she’ll drop more bombshells.
Local doctors say nursing shortage causing hospital backups, diverting patients
Local doctors say nursing shortage causing hospital backups, diverting patients
Critical Mass: The U.S. Nursing Shortage is Close to Blowing Up in Our Faces
Critical Mass: The U.S. Nursing Shortage is Close to Blowing Up in Our Faces
Ingraham Angle Immunology {professor Byram Bridle There is no pandamic of the Unvaccinated
Dr. Byram Bridle / Viral Immunologist at the University of Guelph
First published at 20:44 UTC on August 19th, 2021. Career Destroyed for speaking about COVID Vaccine.
August 4, 2021…Doctor who was part of the team developing a novel covid vaccine platform WE MADE A MISTAKE
A message from Dr. Anne McCloskey
WATCH: Perspectives on the Pandemic #17 “2020 and 2021 have comprised a global propaganda spectacle of unprecedented scale and sophistication.”
WATCH: Perspectives on the Pandemic #18 “One of the things that Covid rollout has done, is create a whole new category of forbidden speech…if you’re not completely credulous then you’re somehow “putting people at risk”.
https://player.fm/series/the-delingpo...
The Delingpod: POD-CAST The James Delingpole Podcast » Mark Crispin Miller 8/20/21
1 hr 47 minutes
Published on August 23rd, 2021 by Jeffrey Dach MD
The post Director of CDC, Rochelle Walensky warns of ADE, Antibody Dependent Enhancement From Israel Data appeared first on Jeffrey Dach MD.
August 16, 2021
Tĕn 1ND1SPUTĂβLE f@čts
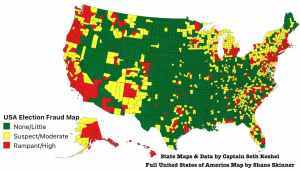 Tĕn 1ND1SPUTĂβLE fāčts on the շoշo єIєčtion That Ărgűe for Ăűđits By ʍichāĕI ƑIyŋŋ
Tĕn 1ND1SPUTĂβLE fāčts on the շoշo єIєčtion That Ărgűe for Ăűđits By ʍichāĕI ƑIyŋŋ
CLICK HERE FOR LINK TO ARTICLE
Published on August 16th, 2021 by Jeffrey Dach MD
The post Tĕn 1ND1SPUTĂβLE f@čts appeared first on Jeffrey Dach MD.
August 1, 2021
The Covid Vaccine is Safe and Effective ?
 The Covid Vaccine is Safe and Effective? by Jeffrey Dach MD
The Covid Vaccine is Safe and Effective? by Jeffrey Dach MD
If you have been getting your information from the nightly news, Facebook, Twitter or You Tube, you will not see any information about COVID vaccine adverse effects. This has all been scrubbed off the internet and censored. However, you will be seeing this information here in this newsletter.
Over the weekend, the CDC has admitted the vaccine is ineffective for the Delta variant of the Covid Virus, the predominant variant now circulating. This data comes directly from the CDC MMR Weekly publication on data from Barnstable Massachustes. And because of this new data, the head of the CDC, Dr. Rochelle Walensky, is now backtracking on masks, advising all vaccinated people to resume wearing masks, another admission of vaccine ineffectiveness.
The top virologists in world have been warning about this for months. According to Robert Malone PhD, a mass vaccination program during a pandemic will only produce vaccine resistant mutant viral strains, making the vaccine ineffective. This is a direct result of evolutionary pressure from using the vaccine in a mass vaccination program. The vaccine eliminates the original strain, leaving behind the resistant mutant strain that is free to replicate and spread through the population. According to Dr. Malone, the new Delta strain is much more contagious than the original one with an R value of 8 (similar to chickenpox).
Other revelations from Dr Robert Malone is that new data from Pfizer shows that the vaccine efficacy wanes after 6 months, and Pfizer just announced the need for a “booster” shot after 6 months. Another admission the vaccine quickly becomes ineffective.
According to Dr. Malone, inventor of the mRNA virus vaccine technique, a more logical and “scientific” approach to the pandemic is to protect the vulnerable (elderly and immunosuppressed) , while allowing the virus to circulate freely among the rest of low-risk younger population. At the same time early treatment must be made available for anyone who becomes symptomatic with Covid, something the government is not doing. Not only are they not making early treatment available, the government in collusion with the mass media and Big Tech, is actively preventing any knowledge of early treatment from getting out to the people. This is a crime of massive proportions. According the Dr. Malone and Dr. McCullough, information about early treatment has been with-held, and censored by government in collusion with Big Tech and the mass media, representing criminal malfeasance.
Early treatment is highly effective and includes ivermectin, hydroxychloroquine, zinc, budesonide, etc. Other preventive measures include optimizing vitamin D levels, vitamin A, C, Quercetin etc. This program has been described in previous newsletters. I should add that over the last year of this pandemic, I have been glad to use early treatment for any one who requests it. Gratefully, all of these patients have recovered uneventfully without any needing hospitalization.
New studies have been published showing that covid infection creates a robust durable natural immunity far superior to vaccination. This is no surprise, since this is true for all other viruses (examples being measles and chickenpox in which natural immunity is more durable and more robust than vaccine immunity). Imagine if the government had made this early treatment widely available early on. We would have been over this and back to normal with herd immunity by now.
CDC Withdraws Approval for COVID PCR Testing
In an Laboratory Alert, the CDC last week revoked emergency use authorization for the COVID PCR test. In previous newsletters, we have discussed the problem of false positives with this PCR test, and we quickly changed our office policy regarding testing in April of last year. We do not recommend asymptomatic testing because of the false positive problem. The test is unreliable.
Covid Vaccine Adverse Events from CDC REPORT July 26, 2021.
Thrombosis with thrombocytopenia syndrome (TTS) after Johnson & Johnson’s Vaccine:
This is an auto-immune destruction of the platelets leading to severe bleeding and death from very low platelet counts.
Guillain-Barré Syndrome (GBS)
This is a neurological injury causing paralysis. Below we will show you a series of videos from people suffering from neurological injury from the vaccine.
Myocarditis and Pericarditis:
1,194 reports of myocarditis or pericarditis among people ages 30 and younger who received COVID-19 vaccine: This is damage to the heart muscle or heart lining in young people.
6,340 Dead After the Vaccine
From 12/14/20 to 7/26/21, SIX thousand Three hundred and Forty (6,340) people died after receiving a COVID-19 vaccine. You will notice that the CDC says that a report of death in the VAERS data base does not prove it was caused by the vaccine. This is the reason why all other vaccine programs must have safety boards set up to monitor vaccine deaths and adverse events. Where is the safety board for the COVID vaccine? They conveniently neglected to do that, another malfeasance of criminal proportions, another way to hide the adverse effects from the public and themselves.
Personal Videos of Vaccine Adverse Effects
The below videos are taken by people who have suffered neurological injury after COVID Vaccine. Are you wondering why you haven’t seen these before? The reason is because all of these videos have been censored and removed from Facebook, Twitter, You Tube and Instagram.
Nurse is Censored After Having Extreme Adverse Reaction to Covid Vax
Previously Healthy Woman Suffers Severe Reaction from Pfizer Vaccine
The Adverse Reaction To Vaccines
Covid 19 vaccine reaction 10/02/2021
Woman’s severe reaction to Pfizer COVID-19 vaccine prompts investigation
Registered Nurse Adverse Reaction To Moderna Covid19 Vaccine
a nurse who got vaccinated with the mRNA vaccine against covid 19 / Vaccine reaction
Covid 19 vaccine reaction – She is ONLY 21 years old
=======================================================
HEARTBREAKING: Mother in Tears After Daughters’ TRAGIC Reaction to Covid Vaccine
Dinesh D’Souza Published July 5, 2021 11,769 Views
FOX News covid Vaccine Adverse Effects round Table
Senator Ron Johnson….Stephanie and Mattie
===================================
Articles with Related Interest:
Could the Covid Vaccine be the Next Vioxx ?
Jeffrey Dach MD
7450 Griffin Road Suite 180/190
Davie, Florida 33314
954 792 4663
www.jeffreydachmd.com
Links and References
Episode 1,137 – Deep Dive into COVID
Bannons War Room Published July 31, 2021
Dr Robert Malone on Covid 19
Dr Peter Mccoullough Video interviews
New US mask guidance prompted by evidence vaccinated can spread Delta
CDC director Rochelle Walensky cites ‘new science’
People with outbreak infections can pass on virus
Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings — Massachusetts – July 30, 2021
Morbidity and Mortality Weekly Report
Early Release / Vol. 70 July 30, 2021
An outbreak caused by the SARS-CoV-2 Delta variant (B.1.617.2) in a secondary care hospital in Finland, May 2021 Eurosurveillance Volume 26, Issue 30, 29/Jul/2021
Covid-19 deaths are rising and official data shows 87% of the people who have died were Vaccinated BY DAILY EXPOSE ON JULY 29, 2021
CDC confesses: Vaccines are failing, the vaxxed can be super-spreaders, demands return to mask mandates for everyone, including the vaxxed
by Planet Today News 7/30/2021
The Vaccine Causes The Virus To Be More Dangerous Robert Malone
Bannons War Room Published July 28, 2021
The Pfizer mRNA vaccine: pharmacokinetics and toxicity Michael Palmer, MD and Sucharit Bhakdi, MD July 23rd, 2021
Iceland: Vaccines do not work.
Iceland has been a vaccine paradise: Some 90 percent of people between the ages of 40-70 and 98 percent of those over 70 are fully vaccinated. On June 26, it abolished all lockdown rules. “Thank you for this joint struggle,” the Health Minister told citizens. Now the country could be heading for new lockdown restrictions for the next five, ten or fifteen years. Published: July 28, 2021, 11:42 am
Natural infection vs vaccination: Which gives more protection?
Nearly 40% of new COVID patients were vaccinated – compared to just 1% who had been infected previously.
COVID: Bennett vows decision on 3rd shot is near as cases top 2,000
On Tuesday morning the number of serious patients stood at 138, compared to 124 on the day before. By ROSSELLA TERCATIN JULY 27, 2021 More than half of the current cases and two-thirds of patients in serious condition were fully vaccinated, the Health Ministry reported.
Actor Michael Rapaport took to TikTok on Wednesday to trash Dr. Anthony Fauci and the Centers for Disease Control and Prevention(CDC) for their mixed messaging on Chinese coronavirus vaccines.
“I just watched Tony Fauci and CNN — and Fox — tell me that people with the vaccine, vaccinated people, are now spreading the coronavirus,” the Deep Blue Sea and Atypical star said on TikTok. “I went from being a hero because I’m vaccinated, and now you motherfuckers are calling me a superspreader? I ain’t no fucking superspreader,” he said.
Breaking the pandemic spell Daily FT Saturday, 31 July 2021 00:12
Study: Vaccinated people can carry as much virus as others
By LINDSEY TANNER, MIKE STOBBE and PHILIP MARCELOJuly 30, 2021
Published on August 1st, 2021 by Jeffrey Dach MD
The post The Covid Vaccine is Safe and Effective ? appeared first on Jeffrey Dach MD.
Jeffrey Dach's Blog

- Jeffrey Dach's profile
- 3 followers


{kind=link}
_E.jpg){kind=link}