
Arthur Janov's Blog, page 5
March 1, 2017
Suicide is Painless: Repression, Despair and the Relief of Reliving Near-Death Feelings
A recent federal government study shows that suicide in the United States has become epidemic, hitting an alarming 30-year high. More and more people, both men and women in almost every age group, are killing themselves, according to a report from the National Center for Health Statistics. And experts are struggling to adequately explain the troubling trend.
“The question of what has driven the increases is unresolved, leaving experts to muse on the reasons,” states the New York Times in an article about the suicide data.(1)
And so they speculate. Maybe it’s the rising divorce rate, or the lower rates of marriage. Maybe it’s the worsening economy or the new limits on social mobility. Or maybe it’s the country’s weak suicide prevention network.
They can’t find the answers, I believe, because external factors are not the cause; they are just the trigger. After all, many people get divorced and lose their jobs and their homes, or worse, but don’t decide to end their lives. The explanation is elusive because the causes are hidden. They lie deep inside the desperate individuals who see no way out but death, and who may not even know what is driving their desire to take their own lives.
The best way to illuminate the problem is to look at it from the other side. Set aside for a moment those poor souls who are suffering obvious misfortunes. Consider instead those apparently lucky people who have it all, but still choose to end it all. Why do so many celebrities commit suicide?
Suicide and Success
Celebrity suicides always strike us as a mystery. These are successful, wealthy people we admire and emulate. We even try to be like them. So when the rich and famous find their lives too much to bear – as did L’Wren Scott, the high-end fashion designer and girlfriend of Mick Jagger – we inevitably wonder why. Scott hanged herself in the multi-million apartment she had shared with Jagger in New York. She didn’t leave a note. Her friends, who described her as kind and considerate, were shocked. Jagger, who was on tour with the Rolling Stones in Australia, issued a statement claiming he was "still struggling to understand how my lover and best friend could end her life in this tragic way." Everyone was asking the same question.
There have been a number of people who have committed suicide who seemed at the pinnacle of success. And most of us thought that once we choose a profession and follow it and succeed at it, becoming an expert and well known, that would be fulfilling. We would feel like a success. Wrong. When we have deep-rooted lack of love, rejection, indifference and lack of touch early in our lives we cannot feel like a success. We can only feel what was left embedded in us as an imprint: the feeling of being unloved, empty, isolated, unwanted. That is always primary. All else and all later feelings lie on top of the imprint. We need to keep in mind that the imprint is embedded very early in life when the struggle has a life-or-death quality. It takes precedence over any later adversity. The memory is of a life-endangering event. It is not an imaginary time; survival is at stake (lack of oxygen at birth). And later, even the slightest threat takes on the original force of the reaction. Through resonance (the linkage between high nerve pathways and lower ones) terror is again elicited. What is set off? The feeling tone, for feelings are primary very early in life, long before we develop an overall sense of the total context. But the feeling tone will be an augury of a trauma gone by, and also a pathway to the past where the tone originated, engendered by perhaps an overdose of anesthetic to the mother for her pain but is far, far too much for a six-pound baby. That tone (hopelessness) may well underlie later depression, which seems such a mystery. But we are immersed in a sense of “what’s the use?” There is no reason to try or to go on; we are trapped in that imprinted memory where it was hopeless. This imprint may well be the template for building even stronger hopelessness when other needs are not fulfilled such as being held and soothed. And what do we do when we are bereft of that knowledge of the lingering tone? A tone due to its immense impact remains unconscious, repressed by the forces that are elicited to keep us from feeling devastating agony. We seek to submerge it further with drugs. We do the opposite of what is required, which is to release that memory from its neurobiologic cage. But when we observe it with all its power it seems overwhelming. This is why we are working with some medications to ameliorate the impact of that pain so it does not have to be experienced with all its fury. There is only one way to stop the suffering, and that is to revisit the imprint and relive the pain. Until then, we cannot know the real lack and what it is. That is why the system insists on reliving later in life. Our own system is pushing for real integration and liberation, because it seeks to become whole again. That imprint has only one goal in life; to be relived exactly as it was laid down. To finish the unfinished job of integrating what was repressed and put aide at its origin. Its message is a constant warning of unfinished business. The pain from very early on has to be felt and dealt with in all its agony and terror. The imprint knows no mercy. It wants conscious awareness somewhere inside even while the top cortical level does what it can to imprison it. Conscious awareness means delving into deep feeling plus ultimate awareness of what it is. The imprint will never leave until it is lived again, fully, in its original context. Enough rearranging of the chairs on the Titanic. We must join feelings with their thoughts and make ourselves whole. Fame won’t do that; I have treated enough stars to know that, and my patients also know it. There is no substitute for extirpating the imprint. None. Avoiding the imprint and we are leaving misery in place. Reliving it finally stops the terrible drive to feel like a success; to run from the feeling. That is different from being authentically successful, which is the drive to do things right. A little more relaxing.
To be loved early on, that is what sets the stage for your life. It means fulfilling basic needs as they evolve; it makes us feel confident and productive, but not driven. It offers daring and enthusiasm and a joie de vivre. It allows us to try but never in desperation. Symbolic love – the kind we get from fame and celebrity – has to be repeated over and over exactly because it cannot fulfill. Why not? Precisely because it is symbolic, a substitute for the true love we never got from our parents. When there is a basic lack of fulfillment early in life, especially during gestation, birth and infancy, an imprint is created that stamps in that deprivation, through the partially open sensory window. That imprint is embedded deep in the brain and stays there, almost inaccessible. We are aware only of a gnawing emptiness, feeling unfulfilled. Empty like a shell, as one patient put it. And that need, now un-anchored from its source, drags us into the race for symbolic fulfillment. But it’s a race that never ends because it does nothing to alter the motor that’s driving it, which is the painful, buried imprint of getting no love when it really mattered. No hugs, no attention, no sympathy, no understanding, nada. No love. And that compounds and builds into a massive forceful load of unconsciousness. For most us, given a bit of hope for love we are galvanized. But those with deep implacable hopelessness it seems to be a signal to give up; the original reaction that was life saving. Again, the basic survival imprint. Once the pain is embedded and out of reach, we will seek out substitutes, so as to stop feeling empty and unloved. The agony from that deep, deep pain becomes a primordial part of us. It now confuses us, distracts us, and above all, stops our concentration. Oh yes; it depresses us because we live with an enemy in the house that we cannot escape. It lives with us and in us; it claws for its liberation; it wants freedom to live the pain, believe it or not. Yet we do what we can to stop it. No wonder most psychotherapy is aimed at repression and rationales, and understanding but never deep feeling. Patients get a bit of relief, which the he settles for; but no cure. So what does the successful person feel? Very little: Down, unhappy and unfulfilled. He has no other choice because those feelings will not leave even for mercy’s sake. Mercy has no part in the lexicon of the unconscious; it follows the road to what seemed to work originally. Freud called it The Repetition Compulsion. Let us never forget the enormous pull of that embedded hopelessness low in the nervous system. It drags us down toward the non-integrated feeling that might have occurred when the newborn was heavily dosed with anesthetics; or earlier there might a smoking mother or one who drank all of the time. Or worse, a carrying mother who took constant painkillers, which diminished oxygen supplies. This, inter alia, also, drugged the baby and affected his breathing and energy levels. The drugs infused into the baby again drains him of effort and will power. He may be born passive, inactive and unresponsive. His whole being has given up against insuperable odds. And that erupts the minute he must make any strenuous effort. All this keeps him from feeling like a success; “I can do and succeed”.
Success is not a real feeling; being loved is. Fame is other people’s idea of our achievements; it is in a way their feeling… Admiration, humble, important, etc. And why does even the most accomplished person never feel satisfied nor fulfilled? Because all of his fulfillment and all of his admiration is symbolic; it is not the love he needed early on. It coversit over the lack of love, sits on top of the real need. The feeling window is now closed, and leaves an emotional vacuum in its place. It is the imprinted pain that cannot be erased no matter what kind of success is there. And it drives him for more and more – more money, more applause, more awards.
Finally at the top of his fame he feels still unfulfilled and a failure; there is nothing more to gain, nothing more to try for. He looks at all his billboards and feels empty. What does it mean? “I don’t know what else to do to feel good, to feel successful.” It seems that life is empty. There is no point; suicidal thoughts thrust their way in, as he feels the real deep feeling of hopelessness and helplessness that he has been escaping from in his work. The pain that drove it all is still alive and gnawing inside. It says, sotto voce, you are not loved and that is all that matters. Something is missing and you have no idea what that is. You have failed at what matters most; to be adored, admired, encouraged, held and caressed. That is the constant malaise that speaks of something missing. “All your drive was to try to escape the imprinted feeling and feel loved, and you believe you are, but not by the people who really matter, and not at the time when love was a life-or-death affair. There is a critical window for love to happen and a special time when the system is at its asymptote of need. When the critical time has passed repression takes over; it is too late now for fulfillment so there is no choice; symbolic fulfillment takes place; the ever-present audience who adores.
I treated one film director who became seriously depressed when he was no longer on stage. He felt useless, unneeded and unwanted; he started to feel his old feelings once again, only before therapy he drugged his hopelessness and now in therapy he is feeling it for what is really is. He began to feel the childhood part of the pain with parents who did not want him around; he was convinced there was something seriously wrong with him. This lay on top of the earlier pains of a sense of dying, of suffocating and losing consciousness. But not being needed on set began the whole process all over again. The first part was the feeling of “I will die if I am not loved,” and then much later, “I am dying and there is nothing I can do to escape.” This was the ultimate helplessness and hopelessness, the key elements of depression. Resonance always involves the chain of pain; the neuronal linkage from one set of neural processes to another. It is why something innocuous can set off catastrophic feelings.
As I have written à maintes reprises, many times over, we respond primarily and firstly to apparent problems in the present, and later to inner links that are awakened by those current problems, such as job losses or divorce. Those repressed traumas are ready to fire and when those links fire together they become wired together, solidified. That is the process I call resonance. The body and brain are busy reacting to what happened decades earlier during womb-life and birth. Those are the events we continually react to because of their remoteness, something that occurred when we were vulnerable and easily and heavily impacted. This is not only my hypothesis. Within the past 20 years, there have been literally hundreds of studies verifying the importance of early imprints, how they last a lifetime and alter our systems. Imprints lay down engraved memories that show themselves when we are alone, in a weakened state or otherwise too open to events.
That is what I believe may have happened to L’Wren Scott in those moments alone before she took her life. She must have had an inkling, a deep down unease and hopeless feeling that would have warned her. It was all hidden inside her, pushing through her weakened defense layers and making her feel so hopeless and “down,” despite her current surroundings. Being alone for a short time can set off being left and abandoned as a child; this is only surmise for now since I have not idea about this but I have seen in my patients. It can first set off, “I am all alone and no one to hold and comfort me.” Just a few hours alone with no one nearby can do it. Remember, small things can set off huge feelings. If she were left alone and neglected by her parents very early on, the connection to despair of the past it becomes clear.She probably had no idea about imprints or deep-lying trauma/memory. That is the reason our theory is so important, so that people who are suffering can be aware of what is going on inside and understand where their despair and suicidal thoughts come from. This may avoid needless deaths. How tragic and unnecessary all this. And now you understand our mission: not money nor fame, but the lives of us humans. We all have a basic right to a full-length life. The Way In Is The Way Out
You may wonder why a privileged and wealthy celebrity can’t find distractions for her despair. Why doesn’t she run away or go to parties and “take her mind off of it?” She cannot; the imprint constrains her. She lives within that primordial memory and cannot imagine or think about other solutions. There were no alternatives originally, thus there are none now while awash in the imprint. And the imprint forces her to remain on the same route all over again. Her hopelessness (depression) is all-consuming. She cannot stray outside its bounds. The stabs of depression she suffers are reminders of the mounting memory that periodically surges upwardly toward awareness. There is no way to know now exactly why she killed herself. But a clue to her motive can be found post-mortem, in the manner in which she chose to kill herself. Scott had just about everything in life; although she was in debt, she lived well and lived high with Jagger. Yet she took the trouble to go through the machinations of hanging. Why not take the simpler “way out,” with pills? Though some will find this hard to believe, the answer goes back to the very beginning of life: the way in is often the way out. The same imprint that produced deep hopelessness at birth – the root of depression – is also what likely led to her to choose hanging. I am not familiar with the circumstances of Scott’s death, but I am not limiting my discussion only to her. This applies to all of us. The fact of the deep imprint also can lead to hanging for if she were strangling on the cord she is most likely to repeat the act. It was the closest she came to death and the trauma and its consequences remain. Fifty years ago, I wrote about methods of suicide and I noted that they followed the deep imprint. Being strangled on the cord would lead to hanging. Being suffocated in the womb might lead to gassing oneself. Being mangled at birth might end in jumping off a building or in front of a train. A mother drugging herself might be duplicated in suicide by an overdose of pain-killers in the offspring. Thus, the imprint, now embedded, searches out its duplicate, like most act-outs. And act-outs follow the imprint closely because there is a sense of approaching death early on, and it follows by approaching death now, where death is the final relief from this catastrophic imprint. That is also an imprinted memory – final relief. It is the final denouement of the imprint. Recent research has confirmed the link between the nature of trauma at birth and the manner of suicide chosen in adulthood. In a study published in the journal Biology of the Neonate, K. J. S. Anand and associates state that in a number of suicides by violent means “the significant risk factors were those perinatal events that were likely to cause pain in the newborn.” (Anand & Scalzo, 2000). (2) In other words, suicides will often choose a method that reflects the prototype of their birth experiences. Why? Because each prototype requires its own conclusion. For a neonate strangling on the cord, further strangling would have ended the agony. Those drowning in amniotic fluid at birth may opt for death by drowning. Those who received a massive dose of anesthetic at birth may take an overdose of barbiturates, or they might gas themselves in their garage. And so on. Not every rule can be followed slavishly, as it is here. People do commit suicide also depending on current circumstances; being on a tall building, for example. I offer this heuristically only as a frame of reference toward clarity. I remember one patient who saved up dynamite; having experienced anoxia at birth, he was going to put a stick to his head and blow his head off so that he wouldn't have one second of pain and hopelessness. He laughs at that now, but at the time it spoke volumes of his desperation. Another patient was obsessed with jumping off a building. During her birth by Cesarean, this person had felt wrenched into space with nothing to hang onto. Another patient, battered and squeezed at birth, obsessed about jumping off a bridge, head first. I found this was almost a universal law: we attempt to die in the way our birth was threatened. Those memories, that of trauma during gestation, last a lifetime and lead to same attempt years later to die in the way it might have happened at the beginning. In other words, as the memory of the early trauma rises, the memory of the early result mounts as well. Thus early strangulation may lead to the same course of action with the final denouement; death. The logic of the system. It is confirmation of the imprint and its lifelong effect on the system. It drives behavior ineluctably. So the imprint includes the probable outcome – death. We need to consider suicide as another form of act-out. It channels behavior despite exhortation and encouragement; the sense of approaching death. What is often articulated for those who have no idea about the imprint is, “I don’t want to live anymore.” And even that is not fully articulated; it is usually a vague thought or sense. It is often not, “I am in so much pain I don’t want to go on.” It is just a vague sense of hopelessness and helplessness that leads to an attempt. It all remains vague and aleatory, a constant rumination inside of a black cloud descending. It is difficult, perhaps, to believe that birth problems can give rise to suicidal tendencies years later. This is because we are not used to thinking about physiologic memory. Nor are we used to thinking that the most powerful memories we have are those without words, memories of events which predated our ability to understand what was happening to us. It's not always the case that the suicide method mimics the birth trauma, of course, but it is often what we discover in talking to and observing our patients. If we want to get an idea about our birth, look at our imagined choice of suicide. Conversely, if we want to know the origins of depression, we might examine the birth epoch. Eventually, we may discover the secrets of our beginnings in life.
Suicidal or Self-Destructive There are some acts of suicide that are a cry for help, taking a certain amount of sleeping pills, for example. And there are others that say, I really don’t want to live anymore; that is a jump off a bridge. That is final, no call for help. It all seems so helpless and hopeless; they want to die for relief. No more pain; that’s enough. Their pain is importuning and relentless. Because so is the imprint. No immediate escape, as there might not have been during the original trauma. The pain is so devastating and militating to higher levels that the person cannot contemplate other options. Those feelings are terrible, and they say to us, “Life is terrible.” No it’s not, a therapist may say in an attempt to steer the patient’s mind away from desperate thoughts. But if we try to argue the person out of those thoughts we are using the wrong brain. Our words can never reach the wordless pain they are in. Yet counseling can be a help, although not a cure. It offers help against feeling helpless and hope against hopelessness. It means someone cares and wants you to live. Crucial. There are some cases where it was impossible to try; further trying might have been life-endangering. Here lies the “loser.” Everything is too much and he gives up automatically. The whole parasympathetic nervous system dominates and directs, and leads him to a passive lifestyle. Why doesn’t get up and get going? He cannot. He is blocked by a memory of action is dangerous. This is not a fantasy; it is real history he is fighting and he lost originally and he will lose again. His depression deepens as he seems stuck in life and can find no way out. He needs to be led, encouraged; to have life breathed into him. In many suicide cases, it turns out victims had suffered some sort of oxygen deficit early on, caused perhaps by a heavy dose of anesthesia to the mother or by being strangled on the cord at birth. And after an agonizing attempt to get born, death approaches and there is a sense of impending doom and then relief. That memory of possible relief is sealed in so that later in the face of utter hopelessness – triggered by an impending divorce, for instance – death becomes the answer. So an attempt at suicide follows. It is a memory of possible relief, stamped in, engraved that endures for a lifetime. It is the end of the chain of pain, as it were, the logical denouement when current hopelessness can set off the primordial hopelessness where death lurks. How is it that hopelessness today sets off the same feeling during birth? It is again the chain of pain, the links between levels of consciousness. One way we see that link is through resonance; the current feeling sets off the same deeper feelings until the whole system is engulfed in utter hopeless feelings. And worse, there is no scene attached to it as it is pure feeling, naked and unadorned, the exact same feeling rising again to smother the person and make her suicidal. It is the most profound hopelessness. The current feeling, in short, has triggered off its progenitor with sensations of approaching death becoming paramount. That early hopelessness is later expanded and ramified as the whole system and brain mature. As each new brain system comes on line, it adds its emotional weight to the feeling. But it is the same feeling with increased maturity and neuronal development. It is the system’s effort to suppress the feeling that produces depression. So depression is not a feeling; it is what happens as that feeling is blocked from higher level access. And when we unravel depression that is what we find: utter, unarticulated hopelessness. We get confirmation by drops in body temperature and blood pressure, a sign of giving up. That foretells a suicidal attempt. However, it can be felt and relived with all of its pain, which provides the ultimate relief as the depression begins to leave, at last. This is not done in a day because it is very deep, the end point of the birth agony, a cord around the neck, for example. This means that we must not trump evolution and feel it soon in therapy. And if we do not take care to go slowly we will touch the embed too early and abreaction results. Why? Because the patient is not ready for that much pain. We can only feel it as the body and brain allow, current hopeless feelings first, then the childhood compounding and finally, the first line, brainstem component where the deepest feelings always lie. I use the word “compounding,” because these are not different feelings; they are the same feelings laid down and layered at different stages of development, and connected through resonance. The child just seems unhappy and sullen and no one knows why. And certainly the child has no idea at all, nor do his teachers. He is in the grasp of that early devastating feeling that no one can say its name. It is literally “ineffable.” The feeling cannot respond to encouraging words because discouraging feelings take priority. Suddenly, one day in therapy while the patient is feeling deeply about childhood events where he was blocked for whatever he wanted to do, he shifts into choking and suffocation; the precursor is on its way. It says, “I am strangling on the cord.” Only it does not say it for the moment. The patient is in the grips of first-line, brainstem imprints which only later can he give it a name and context. For the moment the patient only senses the physical sensations. As the body experience enters resonance again and moves higher in the nervous system, where words and thoughts become available, then he knows it is the cord that is stopping me from breathing. That cord has imprinted the trauma, and with the sensation of suffocation together with hopelessness and helplessness. How does he know? The inevitable concomitant of this is during the Primal he again sinks into deep hopelessness, and with it a lowering of core body temperature. It can go down several degrees, and, happily, after the feeling it can normalize and rise to higher levels again. But the body nearly always follows suit in these situations; not just the mind at work. And they never say, “I feel depressed.” It is evident in all of their demeanor. Even how they breathe; it gets more and more shallow as conservation of oxygen takes over during the session as the patients goes deeper, approaching the primal imprint. What has this to do with self-destruction, as some therapies describe the suicide attempt? I was discussing the difference between self-destructive behavior and suicide with a colleague. They are quite different, although you would think that suicide is destruction of the self, but it is not at all like that. Let’s take literal destruction, cutting oneself. This is a later ploy, making hurt obvious. It is a plea for help; “Please see my hurt. See that I hurt.” This in lieu of screaming out that hurt. And the cutter is not often aware of what she is doing or why. It was never acknowledged by anyone because perhaps the parents had no idea of that hurt or even that such emotional hurt existed. There are many aspects of this. Her feeling was, “I’m trying to let the hurt escape,” even when she had no idea what it was. She just knew it was inside and it had to come out. Another woman, a self-cutter. told me that she cut because it took away some of the emotional hurt which was more painful. It had a beginning and an end. It was controllable whereas the emotional hurt just kept going on. She found out that it was exactly what we do; letting pain out: but in methodical ways so she no longer had to cut herself. The feeling has to be felt deeply to match the force of the pain involved. The patient is trying to let the pain out in the only way she can; make it visible and palpable. If you can at least see it there is something you can do about it. When there are later circumstances of neglect and lack of love, the deep imprints become compounded and cemented in. Those later traumas (lack of love) increase the repression and force unconscious acting out, such as cutting oneself, to try to get at the source, hopefully, yet unconsciously. But suicide is still a long way off. It is amazing how so often people cut themselves, unwittingly digging out the source of their suffering without even knowing what they are doing. Suicide, then, is a deeper, earlier sensation/feeling with no behavioral possibilities. They are, indeed, two different things. Even though suicide attempts to destroy the self it is not, oddly, self-destructive. And of course, self-destructivenessit ramifies so that the destructive behavior takes on many forms, such as sabotaging one’s own success or always picking toxic partners. But it is not as direct as suicide. Suicide means one final act. It is not anything in the present that causes it; it is the result of a deep memory. There are myriad examples of self-destructive behavior, but all the manifestations come from subdued feelings. There are people who set themselves up for certain failure, who always make sure things turn out bad, who drink themselves into oblivion or who repeatedly get involved with a low-lives they know are bad for them. Here the driving forces are nearly always deep-seeded pain. These are secondary effects of imprinted hurt. Driving with drunk drivers is a good example.
Another is the case of a graduate student who could not get feedback from his professors for a paper he had turned in. After weeks of “trying to get through” he sent a most nasty letter to the instructor. For that, he was delayed in getting his degree. So he shot himself in the foot because he could never get through to his father and also because he literally couldn’t get through in being born. Being blocked from getting what he wanted and needed had set off a rage in him, and as we know rage is first line, brainstem originated. It is the seat of the most atavistic anger possible. He was helpless before this surge of fury. Resonance reached down and dredged it all up, surging upwards beyond control. He knew when he sent the letter it was wrong; this is what used to be called “emotional.” His emotions got the best of him. They weren’t irrational; they were real but buried deeply.
The Relief of Reliving In Primal Therapy, we seek access to those deep recesses of the brain, where ultimate healing lies. First-line is always more powerful than later imprints; and they are the most healing, offering up many insights that previous behavior was based on. The insights that flow from first-line feelings are widely encompassing because they are the basis for so much later behavior. Reliving on the brainstem level means complete connection as the driving force of impulses are experienced at last. We connect, in short, on the level of the trauma and in that context only. Here we are dealing with the shark brain: no shouts, no wild movements; evolution has taken over. It means the patient has gone back in time and is living again what went on decades before. Then it was too overwhelming for a naïve and fragile infant brain to integrate. Now, perhaps, he is ready for it. That is the true meaning of facing yourself and accepting yourself; not in the booga-booga, new-age sense but in the biologic evolutionary meaning of it, where the feeling is now integrated into the physical system. It becomes ego syntonic. That is the real meaning of becoming oneself. As the reliving goes on, the feeling is fully integrated and there is a continued drop in vital signs and body temperature lowers to real normal, rather than “average” normal. In this sense, “integration” is a new biologic state where the whole system can re-regulate itself. Normalization has set in and depression bids adieu. And no one has done anything outside the body. It all originated from inside. That is why I say that everything the patient has to learn is already inside, waiting. In Primal Therapy, we get patients gradually down to those deep feelings that are so disturbing. And once those feelings are resolved and brought to consciousness, there are no more thoughts of suicide. Why? Because there are no more buried feelings driving the suicidal thoughts. It takes time, but when they get there, they discover real relief, the kind that lasts and lets them live.
I am not writing as the shoemaker who sees only shoes in the world but as a therapist who has seen patients relive birth hundreds of times and know what an impact it has. Let us not shy away from a key reality of our lives and adopt a rebirthing therapy that is ineffective and sometimes quite dangerous.
“The question of what has driven the increases is unresolved, leaving experts to muse on the reasons,” states the New York Times in an article about the suicide data.(1)
And so they speculate. Maybe it’s the rising divorce rate, or the lower rates of marriage. Maybe it’s the worsening economy or the new limits on social mobility. Or maybe it’s the country’s weak suicide prevention network.
They can’t find the answers, I believe, because external factors are not the cause; they are just the trigger. After all, many people get divorced and lose their jobs and their homes, or worse, but don’t decide to end their lives. The explanation is elusive because the causes are hidden. They lie deep inside the desperate individuals who see no way out but death, and who may not even know what is driving their desire to take their own lives.
The best way to illuminate the problem is to look at it from the other side. Set aside for a moment those poor souls who are suffering obvious misfortunes. Consider instead those apparently lucky people who have it all, but still choose to end it all. Why do so many celebrities commit suicide?
Suicide and Success
Celebrity suicides always strike us as a mystery. These are successful, wealthy people we admire and emulate. We even try to be like them. So when the rich and famous find their lives too much to bear – as did L’Wren Scott, the high-end fashion designer and girlfriend of Mick Jagger – we inevitably wonder why. Scott hanged herself in the multi-million apartment she had shared with Jagger in New York. She didn’t leave a note. Her friends, who described her as kind and considerate, were shocked. Jagger, who was on tour with the Rolling Stones in Australia, issued a statement claiming he was "still struggling to understand how my lover and best friend could end her life in this tragic way." Everyone was asking the same question.
There have been a number of people who have committed suicide who seemed at the pinnacle of success. And most of us thought that once we choose a profession and follow it and succeed at it, becoming an expert and well known, that would be fulfilling. We would feel like a success. Wrong. When we have deep-rooted lack of love, rejection, indifference and lack of touch early in our lives we cannot feel like a success. We can only feel what was left embedded in us as an imprint: the feeling of being unloved, empty, isolated, unwanted. That is always primary. All else and all later feelings lie on top of the imprint. We need to keep in mind that the imprint is embedded very early in life when the struggle has a life-or-death quality. It takes precedence over any later adversity. The memory is of a life-endangering event. It is not an imaginary time; survival is at stake (lack of oxygen at birth). And later, even the slightest threat takes on the original force of the reaction. Through resonance (the linkage between high nerve pathways and lower ones) terror is again elicited. What is set off? The feeling tone, for feelings are primary very early in life, long before we develop an overall sense of the total context. But the feeling tone will be an augury of a trauma gone by, and also a pathway to the past where the tone originated, engendered by perhaps an overdose of anesthetic to the mother for her pain but is far, far too much for a six-pound baby. That tone (hopelessness) may well underlie later depression, which seems such a mystery. But we are immersed in a sense of “what’s the use?” There is no reason to try or to go on; we are trapped in that imprinted memory where it was hopeless. This imprint may well be the template for building even stronger hopelessness when other needs are not fulfilled such as being held and soothed. And what do we do when we are bereft of that knowledge of the lingering tone? A tone due to its immense impact remains unconscious, repressed by the forces that are elicited to keep us from feeling devastating agony. We seek to submerge it further with drugs. We do the opposite of what is required, which is to release that memory from its neurobiologic cage. But when we observe it with all its power it seems overwhelming. This is why we are working with some medications to ameliorate the impact of that pain so it does not have to be experienced with all its fury. There is only one way to stop the suffering, and that is to revisit the imprint and relive the pain. Until then, we cannot know the real lack and what it is. That is why the system insists on reliving later in life. Our own system is pushing for real integration and liberation, because it seeks to become whole again. That imprint has only one goal in life; to be relived exactly as it was laid down. To finish the unfinished job of integrating what was repressed and put aide at its origin. Its message is a constant warning of unfinished business. The pain from very early on has to be felt and dealt with in all its agony and terror. The imprint knows no mercy. It wants conscious awareness somewhere inside even while the top cortical level does what it can to imprison it. Conscious awareness means delving into deep feeling plus ultimate awareness of what it is. The imprint will never leave until it is lived again, fully, in its original context. Enough rearranging of the chairs on the Titanic. We must join feelings with their thoughts and make ourselves whole. Fame won’t do that; I have treated enough stars to know that, and my patients also know it. There is no substitute for extirpating the imprint. None. Avoiding the imprint and we are leaving misery in place. Reliving it finally stops the terrible drive to feel like a success; to run from the feeling. That is different from being authentically successful, which is the drive to do things right. A little more relaxing.
To be loved early on, that is what sets the stage for your life. It means fulfilling basic needs as they evolve; it makes us feel confident and productive, but not driven. It offers daring and enthusiasm and a joie de vivre. It allows us to try but never in desperation. Symbolic love – the kind we get from fame and celebrity – has to be repeated over and over exactly because it cannot fulfill. Why not? Precisely because it is symbolic, a substitute for the true love we never got from our parents. When there is a basic lack of fulfillment early in life, especially during gestation, birth and infancy, an imprint is created that stamps in that deprivation, through the partially open sensory window. That imprint is embedded deep in the brain and stays there, almost inaccessible. We are aware only of a gnawing emptiness, feeling unfulfilled. Empty like a shell, as one patient put it. And that need, now un-anchored from its source, drags us into the race for symbolic fulfillment. But it’s a race that never ends because it does nothing to alter the motor that’s driving it, which is the painful, buried imprint of getting no love when it really mattered. No hugs, no attention, no sympathy, no understanding, nada. No love. And that compounds and builds into a massive forceful load of unconsciousness. For most us, given a bit of hope for love we are galvanized. But those with deep implacable hopelessness it seems to be a signal to give up; the original reaction that was life saving. Again, the basic survival imprint. Once the pain is embedded and out of reach, we will seek out substitutes, so as to stop feeling empty and unloved. The agony from that deep, deep pain becomes a primordial part of us. It now confuses us, distracts us, and above all, stops our concentration. Oh yes; it depresses us because we live with an enemy in the house that we cannot escape. It lives with us and in us; it claws for its liberation; it wants freedom to live the pain, believe it or not. Yet we do what we can to stop it. No wonder most psychotherapy is aimed at repression and rationales, and understanding but never deep feeling. Patients get a bit of relief, which the he settles for; but no cure. So what does the successful person feel? Very little: Down, unhappy and unfulfilled. He has no other choice because those feelings will not leave even for mercy’s sake. Mercy has no part in the lexicon of the unconscious; it follows the road to what seemed to work originally. Freud called it The Repetition Compulsion. Let us never forget the enormous pull of that embedded hopelessness low in the nervous system. It drags us down toward the non-integrated feeling that might have occurred when the newborn was heavily dosed with anesthetics; or earlier there might a smoking mother or one who drank all of the time. Or worse, a carrying mother who took constant painkillers, which diminished oxygen supplies. This, inter alia, also, drugged the baby and affected his breathing and energy levels. The drugs infused into the baby again drains him of effort and will power. He may be born passive, inactive and unresponsive. His whole being has given up against insuperable odds. And that erupts the minute he must make any strenuous effort. All this keeps him from feeling like a success; “I can do and succeed”.
Success is not a real feeling; being loved is. Fame is other people’s idea of our achievements; it is in a way their feeling… Admiration, humble, important, etc. And why does even the most accomplished person never feel satisfied nor fulfilled? Because all of his fulfillment and all of his admiration is symbolic; it is not the love he needed early on. It covers
Finally at the top of his fame he feels still unfulfilled and a failure; there is nothing more to gain, nothing more to try for. He looks at all his billboards and feels empty. What does it mean? “I don’t know what else to do to feel good, to feel successful.” It seems that life is empty. There is no point; suicidal thoughts thrust their way in, as he feels the real deep feeling of hopelessness and helplessness that he has been escaping from in his work. The pain that drove it all is still alive and gnawing inside. It says, sotto voce, you are not loved and that is all that matters. Something is missing and you have no idea what that is. You have failed at what matters most; to be adored, admired, encouraged, held and caressed. That is the constant malaise that speaks of something missing. “All your drive was to try to escape the imprinted feeling and feel loved, and you believe you are, but not by the people who really matter, and not at the time when love was a life-or-death affair. There is a critical window for love to happen and a special time when the system is at its asymptote of need. When the critical time has passed repression takes over; it is too late now for fulfillment so there is no choice; symbolic fulfillment takes place; the ever-present audience who adores.
I treated one film director who became seriously depressed when he was no longer on stage. He felt useless, unneeded and unwanted; he started to feel his old feelings once again, only before therapy he drugged his hopelessness and now in therapy he is feeling it for what is really is. He began to feel the childhood part of the pain with parents who did not want him around; he was convinced there was something seriously wrong with him. This lay on top of the earlier pains of a sense of dying, of suffocating and losing consciousness. But not being needed on set began the whole process all over again. The first part was the feeling of “I will die if I am not loved,” and then much later, “I am dying and there is nothing I can do to escape.” This was the ultimate helplessness and hopelessness, the key elements of depression. Resonance always involves the chain of pain; the neuronal linkage from one set of neural processes to another. It is why something innocuous can set off catastrophic feelings.
As I have written à maintes reprises, many times over, we respond primarily and firstly to apparent problems in the present, and later to inner links that are awakened by those current problems, such as job losses or divorce. Those repressed traumas are ready to fire and when those links fire together they become wired together, solidified. That is the process I call resonance. The body and brain are busy reacting to what happened decades earlier during womb-life and birth. Those are the events we continually react to because of their remoteness, something that occurred when we were vulnerable and easily and heavily impacted. This is not only my hypothesis. Within the past 20 years, there have been literally hundreds of studies verifying the importance of early imprints, how they last a lifetime and alter our systems. Imprints lay down engraved memories that show themselves when we are alone, in a weakened state or otherwise too open to events.
That is what I believe may have happened to L’Wren Scott in those moments alone before she took her life. She must have had an inkling, a deep down unease and hopeless feeling that would have warned her. It was all hidden inside her, pushing through her weakened defense layers and making her feel so hopeless and “down,” despite her current surroundings. Being alone for a short time can set off being left and abandoned as a child; this is only surmise for now since I have not idea about this but I have seen in my patients. It can first set off, “I am all alone and no one to hold and comfort me.” Just a few hours alone with no one nearby can do it. Remember, small things can set off huge feelings. If she were left alone and neglected by her parents very early on, the connection to despair of the past it becomes clear.She probably had no idea about imprints or deep-lying trauma/memory. That is the reason our theory is so important, so that people who are suffering can be aware of what is going on inside and understand where their despair and suicidal thoughts come from. This may avoid needless deaths. How tragic and unnecessary all this. And now you understand our mission: not money nor fame, but the lives of us humans. We all have a basic right to a full-length life. The Way In Is The Way Out
You may wonder why a privileged and wealthy celebrity can’t find distractions for her despair. Why doesn’t she run away or go to parties and “take her mind off of it?” She cannot; the imprint constrains her. She lives within that primordial memory and cannot imagine or think about other solutions. There were no alternatives originally, thus there are none now while awash in the imprint. And the imprint forces her to remain on the same route all over again. Her hopelessness (depression) is all-consuming. She cannot stray outside its bounds. The stabs of depression she suffers are reminders of the mounting memory that periodically surges upwardly toward awareness. There is no way to know now exactly why she killed herself. But a clue to her motive can be found post-mortem, in the manner in which she chose to kill herself. Scott had just about everything in life; although she was in debt, she lived well and lived high with Jagger. Yet she took the trouble to go through the machinations of hanging. Why not take the simpler “way out,” with pills? Though some will find this hard to believe, the answer goes back to the very beginning of life: the way in is often the way out. The same imprint that produced deep hopelessness at birth – the root of depression – is also what likely led to her to choose hanging. I am not familiar with the circumstances of Scott’s death, but I am not limiting my discussion only to her. This applies to all of us. The fact of the deep imprint also can lead to hanging for if she were strangling on the cord she is most likely to repeat the act. It was the closest she came to death and the trauma and its consequences remain. Fifty years ago, I wrote about methods of suicide and I noted that they followed the deep imprint. Being strangled on the cord would lead to hanging. Being suffocated in the womb might lead to gassing oneself. Being mangled at birth might end in jumping off a building or in front of a train. A mother drugging herself might be duplicated in suicide by an overdose of pain-killers in the offspring. Thus, the imprint, now embedded, searches out its duplicate, like most act-outs. And act-outs follow the imprint closely because there is a sense of approaching death early on, and it follows by approaching death now, where death is the final relief from this catastrophic imprint. That is also an imprinted memory – final relief. It is the final denouement of the imprint. Recent research has confirmed the link between the nature of trauma at birth and the manner of suicide chosen in adulthood. In a study published in the journal Biology of the Neonate, K. J. S. Anand and associates state that in a number of suicides by violent means “the significant risk factors were those perinatal events that were likely to cause pain in the newborn.” (Anand & Scalzo, 2000). (2) In other words, suicides will often choose a method that reflects the prototype of their birth experiences. Why? Because each prototype requires its own conclusion. For a neonate strangling on the cord, further strangling would have ended the agony. Those drowning in amniotic fluid at birth may opt for death by drowning. Those who received a massive dose of anesthetic at birth may take an overdose of barbiturates, or they might gas themselves in their garage. And so on. Not every rule can be followed slavishly, as it is here. People do commit suicide also depending on current circumstances; being on a tall building, for example. I offer this heuristically only as a frame of reference toward clarity. I remember one patient who saved up dynamite; having experienced anoxia at birth, he was going to put a stick to his head and blow his head off so that he wouldn't have one second of pain and hopelessness. He laughs at that now, but at the time it spoke volumes of his desperation. Another patient was obsessed with jumping off a building. During her birth by Cesarean, this person had felt wrenched into space with nothing to hang onto. Another patient, battered and squeezed at birth, obsessed about jumping off a bridge, head first. I found this was almost a universal law: we attempt to die in the way our birth was threatened. Those memories, that of trauma during gestation, last a lifetime and lead to same attempt years later to die in the way it might have happened at the beginning. In other words, as the memory of the early trauma rises, the memory of the early result mounts as well. Thus early strangulation may lead to the same course of action with the final denouement; death. The logic of the system. It is confirmation of the imprint and its lifelong effect on the system. It drives behavior ineluctably. So the imprint includes the probable outcome – death. We need to consider suicide as another form of act-out. It channels behavior despite exhortation and encouragement; the sense of approaching death. What is often articulated for those who have no idea about the imprint is, “I don’t want to live anymore.” And even that is not fully articulated; it is usually a vague thought or sense. It is often not, “I am in so much pain I don’t want to go on.” It is just a vague sense of hopelessness and helplessness that leads to an attempt. It all remains vague and aleatory, a constant rumination inside of a black cloud descending. It is difficult, perhaps, to believe that birth problems can give rise to suicidal tendencies years later. This is because we are not used to thinking about physiologic memory. Nor are we used to thinking that the most powerful memories we have are those without words, memories of events which predated our ability to understand what was happening to us. It's not always the case that the suicide method mimics the birth trauma, of course, but it is often what we discover in talking to and observing our patients. If we want to get an idea about our birth, look at our imagined choice of suicide. Conversely, if we want to know the origins of depression, we might examine the birth epoch. Eventually, we may discover the secrets of our beginnings in life.
Suicidal or Self-Destructive There are some acts of suicide that are a cry for help, taking a certain amount of sleeping pills, for example. And there are others that say, I really don’t want to live anymore; that is a jump off a bridge. That is final, no call for help. It all seems so helpless and hopeless; they want to die for relief. No more pain; that’s enough. Their pain is importuning and relentless. Because so is the imprint. No immediate escape, as there might not have been during the original trauma. The pain is so devastating and militating to higher levels that the person cannot contemplate other options. Those feelings are terrible, and they say to us, “Life is terrible.” No it’s not, a therapist may say in an attempt to steer the patient’s mind away from desperate thoughts. But if we try to argue the person out of those thoughts we are using the wrong brain. Our words can never reach the wordless pain they are in. Yet counseling can be a help, although not a cure. It offers help against feeling helpless and hope against hopelessness. It means someone cares and wants you to live. Crucial. There are some cases where it was impossible to try; further trying might have been life-endangering. Here lies the “loser.” Everything is too much and he gives up automatically. The whole parasympathetic nervous system dominates and directs, and leads him to a passive lifestyle. Why doesn’t get up and get going? He cannot. He is blocked by a memory of action is dangerous. This is not a fantasy; it is real history he is fighting and he lost originally and he will lose again. His depression deepens as he seems stuck in life and can find no way out. He needs to be led, encouraged; to have life breathed into him. In many suicide cases, it turns out victims had suffered some sort of oxygen deficit early on, caused perhaps by a heavy dose of anesthesia to the mother or by being strangled on the cord at birth. And after an agonizing attempt to get born, death approaches and there is a sense of impending doom and then relief. That memory of possible relief is sealed in so that later in the face of utter hopelessness – triggered by an impending divorce, for instance – death becomes the answer. So an attempt at suicide follows. It is a memory of possible relief, stamped in, engraved that endures for a lifetime. It is the end of the chain of pain, as it were, the logical denouement when current hopelessness can set off the primordial hopelessness where death lurks. How is it that hopelessness today sets off the same feeling during birth? It is again the chain of pain, the links between levels of consciousness. One way we see that link is through resonance; the current feeling sets off the same deeper feelings until the whole system is engulfed in utter hopeless feelings. And worse, there is no scene attached to it as it is pure feeling, naked and unadorned, the exact same feeling rising again to smother the person and make her suicidal. It is the most profound hopelessness. The current feeling, in short, has triggered off its progenitor with sensations of approaching death becoming paramount. That early hopelessness is later expanded and ramified as the whole system and brain mature. As each new brain system comes on line, it adds its emotional weight to the feeling. But it is the same feeling with increased maturity and neuronal development. It is the system’s effort to suppress the feeling that produces depression. So depression is not a feeling; it is what happens as that feeling is blocked from higher level access. And when we unravel depression that is what we find: utter, unarticulated hopelessness. We get confirmation by drops in body temperature and blood pressure, a sign of giving up. That foretells a suicidal attempt. However, it can be felt and relived with all of its pain, which provides the ultimate relief as the depression begins to leave, at last. This is not done in a day because it is very deep, the end point of the birth agony, a cord around the neck, for example. This means that we must not trump evolution and feel it soon in therapy. And if we do not take care to go slowly we will touch the embed too early and abreaction results. Why? Because the patient is not ready for that much pain. We can only feel it as the body and brain allow, current hopeless feelings first, then the childhood compounding and finally, the first line, brainstem component where the deepest feelings always lie. I use the word “compounding,” because these are not different feelings; they are the same feelings laid down and layered at different stages of development, and connected through resonance. The child just seems unhappy and sullen and no one knows why. And certainly the child has no idea at all, nor do his teachers. He is in the grasp of that early devastating feeling that no one can say its name. It is literally “ineffable.” The feeling cannot respond to encouraging words because discouraging feelings take priority. Suddenly, one day in therapy while the patient is feeling deeply about childhood events where he was blocked for whatever he wanted to do, he shifts into choking and suffocation; the precursor is on its way. It says, “I am strangling on the cord.” Only it does not say it for the moment. The patient is in the grips of first-line, brainstem imprints which only later can he give it a name and context. For the moment the patient only senses the physical sensations. As the body experience enters resonance again and moves higher in the nervous system, where words and thoughts become available, then he knows it is the cord that is stopping me from breathing. That cord has imprinted the trauma, and with the sensation of suffocation together with hopelessness and helplessness. How does he know? The inevitable concomitant of this is during the Primal he again sinks into deep hopelessness, and with it a lowering of core body temperature. It can go down several degrees, and, happily, after the feeling it can normalize and rise to higher levels again. But the body nearly always follows suit in these situations; not just the mind at work. And they never say, “I feel depressed.” It is evident in all of their demeanor. Even how they breathe; it gets more and more shallow as conservation of oxygen takes over during the session as the patients goes deeper, approaching the primal imprint. What has this to do with self-destruction, as some therapies describe the suicide attempt? I was discussing the difference between self-destructive behavior and suicide with a colleague. They are quite different, although you would think that suicide is destruction of the self, but it is not at all like that. Let’s take literal destruction, cutting oneself. This is a later ploy, making hurt obvious. It is a plea for help; “Please see my hurt. See that I hurt.” This in lieu of screaming out that hurt. And the cutter is not often aware of what she is doing or why. It was never acknowledged by anyone because perhaps the parents had no idea of that hurt or even that such emotional hurt existed. There are many aspects of this. Her feeling was, “I’m trying to let the hurt escape,” even when she had no idea what it was. She just knew it was inside and it had to come out. Another woman, a self-cutter. told me that she cut because it took away some of the emotional hurt which was more painful. It had a beginning and an end. It was controllable whereas the emotional hurt just kept going on. She found out that it was exactly what we do; letting pain out: but in methodical ways so she no longer had to cut herself. The feeling has to be felt deeply to match the force of the pain involved. The patient is trying to let the pain out in the only way she can; make it visible and palpable. If you can at least see it there is something you can do about it. When there are later circumstances of neglect and lack of love, the deep imprints become compounded and cemented in. Those later traumas (lack of love) increase the repression and force unconscious acting out, such as cutting oneself, to try to get at the source, hopefully, yet unconsciously. But suicide is still a long way off. It is amazing how so often people cut themselves, unwittingly digging out the source of their suffering without even knowing what they are doing. Suicide, then, is a deeper, earlier sensation/feeling with no behavioral possibilities. They are, indeed, two different things. Even though suicide attempts to destroy the self it is not, oddly, self-destructive. And of course, self-destructiveness
The Relief of Reliving In Primal Therapy, we seek access to those deep recesses of the brain, where ultimate healing lies. First-line is always more powerful than later imprints; and they are the most healing, offering up many insights that previous behavior was based on. The insights that flow from first-line feelings are widely encompassing because they are the basis for so much later behavior. Reliving on the brainstem level means complete connection as the driving force of impulses are experienced at last. We connect, in short, on the level of the trauma and in that context only. Here we are dealing with the shark brain: no shouts, no wild movements; evolution has taken over. It means the patient has gone back in time and is living again what went on decades before. Then it was too overwhelming for a naïve and fragile infant brain to integrate. Now, perhaps, he is ready for it. That is the true meaning of facing yourself and accepting yourself; not in the booga-booga, new-age sense but in the biologic evolutionary meaning of it, where the feeling is now integrated into the physical system. It becomes ego syntonic. That is the real meaning of becoming oneself. As the reliving goes on, the feeling is fully integrated and there is a continued drop in vital signs and body temperature lowers to real normal, rather than “average” normal. In this sense, “integration” is a new biologic state where the whole system can re-regulate itself. Normalization has set in and depression bids adieu. And no one has done anything outside the body. It all originated from inside. That is why I say that everything the patient has to learn is already inside, waiting. In Primal Therapy, we get patients gradually down to those deep feelings that are so disturbing. And once those feelings are resolved and brought to consciousness, there are no more thoughts of suicide. Why? Because there are no more buried feelings driving the suicidal thoughts. It takes time, but when they get there, they discover real relief, the kind that lasts and lets them live.
I am not writing as the shoemaker who sees only shoes in the world but as a therapist who has seen patients relive birth hundreds of times and know what an impact it has. Let us not shy away from a key reality of our lives and adopt a rebirthing therapy that is ineffective and sometimes quite dangerous.


February 26, 2017
Can Feelings Hurt?
I know that feeling certain feelings causes pain but can feelings hurt? Are there special feelings that make us hurt. Oh yes, and there are levels in the brain that engender more and more pain the deeper we go in the brain. And how do you go deeper and deeper in the brain? Can we go deeper voluntarily, by an act of will? Never. Because an act of will is inimical to feeling deep feelings. The more we want and try to do it, the less deep we can travel. We are then using the last bit of brain evolution to reach the first bit of brain in evolution. Between those levels are gating systems, chemicals that block pain, that block one level from another. If we did not have that mechanism, we would all have a hard time keeping pain down. And when the deep brainstem levels has been dredged up, it means we need heavier pain killers to keep us somewhat comfortable. It is on that level that heavy addiction takes place because it is on that level that heavy pain resides. And that is the pain stirred up in the earliest period of our lives. It lies on the level of pure agony equal to the pain/terror experienced by the shark brain. That deep brain system has the great capacity to feel and also repress pain. Above all, the brain system must try to equal the pain output. When various pains are compounded and accumulate, they become an overload, a challenge to the faltering defense system, and suffering sets in, as does the urgent call for taking exceptionally powerful pain killers. There is just so much hurt we can take before the system falters and cannot do its job. I call that first-line pain. It is often life-endangering pain; an attack by another great predator who sees the shark as a proper meal. Or human hunters who chase and hunt for bragging rights; to be the most macho of men. Diabolically, as he is able to kill without another thought, he is already well repressed and cannot begin to feel what he is doing.
Let us look at the experiment that set this off. It was done at the Michigan University Medical School, in 2013. They studied students who expressed an attraction to certain other students. The subjects then entered an MRI machine and were told that the person they were describing was not interested in them. It is a bit more detailed but in principle, it is the essence of the study. The investigators (led by Dr. David Hsu) were after…… Rejection. They focused on the mu(μ) opioid receptors (think heroin). When someone feels hurt he uses the same biologic system and nerve pathways as with physical hurt. There is the release of chemicals that damp down and cap pain. They are twins, pain and its antagonist. It seems that the same pathways for physical pain are the ones that are also for emotional pain such as rejection. But there is much more to the story, which highlights the problem with laboratory research.
In our clinical research we found pain on levels unimaginable, emanating from deeper levels than the limbic/feeling system. And what happens as patients begin to relive these horrors from deep in the brain the pain builds as does the gating function, as well. And this is the kind of emotional level that is not often reached in researching pain. It is the terror from the threat of impending death, pain that equals the birth trauma that we have seen for fifty years in our work in Primal Therapy. Still, we see that emotional pain does have serious emotional components. And this can mean that as emotional pain gets embedded in the neurologic system it can ramify throughout the system, creating physical havoc. This level of pain is truly ineffable and has no verbally descriptive equivalent. From this, we may see serious physical afflictions such as cancer. Again, the pain from pre-verbal life is catastrophic and can lead to equally catastrophic disease. Let me repeat: the reason for serious catastrophic disease later in life is because there is a pileup of compounded pain pushing it. The agony I have seen in reliving early rejection, as in not being held or touched soon after birth is, I can think of no other word; ineffable. Being rejected by some attractive woman or man is literally of little consequence compared to real rejection by a parent when parental love can be life saving; and a matter of survival. It is the kind of pain we can only see clinically, not concocted in a laboratory. Then and only then can we see why we have back-up systems to control and gate pain.
So feelings can hurt and not just emotionally. They can affect the circulatory and heart system, as well. We must keep in mind that the system we use, the nerve pathways we employ, for both physical and emotional pain are often identical. And when we say, it hurt so much; it really does.
Let us look at the experiment that set this off. It was done at the Michigan University Medical School, in 2013. They studied students who expressed an attraction to certain other students. The subjects then entered an MRI machine and were told that the person they were describing was not interested in them. It is a bit more detailed but in principle, it is the essence of the study. The investigators (led by Dr. David Hsu) were after…… Rejection. They focused on the mu(μ) opioid receptors (think heroin). When someone feels hurt he uses the same biologic system and nerve pathways as with physical hurt. There is the release of chemicals that damp down and cap pain. They are twins, pain and its antagonist. It seems that the same pathways for physical pain are the ones that are also for emotional pain such as rejection. But there is much more to the story, which highlights the problem with laboratory research.
In our clinical research we found pain on levels unimaginable, emanating from deeper levels than the limbic/feeling system. And what happens as patients begin to relive these horrors from deep in the brain the pain builds as does the gating function, as well. And this is the kind of emotional level that is not often reached in researching pain. It is the terror from the threat of impending death, pain that equals the birth trauma that we have seen for fifty years in our work in Primal Therapy. Still, we see that emotional pain does have serious emotional components. And this can mean that as emotional pain gets embedded in the neurologic system it can ramify throughout the system, creating physical havoc. This level of pain is truly ineffable and has no verbally descriptive equivalent. From this, we may see serious physical afflictions such as cancer. Again, the pain from pre-verbal life is catastrophic and can lead to equally catastrophic disease. Let me repeat: the reason for serious catastrophic disease later in life is because there is a pileup of compounded pain pushing it. The agony I have seen in reliving early rejection, as in not being held or touched soon after birth is, I can think of no other word; ineffable. Being rejected by some attractive woman or man is literally of little consequence compared to real rejection by a parent when parental love can be life saving; and a matter of survival. It is the kind of pain we can only see clinically, not concocted in a laboratory. Then and only then can we see why we have back-up systems to control and gate pain.
So feelings can hurt and not just emotionally. They can affect the circulatory and heart system, as well. We must keep in mind that the system we use, the nerve pathways we employ, for both physical and emotional pain are often identical. And when we say, it hurt so much; it really does.
February 25, 2017
The Origins of Anxiety, Panic, and Rage Attacks
Read full article published in Activitas Nervosa Superior here:
http://www.activitas.org/index.php/ne...
http://www.activitas.org/index.php/ne...
February 24, 2017
Mindfulness and Other Nonsense, the Twin Sister of Psychoanalysis
I was thinking about some of the new fads such as Mindfulness and wondering what would be the most succinct way to describe what is wrong with it. Oh, I know, it leaves out a little thing called evolution. If we understand evolution we know that the awareness brain came along last, millions of years after the earlier brains. That brain can disconnect from those early brains and take on a life of its own. It is never the curative brain. Why? Because we now know that traumas very early in our lives are embedded deep down in the brain and leave a trace. They are located far from the brain that is aware, so does mindfulness help you get well? Of course not; it is a shallow shell. It rides above the lower brains and usually does not know anything is down there; certainly not aware of feelings churning away below. So if it is not aware of deep roiling how can awareness improve consciousness, which is the sine qua non of cure. Awareness is a non-depth event and is meant to be the enemy of consciousness. It is the essence of blocking full consciousness of suppressing those forces sequestered below which must be relived; not just understood. Reliving is no longer just my notion but now has a widespread scientific base, acknowledged as the essence of cure. There is no fooling with that, no jiggering or tweaking it; it is unchangeable and unrelenting and uncompromising. To make any real change there must be reliving, and it has to be exactly as the trauma was set down; so who knows that? The patient and only him because when the time is right that imprint will arise in its full glory with all of its feelings to be absorbed and integrated at last. It is those forces that make us very sick and also mentally ill.
It has waited a very long time to breathe the air, to become conscious where all three brains coalesce to make us conscious. Its unceasing roiling below has exhausted it and us and worn down the biologic system. The system is designed not to permanently hide feelings but to bring them up when the system can take it and integrate it. To see the faces of those who have reversed the imprint is to see a face of great relief, openness and joy. Some call it , “getting that monkey off the back” which means unloading Pain. No awareness can accomplish that because it cannot lift the Primal load, cannot unburden us and liberate us from our Primal Chains. Awareness was never meant to plunge to the depths; that is only the role of consciousness. Consciousness means reaching the deepest levels of the brain where the greatest terror and pain reside. We cannot get well with only half a brain at work. We cannot get well when half of our evolution is neglected and not considered part of us. But until we are fully ready, awareness can help mask our pain as we go through the motions of getting better which will forever be an elusive target. We cannot get there from here. Cannot get well looking at the brain from on top and believing we are treating the whole person, whereas we are treating the person’s later life, the slim slice of life that came along after many of the imprints were laid down.
Don’t think psychotherapy, insight therapy and psychoanalysis can escape; they suffer from the same rationales and beliefs and the same superficial defects in their therapy. When someone bestows our private truths on us through the prism of their apperceptive mass, failure must follow. They are essentially treating themselves. To think that we can even guess what lies deeply buried in us is a delusion.
Consciousness means connection; it means fluid attachment to lower brain levels; it means access to our feeling base so we have feelings as part of our armamentarium, so we are guided by our feelings and not just our top level neocortical awareness. It means seeing in depth the pain and feelings of others; our children, spouses and friends. It means we are passionate and empathic. We can live the feeling life.
If we are not connected to what is driving us and making us act the way we do, we only access to ideas and beliefs and not what truly makes us human. Awareness keeps us disconnected, yet is the darling of intellectual therapists. Because it rides above and beyond feelings. Therapy then becomes some kind of game or exercise lauded by those who live in that upper zone, those instantly attracted each new phase of enhanced awareness. Hey, there is a large world down there that exists even when we cannot easily see it. Fortunately and unfortunately we can never see it till we feel it and we cannot do that until we can access our feelings. And we can never do that until we realize finally, that there is a world deep down that is the source of so much of us, our behavior and afflictions.
How to convince unfeeling people that there are feelings? It seems to be true that when they suffer and are close to feelings they rush to us for answers; and we have them: feelings. Evolution of our prefrontal cortex was preceded long before we had reason by a non verbal brain. Now that we have it, let’s steer it in the right direction and liberate ourselves.
Awareness is a late-comer to this enterprise; let us not evade the feelings that can free us. We cannot be anxious and conscious. Consciousness is the end of anxiety because we are finally in touch with its source. No one can do better than that.
It has waited a very long time to breathe the air, to become conscious where all three brains coalesce to make us conscious. Its unceasing roiling below has exhausted it and us and worn down the biologic system. The system is designed not to permanently hide feelings but to bring them up when the system can take it and integrate it. To see the faces of those who have reversed the imprint is to see a face of great relief, openness and joy. Some call it , “getting that monkey off the back” which means unloading Pain. No awareness can accomplish that because it cannot lift the Primal load, cannot unburden us and liberate us from our Primal Chains. Awareness was never meant to plunge to the depths; that is only the role of consciousness. Consciousness means reaching the deepest levels of the brain where the greatest terror and pain reside. We cannot get well with only half a brain at work. We cannot get well when half of our evolution is neglected and not considered part of us. But until we are fully ready, awareness can help mask our pain as we go through the motions of getting better which will forever be an elusive target. We cannot get there from here. Cannot get well looking at the brain from on top and believing we are treating the whole person, whereas we are treating the person’s later life, the slim slice of life that came along after many of the imprints were laid down.
Don’t think psychotherapy, insight therapy and psychoanalysis can escape; they suffer from the same rationales and beliefs and the same superficial defects in their therapy. When someone bestows our private truths on us through the prism of their apperceptive mass, failure must follow. They are essentially treating themselves. To think that we can even guess what lies deeply buried in us is a delusion.
Consciousness means connection; it means fluid attachment to lower brain levels; it means access to our feeling base so we have feelings as part of our armamentarium, so we are guided by our feelings and not just our top level neocortical awareness. It means seeing in depth the pain and feelings of others; our children, spouses and friends. It means we are passionate and empathic. We can live the feeling life.
If we are not connected to what is driving us and making us act the way we do, we only access to ideas and beliefs and not what truly makes us human. Awareness keeps us disconnected, yet is the darling of intellectual therapists. Because it rides above and beyond feelings. Therapy then becomes some kind of game or exercise lauded by those who live in that upper zone, those instantly attracted each new phase of enhanced awareness. Hey, there is a large world down there that exists even when we cannot easily see it. Fortunately and unfortunately we can never see it till we feel it and we cannot do that until we can access our feelings. And we can never do that until we realize finally, that there is a world deep down that is the source of so much of us, our behavior and afflictions.
How to convince unfeeling people that there are feelings? It seems to be true that when they suffer and are close to feelings they rush to us for answers; and we have them: feelings. Evolution of our prefrontal cortex was preceded long before we had reason by a non verbal brain. Now that we have it, let’s steer it in the right direction and liberate ourselves.
Awareness is a late-comer to this enterprise; let us not evade the feelings that can free us. We cannot be anxious and conscious. Consciousness is the end of anxiety because we are finally in touch with its source. No one can do better than that.
February 18, 2017
My Life: Practicing Primal Therapy
Because of my divorce dictum (I was going to call it an agreement), I could no longer practice in an English speaking country. My French wife, France, and I moved to Paris and opened a French clinic which was packed from the first day. We began our research program in London and flew blood samples back and forth from Paris. We studied the immune system and natural killer (NK) cells to see what happened in therapy. After one year the NK cells grew very fast. These were the cells to survey the system. As soon as a cancer cell began its life, the NK cells searched them out and killed them. Maybe that was why we saw so little cancer in our advanced patients. We studied other aspects as well. We found that body temperature dropped after one year of Primal Therapy, as well as heart rate and blood pressure. Clearly, as we took out internal pain the system was no longer lumbering under heavy pressure. Most importantly, there was the one degree drop in body temperature, which told us that maybe longevity is increased as the system’s workload lessened. There is a theory that for every one degree enduring drop in body temperature, there is a corresponding increase in longevity.
Europe became a heavy load with a five story building running night and day. Patients came from Europe, by and large, and stayed much longer back then because there were far less Visa restrictions to force patients out. Now in the USA, they are limited, which slows their therapy considerably. We treated a wide range of patients from ambassadors to a sort of terrorists, who were not that at all. They claimed to be revolutionists but they were the kindest and smartest people I met. We did therapy in several languages and it was really a polyglot group. We did research with several universities and it was all exciting stuff.
We had the clinic in a giant building in Paris, with an old fashion bathtub in the basement. France was treating a 65 year old doctor who never left her village. Why? Because she was a bed better and was so ashamed of it. France had a hunch, and took her down below into the bathtub. She gave the doctor orders to totally relax and let herself go in the tub. She did, and what happened? She urinated. Only now she felt what it was all about: it was the only warmth she ever felt. Soon after, we received postcards from her from all over the world. She was free. No more neurosis.
Here is an example to emphasize how we are a therapy of experience and not of ideas. We had a male patient obsessed with women’s feet and shoes. Our male therapist painted his nails, wore shorts and had the patient sit looking at his feet as he dangled them. Every time the patient tried to touch his feet, the therapist abruptly drew his feet away. Soon the patient was crying and screaming, “Mommy, Mommy, let me touch you.” His mother was a seamstress who did her work in front of her child. She never touched him but he watched her, transfixed, aching to touch her. She kicked him away as a pest, over and over again. His need continued to grow until it was acted out in the street or peering through windows, risking arrest. He finally resolved this act-out after much therapy. The need to be hugged and caressed, that was the simple answer. The force of his original need became the force behind his importuning obsession. The failed effort is usually an attempt to stop the symbolic acting-out. It is an effort to change and block a symbol of the need, not the basic biologic need itself. In every act-out, we must go much deeper to find that need and deal with it. That is what is biologic and real.
In a way our therapy is simple: find the basic biologic need and relive how it was not fulfilled. But Oh My! It is so much more than that. Those needs are sequestered by a labyrinth of defenses and are difficult to find. First we need to deal with how the need is ramified as to be unrecognizable. We have to find ways to dig out the essence of the feeling. The complexities became, duh……complex. Neurosis dies hard.
In group, I sometimes had die-hard atheists pray to God for fulfillment: “hold me, cherish me, love me.” Why God? Because I was after the need, and God became the channel for need. I had to find a neutral channel for patients to express need. Once they get to need, even the atheists crumble in tears because that is where the tears lie hidden. Otherwise they would see the faces of the parents whom they were importuning, and grow cold and feelingless. Anent the act out, some patients refuse to do what is necessary to get well: stop medication, start medication, whatever. If we stay hung up on their bad behavior, we will never get to what is real: “I am hopeless and cannot be helped. What’s the use? I am a failure. No one can help me.”
My education began in France with my new French family. We lived high above Aix en Provence, overlooking a beautiful city. They only spoke French to each other, and I decided I would never let it happen again, that I would never be left out of esoteric and fascinating discussions. I learned French and took part in conversations, and it was erudite and informational as I ever knew. I never had a family and this was certainly an example of what was missing. I learned French fast because now I had someone to talk to but it was not in my natal (Maternal) language. A small impediment.
I soon led the French life, reading French magazines and watching French TV, which I do to this day. Nearly all of our friends were French and among them some creative and intelligent people. I do not plan to name drop but our pals were in many of the arts and I was so proud of them, including an actress whom I saw mostly nude in a film when I was in high school. Years later she lived with us and as happens in France there was much nude swimming. Sometimes I thought I was dreaming. But no. I was just living in a sane and non-prudish country, France. Many of the public beaches were nudist. All healthy and non pejorative. Non moralistic. There were many examples of this throughout France.
After years in France, I got permission to practice in the USA so we returned to America. France’s health was breaking from the load of patients in Paris and she needed a long rest, which she got. We opened a small training center in Santa Monica which blossomed again into a major worldwide clinic, the majority of patients from Europe. I am in my nineties now and am cutting back but I still write books and the blog every day.
There are still hundreds of pretenders throughout the world using my name and my therapy to mislead patients, usually with bad results. They have my books on their desks and to all appearances they are associated with me… Without a day’s training. That is why it is always best to check with us as to who is qualified and who is not.
Europe became a heavy load with a five story building running night and day. Patients came from Europe, by and large, and stayed much longer back then because there were far less Visa restrictions to force patients out. Now in the USA, they are limited, which slows their therapy considerably. We treated a wide range of patients from ambassadors to a sort of terrorists, who were not that at all. They claimed to be revolutionists but they were the kindest and smartest people I met. We did therapy in several languages and it was really a polyglot group. We did research with several universities and it was all exciting stuff.
We had the clinic in a giant building in Paris, with an old fashion bathtub in the basement. France was treating a 65 year old doctor who never left her village. Why? Because she was a bed better and was so ashamed of it. France had a hunch, and took her down below into the bathtub. She gave the doctor orders to totally relax and let herself go in the tub. She did, and what happened? She urinated. Only now she felt what it was all about: it was the only warmth she ever felt. Soon after, we received postcards from her from all over the world. She was free. No more neurosis.
Here is an example to emphasize how we are a therapy of experience and not of ideas. We had a male patient obsessed with women’s feet and shoes. Our male therapist painted his nails, wore shorts and had the patient sit looking at his feet as he dangled them. Every time the patient tried to touch his feet, the therapist abruptly drew his feet away. Soon the patient was crying and screaming, “Mommy, Mommy, let me touch you.” His mother was a seamstress who did her work in front of her child. She never touched him but he watched her, transfixed, aching to touch her. She kicked him away as a pest, over and over again. His need continued to grow until it was acted out in the street or peering through windows, risking arrest. He finally resolved this act-out after much therapy. The need to be hugged and caressed, that was the simple answer. The force of his original need became the force behind his importuning obsession. The failed effort is usually an attempt to stop the symbolic acting-out. It is an effort to change and block a symbol of the need, not the basic biologic need itself. In every act-out, we must go much deeper to find that need and deal with it. That is what is biologic and real.
In a way our therapy is simple: find the basic biologic need and relive how it was not fulfilled. But Oh My! It is so much more than that. Those needs are sequestered by a labyrinth of defenses and are difficult to find. First we need to deal with how the need is ramified as to be unrecognizable. We have to find ways to dig out the essence of the feeling. The complexities became, duh……complex. Neurosis dies hard.
In group, I sometimes had die-hard atheists pray to God for fulfillment: “hold me, cherish me, love me.” Why God? Because I was after the need, and God became the channel for need. I had to find a neutral channel for patients to express need. Once they get to need, even the atheists crumble in tears because that is where the tears lie hidden. Otherwise they would see the faces of the parents whom they were importuning, and grow cold and feelingless. Anent the act out, some patients refuse to do what is necessary to get well: stop medication, start medication, whatever. If we stay hung up on their bad behavior, we will never get to what is real: “I am hopeless and cannot be helped. What’s the use? I am a failure. No one can help me.”
My education began in France with my new French family. We lived high above Aix en Provence, overlooking a beautiful city. They only spoke French to each other, and I decided I would never let it happen again, that I would never be left out of esoteric and fascinating discussions. I learned French and took part in conversations, and it was erudite and informational as I ever knew. I never had a family and this was certainly an example of what was missing. I learned French fast because now I had someone to talk to but it was not in my natal (Maternal) language. A small impediment.
I soon led the French life, reading French magazines and watching French TV, which I do to this day. Nearly all of our friends were French and among them some creative and intelligent people. I do not plan to name drop but our pals were in many of the arts and I was so proud of them, including an actress whom I saw mostly nude in a film when I was in high school. Years later she lived with us and as happens in France there was much nude swimming. Sometimes I thought I was dreaming. But no. I was just living in a sane and non-prudish country, France. Many of the public beaches were nudist. All healthy and non pejorative. Non moralistic. There were many examples of this throughout France.
After years in France, I got permission to practice in the USA so we returned to America. France’s health was breaking from the load of patients in Paris and she needed a long rest, which she got. We opened a small training center in Santa Monica which blossomed again into a major worldwide clinic, the majority of patients from Europe. I am in my nineties now and am cutting back but I still write books and the blog every day.
There are still hundreds of pretenders throughout the world using my name and my therapy to mislead patients, usually with bad results. They have my books on their desks and to all appearances they are associated with me… Without a day’s training. That is why it is always best to check with us as to who is qualified and who is not.
February 16, 2017
Why Primal Therapy Needs No Doctor
I write this is as an academic hall of fame in psychology and with years of psychology training and years of training in psychiatric social work. Plus an extra year of post-graduate internship in psychiatric social work. So I have an idea of what is involved. The whole training system needs to be junked and brought up to date with modern science. Right now, it is not a science that can make people well. It is a lot of tinkering, much of which I did in my earlier years on staff at hospitals and clinics. Now the powers that be are making it impossible to master any kind of science. They believe by adding more years of classes, and internships, and lectures, it will somehow build into a cure. I believe it will not, and just be busy work to make it look like a science, which it isn’t. The requirements for a license now are prohibitive and ineffective. It makes students jump through hoops, which are simple impediments to learning. The most advanced of my trainees were the Ph.D candidates. All of whom failed training because they were so intellectual and had their feelings ground out of them. They could not sense when to make a move with a patient and how to do it. It became “mental” illness for them with feelings left behind. They learned to treat patients with insights and rationales with no understanding of brain science. Worse, with no idea about the role of feelings in neocortex function, which in therapy is crucial. Making it difficult is not the same as making it understandable and treatable. And piling on more ethics courses will not help. Normal therapists are ethical, by definition. The failures were the ones who were unethical, trying sometimes to be the patient’s friend and pal, instead of his doctor. So what do we need? A feeling therapist, first and foremost. Then a minimum of brain science, then some biochemistry to see how neurosis works in the body. But the tool is the therapist and he has to be sensitive to the patient’s feelings and needs and his deep-lying imprints. I have confirmed that over fifty years of training to see who can treat and who cannot. It is never the people in their head who can help and cure; it is those who are connected to their feeling centers. Just the opposite of today’s training in psychiatry and psychology. I am poster boy #1. What I learned almost never helped me do therapy and certain never helped me understand what a cure involved. It never help me get to my feelings; they were mostly afterthoughts. For 100 years now, it is still about insights and reasons and explanations. So what is wrong with that? An outside doctor can never tell what is inside a patient because he learns from his system, above all. As feelings come up, he is informed what forces he has been hiding and what has driven him all these years. No foreign expert can do that because the expert and the only expert is the patient. For the patient, it is a crime to rob him of his epiphanies, his sole discoveries and his new ability and power to change himself. He knows what upcoming feelings can be approached, and what feelings must lie quiescent for the moment. He knows what feelings can be overloading and produce the deadly abreaction. And if an outsider pushes him, what he gets too often is abreaction because an outsider cannot know when the patient is ready for the descent into the lower depths of the brain. And that is what we don’t need ,well trained intellectuals who cannot sense what the patient can take and cannot take. If we can off our narcissism for a minute and make psychotherapy patient centered and not doctor centered, where he is not the owner of the domain of the cognoscenti but also a learner of the human condition, then we see no need for the phalanx of specialists who know everything about this symptom or that, but nothing about the internal life of the patient. We then have a cabal of those who ignore deep history of the patient, deep history of his very early key life and the history, not of his intellectual development but that of his emotions. We need to study the whole human, not in the booga booga Holistic Therapy sense, but of the dynamic interactions of all of his systems, not the least of which is his brain. I think that is what training and supervision in the Primal world is all about, and after many decades we do get neurochemical change. We do get cure, as I define it as in behavior and in medical normalization. That is a lot but I cannot deny the results we get, and today they are awesome. Remember, a tough school does not necessarily mean a good school. It is just tough; a school for masochists where upon graduation they hand you your diploma wrapped in a sculpture of your neo-cortex, with testicles hanging and with a note: good luck.
February 13, 2017
Changes and Alterations in Biochemical Functions During Primal Therapy Treatment
Here is a current patient retelling his overall changes and alterations in biochemical functions. It is not enough to relate numbers but also changes that accompany those changes. Changes can be exaggerated to please the doctor so we need corroboration, and external measures as well.
We have studied vital signs changes, especially body temperature which is a measure of the continuing work of the body. Lower temperature that endures means far less work of the whole system. That can mean enhanced longevity according to some related studies.
When all signs drop together, we have a system change, very important. Vital signs are just that: signs of the vitality of the system.
When we pair his life changes with objective measures, we are confident of his improvement. He is enjoying his life. Isn't that the goal of what we do? No pain but joy. Unfortunately, we must go through pain to get to joy: the dialectic.
All those signs combined augur well for increased longevity.
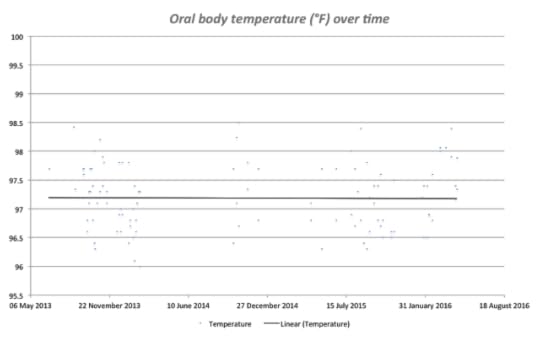
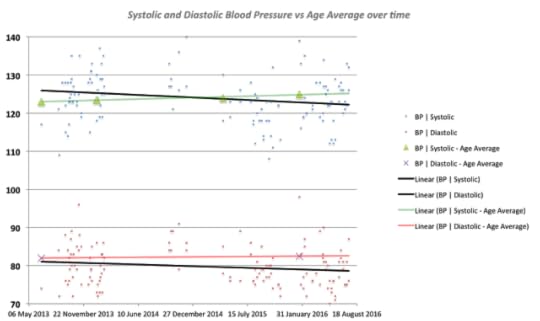
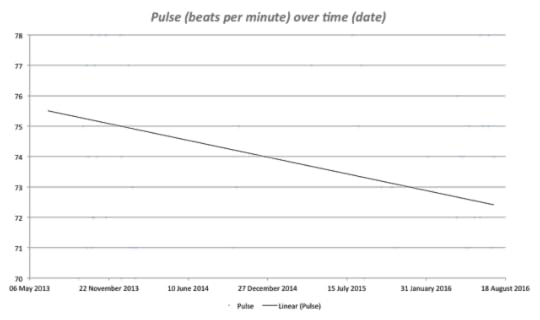
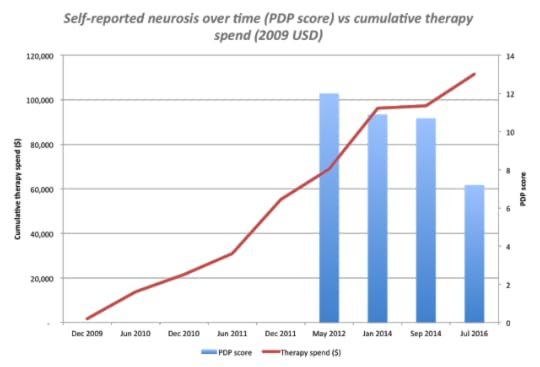
Here is the patient's interpretation, in his own words.
p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 15.0px; font: 14.0px Arial} span.s1 {font-kerning: none} I spent a bit of time extracting my Skype history to create some charts of my vitals from June 2013 to the present time.
My main conclusions:
- My blood pressure has dropped relative the age average- My pulse has dropped relative to the age average- My temperature has been constant and below the age average
At least for BP and pulse, my case appears consistent with others that Art has mentioned where vital signs get 'healthier' over time with therapy.
I have also been intermittently taking Dr Ingeborg Bosch's Personal Defense Profile Test as an indicator of neurosis, albeit self-reported of course. I've plotted my scores on this vs my investment in therapy. My defenses have also trended downwards with increasing investment in therapy.
All in all, this concurs with how I feel these days: more centered, less compulsive, more mature, more masculine.
Thank you all once again for your contribution to my transformation. Long may it continue!
It's been an extraordinary transformation - beyond anything I could have imagined in my first interview in December 2009.
My sexuality has changed fundamentally, my relationships with women have completely transformed. I have a very different personality.
The vital signs do tell a story, but it's really about the emergence of a different human being. It's as if a new version of me has arisen and taken over the body of the "old XXXXX".
I've gone from being sick, confused and under-confident, to someone striding out through the world, loving who they're being. Well most of the time! What a ride Art. What a ride.p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 15.0px; font: 14.0px Arial} p.p2 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 15.0px; font: 14.0px Arial; min-height: 16.0px} p.p3 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 20.0px; font: 14.0px Arial; min-height: 16.0px} p.p4 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 14.0px; font: 14.0px Arial} p.p5 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 14.0px; font: 14.0px Arial; min-height: 16.0px} span.s1 {font-kerning: none} span.s2 {text-decoration: underline ; font-kerning: none; color: #196ad4}
We have studied vital signs changes, especially body temperature which is a measure of the continuing work of the body. Lower temperature that endures means far less work of the whole system. That can mean enhanced longevity according to some related studies.
When all signs drop together, we have a system change, very important. Vital signs are just that: signs of the vitality of the system.
When we pair his life changes with objective measures, we are confident of his improvement. He is enjoying his life. Isn't that the goal of what we do? No pain but joy. Unfortunately, we must go through pain to get to joy: the dialectic.
All those signs combined augur well for increased longevity.
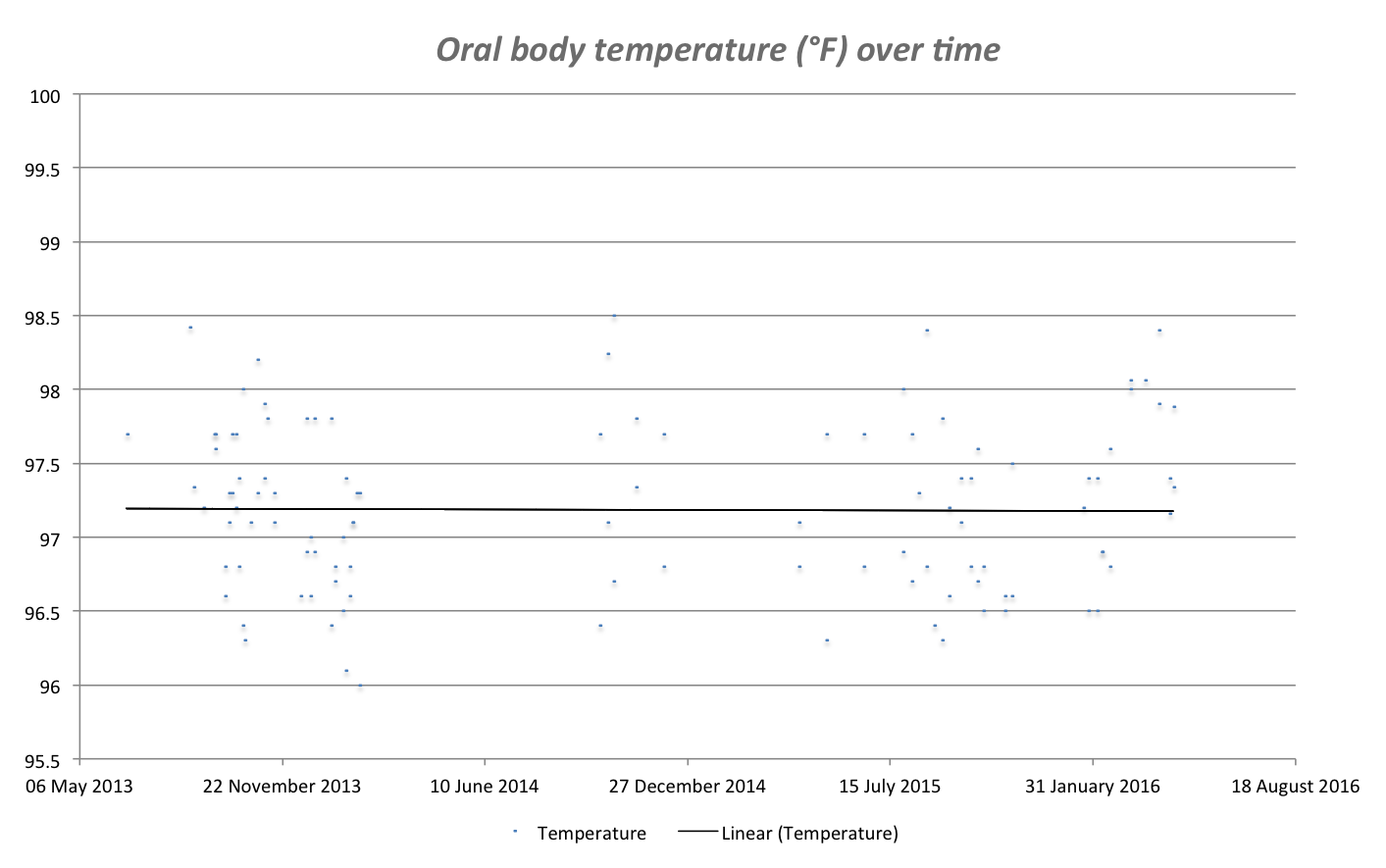
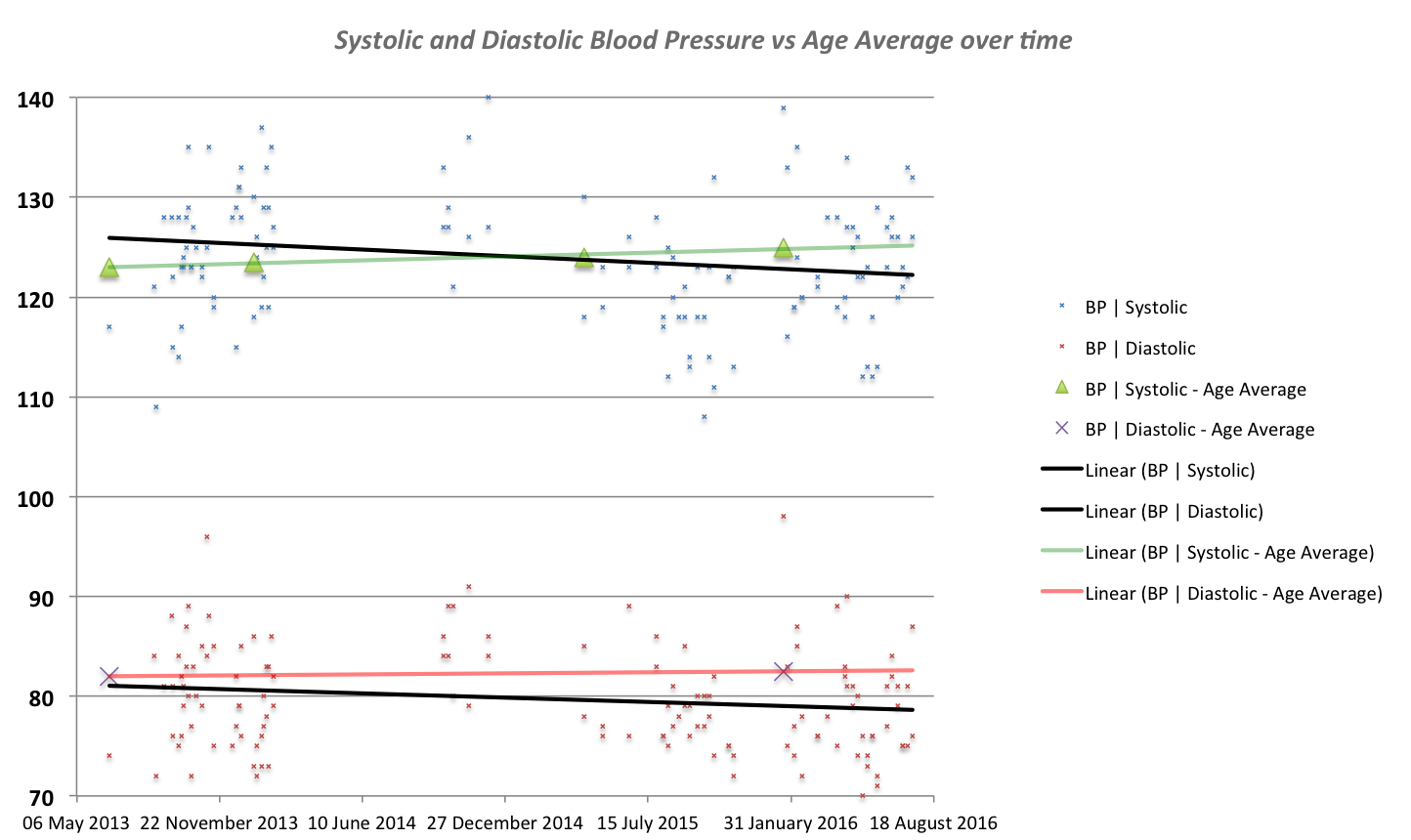
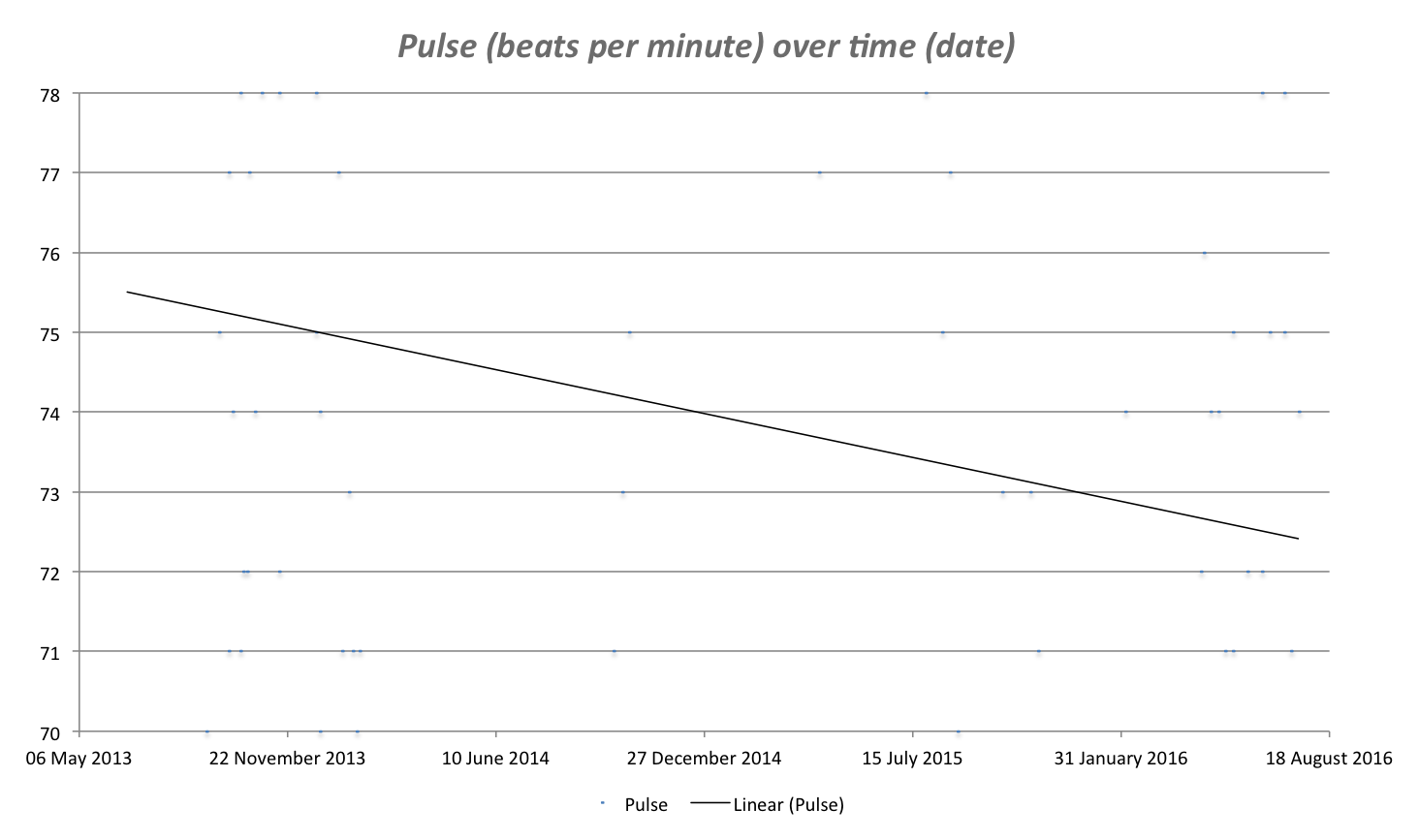
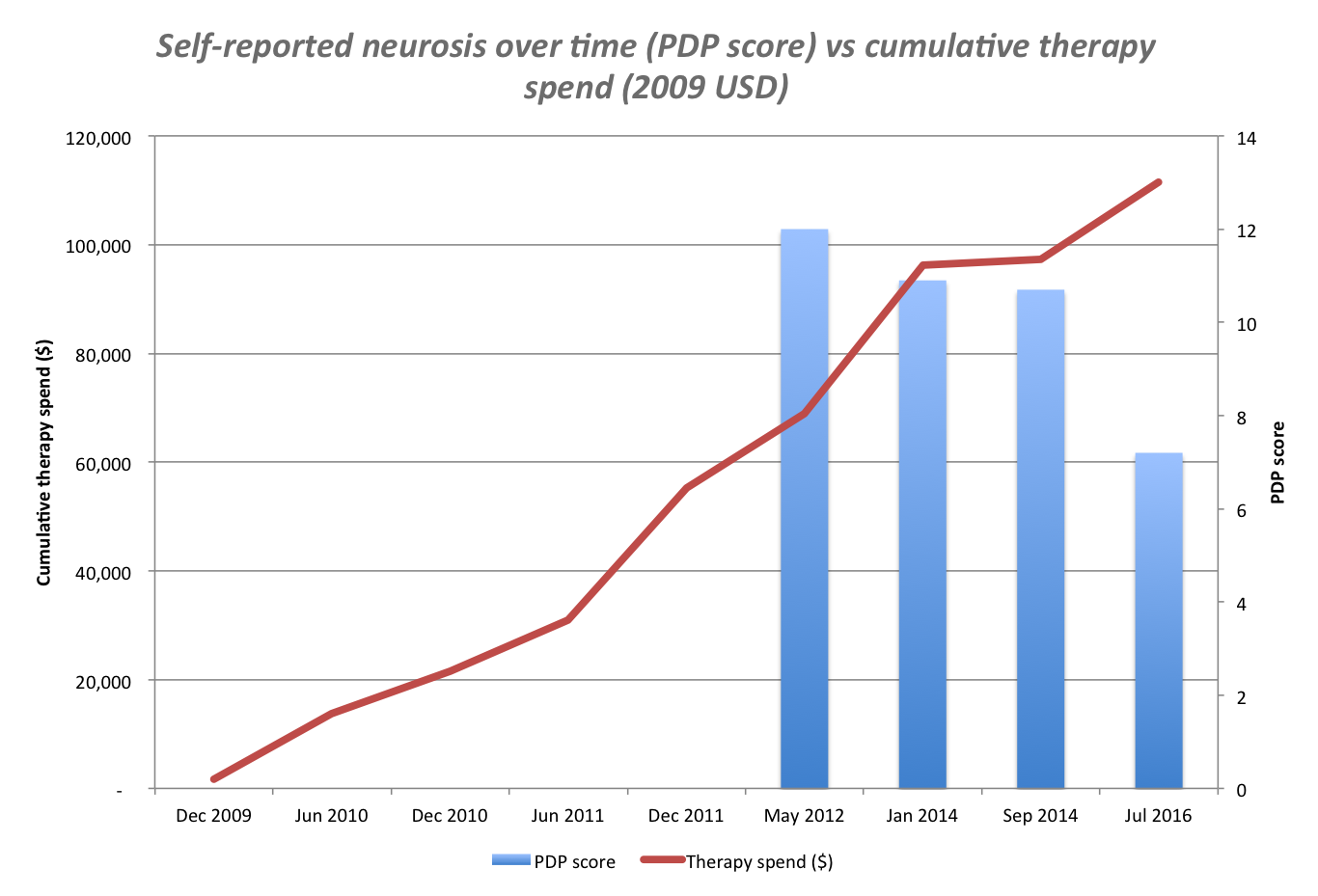
Here is the patient's interpretation, in his own words.
p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 15.0px; font: 14.0px Arial} span.s1 {font-kerning: none} I spent a bit of time extracting my Skype history to create some charts of my vitals from June 2013 to the present time.
My main conclusions:
- My blood pressure has dropped relative the age average- My pulse has dropped relative to the age average- My temperature has been constant and below the age average
At least for BP and pulse, my case appears consistent with others that Art has mentioned where vital signs get 'healthier' over time with therapy.
I have also been intermittently taking Dr Ingeborg Bosch's Personal Defense Profile Test as an indicator of neurosis, albeit self-reported of course. I've plotted my scores on this vs my investment in therapy. My defenses have also trended downwards with increasing investment in therapy.
All in all, this concurs with how I feel these days: more centered, less compulsive, more mature, more masculine.
Thank you all once again for your contribution to my transformation. Long may it continue!
It's been an extraordinary transformation - beyond anything I could have imagined in my first interview in December 2009.
My sexuality has changed fundamentally, my relationships with women have completely transformed. I have a very different personality.
The vital signs do tell a story, but it's really about the emergence of a different human being. It's as if a new version of me has arisen and taken over the body of the "old XXXXX".
I've gone from being sick, confused and under-confident, to someone striding out through the world, loving who they're being. Well most of the time! What a ride Art. What a ride.p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 15.0px; font: 14.0px Arial} p.p2 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 15.0px; font: 14.0px Arial; min-height: 16.0px} p.p3 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 20.0px; font: 14.0px Arial; min-height: 16.0px} p.p4 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 14.0px; font: 14.0px Arial} p.p5 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 14.0px; font: 14.0px Arial; min-height: 16.0px} span.s1 {font-kerning: none} span.s2 {text-decoration: underline ; font-kerning: none; color: #196ad4}
February 10, 2017
Why Does Primal Therapy Take Time?
Because we are undoing and redoing your life? Because we are opening up the gates of repression and allowing access to deeply embedded pain? Because we need to open the gates slowly so that the patient is never overwhelmed by what is buried down below. It takes skills and patience. It is so easy to open the patient up and get dramatic results; results that resemble a primal but are largely a release of the pressure of the feeling without its content. It feels good and can fool the patient and the doctor. I teach all of the time how to avoid all this and keep the patient sane.
When we reach down into the unconscious that predates words and feelings and parallels the archaic brain, we are touching on a primitive brain that deals in impulses and reptilian movements. It emanates from millions up millions of years ago with a brain that can be rageful, or terror ridden, and ultimately can register deep hopelessness labeled as suicidal depression. It is largely the brainstem and the lower reaches of the nervous system. It is an area that takes great care and does not support a booga booga approach, where anything goes.
We adhere to science and facts and try not to concoct theories that do not correspond to reality. Remember we are attempting to put together a disconnected brain system where nervous impulses were severed from their counterpart so that feelings had little or no access to corresponding ideas and beliefs. Feelings stopped being a guide for behavior and left the person bereft of guidelines.
When we reach down into the unconscious that predates words and feelings and parallels the archaic brain, we are touching on a primitive brain that deals in impulses and reptilian movements. It emanates from millions up millions of years ago with a brain that can be rageful, or terror ridden, and ultimately can register deep hopelessness labeled as suicidal depression. It is largely the brainstem and the lower reaches of the nervous system. It is an area that takes great care and does not support a booga booga approach, where anything goes.
We adhere to science and facts and try not to concoct theories that do not correspond to reality. Remember we are attempting to put together a disconnected brain system where nervous impulses were severed from their counterpart so that feelings had little or no access to corresponding ideas and beliefs. Feelings stopped being a guide for behavior and left the person bereft of guidelines.
February 9, 2017
The Joy and Tragedy of a Wide Open Gate
So I was sitting in the garden yesterday and I heard a rustling in the other side in the brush. I hurried there to find my cats killing a baby rabbit. With his last breath, the rabbit raised his paw to say, "I am dying, don’t hurt me anymore." At this point, I fell off my stool and had a giant Primal. It was the leitmotif of my life. I raised my hand and cried and begged, "Don’t hurt me anymore." It formed my weltanschauung, my outlook, and philosophy of living. It became my personality, but I never knew it. I was excessively sweet, kind, and gentle, acting out, "Don’t hurt me anymore," since when my dad started beating me with a fury when I was five or six. I never even knew how it shaped who I was and I never knew I needed to scream, "Do not hurt me anymore." I never knew it because he was unrelenting and was a stone who could never understand his hurt of me, or even that he was hurting me all of the time. It was, “all of the time,” because it became an imprinted feeling that could never let me go of it. I could not get over it because that memory was embedded and part of me. I acted it out in my deep unconscious, "Don’t hurt me anymore." It was now my personality, and I was sweet and submissive so he would stop hurting me. It never happened. Because he never wanted me. I was an accident and he made me suffer for intruding into his life and creating more responsibility.
The image of the rabbit raising his paw to say, "I give up. Please don’t hurt me," led me to a feeling I never knew I had; it was same as that rabbit. My mother was psychotic and could not understand the hurt she brought on her children, and my father was a chronically angry tyrant who could not be mollified. He had no capacity for pity. No ability to empathize with the hurts of his children. They sent me to a hospital for weeks, almost never visiting and never saying that I was in line for a difficult surgery. I was shocked when I was wheeled into the operating room and had no one to explain or reassure me, to soften the blow. And still they did not visit. That is the kind of hurt that was a daily occurrence. I could not raise my hand to utter the plea, "STOP!" It was something they could never understand. Worse, it was something I could not understand. That total neglect seemed everyday to me. It was what parents do. That is how I learned: do the opposite of everything they did and said. I am the opposite of them, illiterate, never any interest in anything, no culture nor education. I often joked that I was an orphan with parents and I now learn how true that was and is.
My daily personality, as my patients and therapists tell me, was sweet and kind; it was the chronic act out, "don’t hurt me anymore," even though I never knew I was hurting. The rabbit taught me to raise my hand to stop the torture. I do it now in my Primal, but the feeling is still built in. I will never be a tyrant or mean. My father beat the meanness out of me. He taught me to give in, to cede and not fight. And clearly, never talk back. My parents' whims were my destiny. I was afraid because I saw the anger in his commands, his watery and red eyes that spelled danger. That shaped my whole life. I never felt, "Love Me," in my earliest Primals. It took first til now to speak what was so awful to speak its name; "Pity, please, Pity. Mercy, I beg you, Mercy."
So an act-out is nothing external for all to see; it is encased in behavior that speaks volumes. And it speaks the truth while my neocortex never knew that truth. My act out was unconscious. So I was perceptive and unconscious. I cried heavily for that poor baby rabbit as I now cry for me as that helpless baby. My cats were not mean; it was just play for them. But so deadly. My father was the same way, creating damage through inadvertence.
The image of the rabbit raising his paw to say, "I give up. Please don’t hurt me," led me to a feeling I never knew I had; it was same as that rabbit. My mother was psychotic and could not understand the hurt she brought on her children, and my father was a chronically angry tyrant who could not be mollified. He had no capacity for pity. No ability to empathize with the hurts of his children. They sent me to a hospital for weeks, almost never visiting and never saying that I was in line for a difficult surgery. I was shocked when I was wheeled into the operating room and had no one to explain or reassure me, to soften the blow. And still they did not visit. That is the kind of hurt that was a daily occurrence. I could not raise my hand to utter the plea, "STOP!" It was something they could never understand. Worse, it was something I could not understand. That total neglect seemed everyday to me. It was what parents do. That is how I learned: do the opposite of everything they did and said. I am the opposite of them, illiterate, never any interest in anything, no culture nor education. I often joked that I was an orphan with parents and I now learn how true that was and is.
My daily personality, as my patients and therapists tell me, was sweet and kind; it was the chronic act out, "don’t hurt me anymore," even though I never knew I was hurting. The rabbit taught me to raise my hand to stop the torture. I do it now in my Primal, but the feeling is still built in. I will never be a tyrant or mean. My father beat the meanness out of me. He taught me to give in, to cede and not fight. And clearly, never talk back. My parents' whims were my destiny. I was afraid because I saw the anger in his commands, his watery and red eyes that spelled danger. That shaped my whole life. I never felt, "Love Me," in my earliest Primals. It took first til now to speak what was so awful to speak its name; "Pity, please, Pity. Mercy, I beg you, Mercy."
So an act-out is nothing external for all to see; it is encased in behavior that speaks volumes. And it speaks the truth while my neocortex never knew that truth. My act out was unconscious. So I was perceptive and unconscious. I cried heavily for that poor baby rabbit as I now cry for me as that helpless baby. My cats were not mean; it was just play for them. But so deadly. My father was the same way, creating damage through inadvertence.
February 5, 2017
On Talking Fast
In childhood I talked so fast that is was hard to understand me, and I never knew why. Then I had the key feeling. My father was so anxious that he could not sit still and pay attention. When I did have to ask him something, I sensed his impatience and hurried through it. I talked fast. He also never wanted to hear anything I said so he would find reasons to delay listening. "Can't you see I am busy?" I got punished for asking because it was never at the right time. He had no time for me.
In fact, he didn't want me around. He never addressed me unless it was a criticism: stand up straight, stop talking through your nose (I had a constant running nose). Mostly, it was “stop bothering me.” He had no time for me. The fates got him at age 63 with a giant heart attack. I began crying at home on the way to the cemetery and my mother ran out screaming, “He's crying! He's crying!” The opposite of a compassionate mother. She had no interest in acting maternal because she was a five year old and talked baby talk.
Crying became an anathema. It was nowhere in the family lexicon. I never saw either parent show any feeling in my lifetime. It was a robotic existence. But my metabolism was set to churn at the pace of their indifference. Their whims became my destiny. When they decided to move, there was no warning or explanation; just pack and get going. Talking to me was a reminder that there was a job to do: take care of me. They wanted no reminder of that.
p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 20.0px; font: 17.0px 'Helvetica Neue'; -webkit-text-stroke: #000000} p.p2 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 20.0px; font: 17.0px 'Helvetica Neue'; -webkit-text-stroke: #000000; min-height: 20.0px} span.s1 {font-kerning: none}
I slowed way down later on as I slipped into my feelings about how they had children but wanted nothing to do with them. I was an orphan with a mommy and daddy.
In fact, he didn't want me around. He never addressed me unless it was a criticism: stand up straight, stop talking through your nose (I had a constant running nose). Mostly, it was “stop bothering me.” He had no time for me. The fates got him at age 63 with a giant heart attack. I began crying at home on the way to the cemetery and my mother ran out screaming, “He's crying! He's crying!” The opposite of a compassionate mother. She had no interest in acting maternal because she was a five year old and talked baby talk.
Crying became an anathema. It was nowhere in the family lexicon. I never saw either parent show any feeling in my lifetime. It was a robotic existence. But my metabolism was set to churn at the pace of their indifference. Their whims became my destiny. When they decided to move, there was no warning or explanation; just pack and get going. Talking to me was a reminder that there was a job to do: take care of me. They wanted no reminder of that.
p.p1 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 20.0px; font: 17.0px 'Helvetica Neue'; -webkit-text-stroke: #000000} p.p2 {margin: 0.0px 0.0px 0.0px 0.0px; line-height: 20.0px; font: 17.0px 'Helvetica Neue'; -webkit-text-stroke: #000000; min-height: 20.0px} span.s1 {font-kerning: none}
I slowed way down later on as I slipped into my feelings about how they had children but wanted nothing to do with them. I was an orphan with a mommy and daddy.
Arthur Janov's Blog

- Arthur Janov's profile
- 63 followers
Arthur Janov isn't a Goodreads Author
(yet),
but they
do have a blog,
so here are some recent posts imported from
their feed.

